OVERVIEW
- Epistaxis in children behaves differently from adult epistaxis
- Epistaxis in adults can be life threatening
- Unusually severe or persistent bleeding should initiate a search for secondary factors (e.g. haematological investigations)
- Primary and secondary epistaxis are different conditions requiring different management strategies
- Continued epistaxis following trauma must be referred to ENT
- Direct (bleeding point specific) therapy reduces hospital stay and morbidity
- Continued bleeding after insertion of a tampon should be seen as an indication to move to the next level of management, e.g.surgical ligation or embolisation
Epistaxis or nosebleeds occur in patients of any age and their severity can range from minor, nuisance bleeds to life-threatening bleeding requiring hospitalisation and surgical treatment. Epistaxis is the commonest reason for adult emergency admission to an ENT ward and it is a condition with a significant morbidity and risk of mortality. The quality of the initial and subsequent management of acute epistaxis can determine whether patients are effectively cured and discharged from hospital or whether they suffer continued bleeding and morbidity after invasive and ineffectual therapies (Figure 13.1).
Figure 13.1 Patient showing the traumatic nature of poor management of an acute adult epistaxis. The nose has been packed with gauze, Foley catheters have been inserted and despite, or perhaps because of, this she continues to bleed but is now also hypoxic and severely traumatised. How not to do it!

The clinical types of epistaxis can be classified according to the scheme outlined in Box 13.1.
- Primary (no obvious causal factor, the majority of cases)
- Secondary (due to an identifiable cause)
- Childhood
- Adult
- Acute
- Recurrent
Aetiology
The causes of epistaxis are poorly understood and most can be considered idiopathic. Cases can, however, be grouped broadly as either primary or secondary. The majority of bleeds fall into the primary category where no obvious cause is identified. Secondary epistaxis is due to a readily identifiable factor such as one of those outlined in Box 13.2. These secondary factors should always be checked for when taking the history. Rare causes such as tumours, hereditary haemorrhagic telangiectasia and juvenile nasopharyngeal angiofibroma are discussed later in this chapter but must be borne in mind as a high index of clinical suspicion is vital if these uncommon causes are not to be missed among the vast predominance of primary cases.
- Alcohol
- Aspirin and non-steroidal anti-inflammatory drugs
- Antiplatelet agents, e.g. clopidogrel
- Anticoagulants, e.g. warfarin
- Herbal medicines, e.g. St John’s wort, fish oil
- Blood dyscrasias, e.g. thrombocytopenia
- Coagulopathy, e.g. haemophilia, von Willebrand’s disease
- Trauma, e.g. nasal fracture
- Tumours
- Surgery
- Septal perforations
Childhood epistaxis
Nosebleeds are common in children of all ages and tend to be recurrent. Childhood epistaxis is mainly primary. They are often reported to occur at night and while the blood loss may seem alarming, it is seldom life threatening (a little blood goes a long way!). The commonest site of the bleeding vessel is on the anterior inferior part of the nasal septum in the highly vascular Little’s area (this area contains Kiesselbach’s vascular plexus). The exact aetiology is unclear but seems to involve mucosal inflammation and infection leading to blood vessel fragility. Nose picking may predispose to nasal vestibulitis, an infection caused by Staphylococcus aureus. Treatment of this chronic low-grade infection may explain the efficacy of chlorhexidine-neomycin creams in reducing the frequency of nosebleeds.
Management
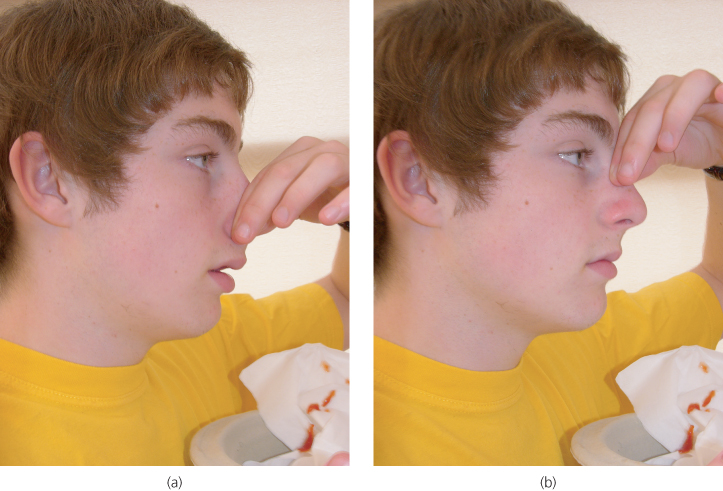
If the child is seen while actively bleeding, first aid should be instituted by pinching the nostrils using the so called Hippocratic manoeuvre. Care should be taken to ensure that firm pressure is applied over Little’s area by compressing the soft alar regions against the septum. Figure 13.2 demonstrates the correct and the surprisingly frequently observed incorrect application of this technique. Once the bleeding has stopped, the nose can be examined gently and with a good source of illumination (a head light is ideal). If a bleeding point is seen, it can be sprayed with a local anaesthetic and vasoconstrictor agent (e.g. lignocaine and phenylephrine compound spray). Chemical cautery using silver nitrate on an applicator stick or diathermy with a bipolar electrode can then be applied to the vessel to control the bleed and to prevent recurrences. Care should be taken to apply the cautery only to the exact spot as a generalised application of silver nitrate can lead to further inflammation and infection and carries a risk of causing a septal perforation. Bilateral cautery should be avoided as it is seldom required and also increases the risk of a perforation. A course of chlorhexidine-neomycin cream is prescribed to prevent recurrence and promote epithelial healing. Nasal packs or tampons (see below) are almost never needed in children.
Figure 13.2 Correct (a) and incorrect (b) application of the Hippocratic manoeuvre. The soft part of the lower nose should be firmly compressed.
Adult primary epistaxis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


