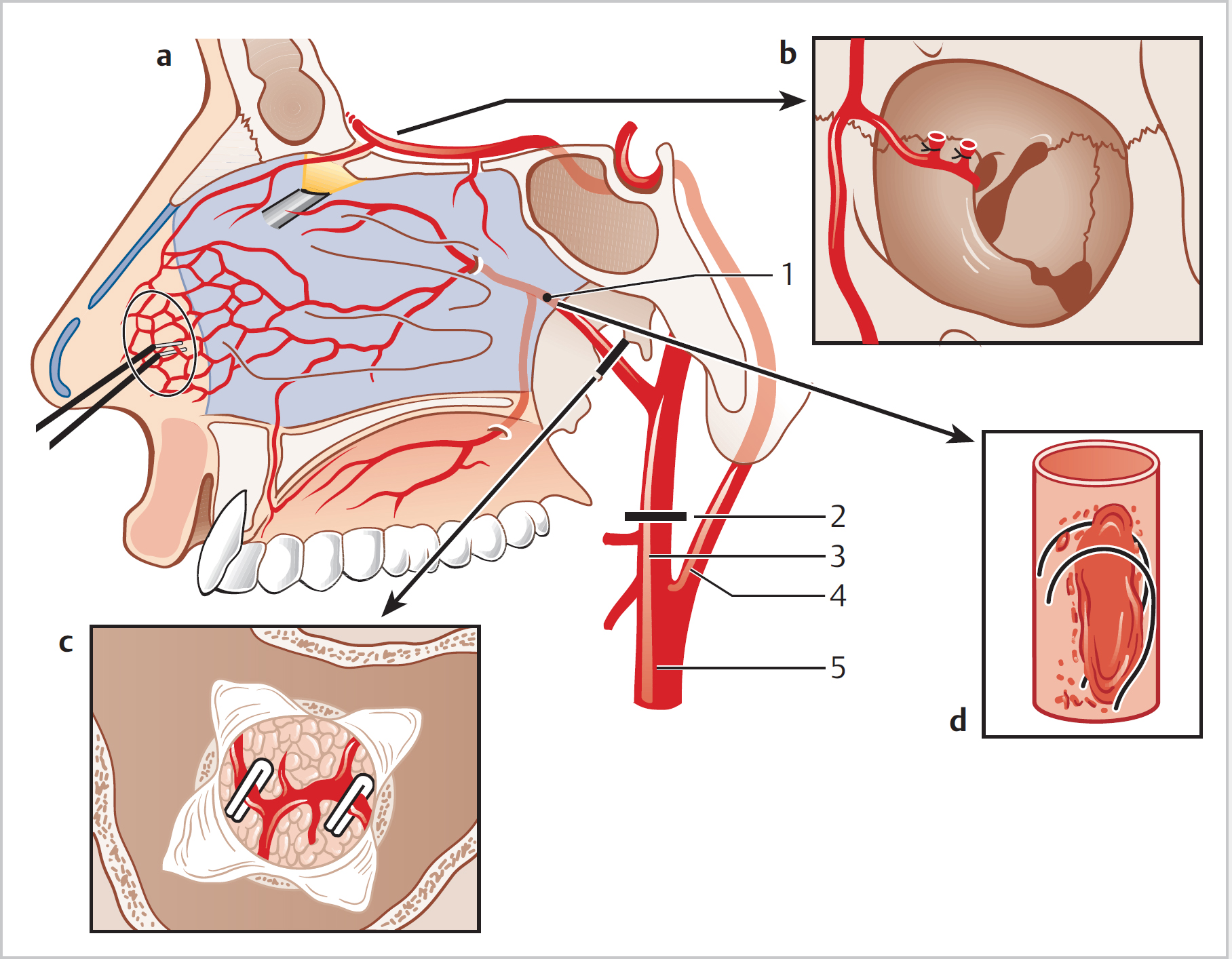
29 Epistaxis • Atherosclerosis, i.e., hypertensive patients • Anticoagulants, e.g., warfarin • Antiplatelet agents, i.e., aspirin • Trauma (inc. finger picking) • Iatrogenic (i.e., postop, inc. septal perforation) • Congenital: haemophilia, HHT • Infective: rhinosinusitis, TB, syphilis, leprosy • Inflammatory: atrophic rhinitis, granulomatous disease (e.g., granulomatosis with polyangiitis) • Metabolic: vitamin deficiency, alcohol abuse • Endocrine: pregnancy, (menstruation) • Trauma: foreign bodies • Idiopathic • Iatrogenic: chemotherapy, non-steroidal anti-inflammatory drugs, ABx • Neoplastic: any sinonasal tumour, especially lymphoma, leukaemia, widespread mets, angiofibroma, others • Bleeding dyscrasias: hepatic/renal failure, massive transfusion • In all patients: • History: • Remember ABCDE • Ensure FBC, coag, G&S for all patients admitted with epistaxis • IV fluids and O2 may well be required • Control BP • Stop anticoagulants if possible • Antibiotics if indicated (should be given when packs in place for more than 24 h) • Blood transfusion • Haematology advice • Local pressure and ice • Suction clearance • Co-phenylcaine (lidocaine + phenylephrine)/cocaine paste/other combinations of decongestant and anaesthetic • Anterior rhinoscopy ± nasendoscopy (ideally with rigid scope to allow for treatment) • Silver nitrate cautery • Packing if required—various packs available • Check oropharynx • Gold standard pack remains as BIPP gauze and Foley catheter secured with gate/umbilical clamp • Options will depend on local resources and skills available • Gold standard is now endoscopic SPA ligation (clips/diathermy) (Fig. 29.1) • Other options: – Anterior ethmoid—medial orbital incision (Lynch–Howarth); artery found 24 mm deep to orbital rim – Maxillary—via Caldwell–Luc approach or even endoscopically – Ext. carotid—ligated in the neck • Performed endoscopically • Can be under LA or GA; infiltration of the sphenopalatine foramen should be performed regardless of anaesthesia given
29.1 Aetiology
29.1.1 Common Conditions
29.1.2 Uncommon Conditions
29.1.3 Assessment
 Check ABC, cardiovascular status
Check ABC, cardiovascular status
 Site, frequency, and duration of epistaxis.
Site, frequency, and duration of epistaxis.
 Aspirin/warfarin/bleeding disorders
Aspirin/warfarin/bleeding disorders
 Possibility of trauma
Possibility of trauma
 Hypertension, alcohol consumption
Hypertension, alcohol consumption
29.2 Management/Examination
29.2.1 General Measures
29.2.2 Specific Measures
29.2.3 Surgical Measures
 EUA, cautery with BPD/silver nitrate and repacking (± PNS pack)
EUA, cautery with BPD/silver nitrate and repacking (± PNS pack)
 Septoplasty
Septoplasty
 Embolization
Embolization
 Ligation of other arteries (Fig. 29.3)
Ligation of other arteries (Fig. 29.3)
29.3 Sphenopalatine Artery Ligation
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


