Indications
Contraindications
Consideration
Fuchs’ dystrophy
Significant irreversible central corneal scarring
Large iris defects
Bullous keratopathy (aphakic or pseudophakic)
Keratoconus
Aniridia
Posterior polymorphous dystrophy
Hypotony
Glaucoma tubes
Iridocorneal endothelial (ICE) syndrome
Aphakia
Endothelial failure
Anterior chamber intraocular lenses
Failed PK
Peripheral anterior synechiae
Congenital hereditary endothelial dystrophy
Surgical Techniques
DLEK
As noted above, DLEK was never widely adopted because of its technical difficulty and unpredictable visual recovery. Although not ideal, DLEK was the first successful EK procedure. It certainly had several advantages over PK because it utilized a smaller incision and maintained the recipient’s anterior corneal surface. Visual recovery was similar to PK and the suture-related complications seen with PK were prevented.
DSEK
In DSEK, the endothelium, Descemet’s membrane, and deep stromal tissue are delivered to the posterior surface of the cornea after removing the recipient’s dysfunctional Descemet’s membrane and endothelium. The procedure comprises three steps: (a) preparation of a posterior lamellar graft, (b) removal of the host Descemet’s membrane and dysfunctional endothelium, and (c) insertion of the graft into the anterior chamber and positioning using air tamponade.
(a)
Donor preparation: The donor cornea is mounted on an artificial anterior chamber for lamellar dissection. Then it is placed on a tissue-cutting block and trephined to the desired diameter (usually 8–9 mm) from the endothelial side. Methods of lamellar dissection include:
Manual dissection (Fig. 4.1, first row) – An initial 4–5-mm curvilinear incision is made at the limbus to a depth of approximately 300–350 μm with a guarded diamond/Bevers’ blade. Short and long curved dissecting blades are used to extend the lamellar dissection 360° to reach to the limbus.

Fig. 4.1
Donor tissue preparation: equipment and methods. First row (L-R) Descemet’s stripping endothelial keratoplasty (DSEK): manual dissectors (DORC, Netherlands); Barron disposable artificial anterior chamber (Katena Products); manual dissection with donor cornea mounted on artificial anterior chamber. Second row (L-R) Descemet’s stripping automated endothelial keratoplasty (DSAEK): microkeratome (Moria); reusable artificial anterior chamber (Moria); microkeratome-assisted donor dissection; microkeratome (Gebauer, Germany). Third row (L-R) Descemet’s membrane automated endothelial keratoplasty (DMAEK) graft preparation: air is injected via a needle inserted through the peripheral scleral rim; this creates a big bubble; the big bubble is enlarged with more air to separate the Descemet’s membrane (DM) from the posterior stroma. Fourth row (L-R) Descemet’s membrane endothelial keratoplasty (DMEK) graft preparation: peripherally scored DM is separated from underlying stromal tissue circumferentially using a microfinger; DM is peeled in four quadrants leaving it attached at the center; final peel to free the center of the tissue; scrolled donor Descemet’s membrane and endothelium. Fifth row (L-R) DMEK graft insertion: trypan blue is being used to stain the DM scroll to improve visualization; the stained DM scroll; the tissue is being loaded into the cartridge of an intraocular lens inserter; the DM scroll within the inserter
Microkeratome dissection (Fig. 4.1, second row) – The donor dissection plane is created with a microkeratome. The microkeratome head depth can be selected according to the desired plane of lamellar dissection (usually 250–400 μm). Microkeratome dissection produces a smoother and more regular dissection plane compared with manual dissection. Numerous eye banks have purchased microkeratomes and provide pre-dissected tissue. The most commonly used microkeratome (Moria, Antony, France) cuts deeper in the periphery than centrally, and this somewhat compensates for the normally increased thickness of the cornea in the periphery compared with the center, usually resulting in a fairly planar posterior donor button.
Femtosecond (FS) laser dissection (FS-DSEK) – The feasibility of using a femtosecond laser to create lamellar cuts has been assessed in multiple studies. So far all have had suboptimal visual results because the laser does not produce as smooth a dissection plane in the soft posterior stroma as it does when producing a flap in the anterior stroma for laser refractive surgery. In addition, irregularities are induced in the posterior stroma when the donor tissue is applanated against a solid laser interface. Finally, the anterior corneal surface is usually used as a reference surface for the cut causing the peripheral graft to be variably thicker than the center, depending upon the thickness gradient in the donor cornea. The latter limitation could potentially be addressed with appropriately sophisticated imaging technology and laser software [26, 27]. So far, no one has been able to demonstrate that this much more expensive approach results in any tangible benefits.
(b)
Stripping of the host Descemet’s membrane (Fig. 4.2, first row – first): The host DM is removed within an area corresponding to the graft diameter or slightly smaller. DM stripping is necessary in Fuchs endothelial dystrophy to remove the guttae; however, this step may be optional in conditions where the DM is optically clear and devoid of any structural alterations, such as in failed PK and pseudophakic corneal edema [28–30].
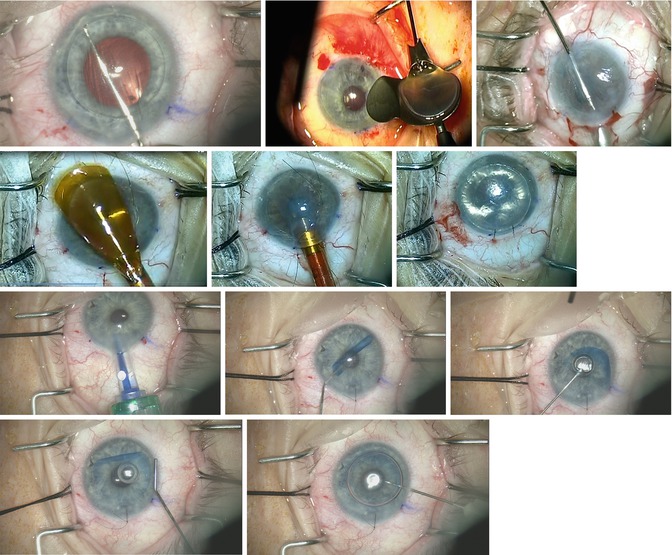
Fig. 4.2
Recipient preparation, graft insertion, and positioning. First row (L-R): Descemet’s membrane scoring; loading a DSEK graft into a Busin glide (Moria); pull-through method of graft insertion using a Busin glide and intraocular forceps. Second row (L-R): loading a DSEK graft into an EndoSerter (Ocular Systems, Winston-Salem, NC); graft insertion with EndoSerter; air tamponade. Third row (L-R): DMEK graft insertion; short bursts of balanced salt solution unfold the scrolled tissue; partial unfold achieved. Fourth row (L-R): unwrapping the scrolled DMEK donor tissue over a posterior air bubble (the air bubble helps anchor the graft in the correct position); final air injection to press the donor tissue against the recipient cornea
(c)
Graft insertion and positioning: The graft was initially inserted through a 5-mm incision using forceps; however, a number of glides and inserters have been developed to facilitate this process and help minimize damage to the tissue during insertion. The incision size has also been decreased in many cases down to 3.4 mm with curled donors. Currently used donor insertion instruments include:
Forceps – The donor tissue is folded into a 60/40 configuration (with the endothelium facing inward and protected with a small amount of viscoelastic) and inserted into the anterior chamber using atraumatic non-coapting forceps (Ex. Charlie II, Goosey, Kelman forceps) [3, 6, 7].
Sheets glide – This method can be helpful in eyes with a shallow anterior chamber and predisposed to iris prolapse. The anterior chamber is maintained using an anterior chamber (AC) maintainer. A Sheets intraocular lens (IOL) glide is inserted halfway into the chamber, which serves to keep the iris from prolapsing out of the wound. The donor graft is placed onto the glide with the endothelial side facing downward and protected with a generous amount of cohesive viscoelastic. An intraocular forceps is inserted through the site opposite to the main incision. The donor edge is grasped with the forceps and pulled inside the anterior chamber (pull-through method) [31]. Alternatively, the graft may be inserted through the main incision using a Sinskey hook or small-gauge needle (push-in method) without the use of an anterior chamber maintainer.
Busin glide (Fig. 4.2, first row – second) – This reusable funnel glide (Moria, Inc., Antony, France) curls the graft into a cylindrical shape as it is pulled through the glide to minimize endothelial trauma during insertion [32]. The leading edge of the graft is grasped and pulled into the anterior chamber with an intraocular forceps introduced through an incision opposite to the main incision (Fig 4.2 first row – third).
Suture pull-through – In this method [33], a 10-0 prolene suture is passed through a 5-mm main incision and across the anterior chamber to exit through the cornea approximately 1 mm beyond the edge of stripped DM. The donor endothelium is coated with viscoelastic, and the second arm of the suture is passed through the periphery of the donor lenticule, entering from the endothelial side and exiting from the stromal side. Both sutures are then passed through the incision, across the anterior chamber, and out through the cornea 1 mm peripheral to the edge of stripped DM. The donor lenticule is gently folded in half with the suture at the leading edge, and the anterior lip of the incision is lifted as both ends of the suture are pulled to guide the graft into the eye. The graft unfolds as the AC is filled with air, and it is secured by tying off the suture, which helps minimize the risk of graft dislocation.
After the graft is inserted, it is positioned and attached to the host posterior stroma using an air bubble (Fig. 4.2, second row – third). Complete air fill in the anterior chamber is maintained for 10–12 min, followed by a partial air-fluid exchange to avoid risk of raised intraocular pressure (IOP) secondary to pupillary block. Alternatively, a prophylactic inferior iridectomy may be made prior to graft insertion to prevent pupillary block because of air, and a 90 % air fill can be left in the eye as long as the iridectomy is not covered by air. Postoperatively, supine positioning is maintained for 15–30 min or longer.
DMEK
DMEK involves harvesting of donor DM and endothelium followed by insertion, unfolding, and positioning in the proper orientation. Just as in DSEK, the central host DM is removed before inserting the donor tissue. However while the DSEK grafts will easily stick to retained areas of the host Descemet’s membrane and endothelium, DMEK grafts stick much better to bare stroma.
(a)
Donor preparation (Fig. 4.1, fourth row): Donor DM can be isolated by direct peeling [36] or by injection of air to create a big bubble [37]. Direct peeling has a higher success rate with less endothelial cell loss [38]. Giebel and Price described a direct peeling method called submerged cornea using backgrounds away (SCUBA) that has a success rate of almost 99 % [39, 40]. Earlier reports had lower success rates, but with experience and refined technique modifications like totally freeing up the scored peripheral Descemet’s membrane before stripping, results have greatly improved. The donor corneoscleral rim is submerged with the endothelial side up in a viewing chamber filled with corneal storage solution, or it can be placed on a cutting block. The DM is lightly scored 1–2 mm inside the trabecular meshwork using a Y-hook, because peripheral DM is the area most likely to tear during edge lift due to adhesions. Trypan blue staining improves visualization of the scored edge, which is then lifted circumferentially with a microfinger (Moria, Inc.). Radial tears are identified and removed prior to edge lift with the microfinger because these tears can extend centrally. The edge of the DM is grasped with a Tubingen forceps (Ambler Surgical), while fixation of the limbus is achieved with 0.5-mm forceps. DM is partially peeled in four quadrants, leaving the center part attached (“corridor method”) – a technique which decreases tension during the peel by decreasing the width of the peel zone [41]. The membrane is floated back into position and the donor is trephined lightly into stroma. The donor is placed back in the viewing chamber for a final peel to detach DM centrally. The detached DM spontaneously forms a scroll with the endothelium on the outside. The DM scroll is placed either in the storage medium or used immediately for transplantation. The DM thickens with age; thus grafts from older donors generally scroll less tightly, which makes graft unwrapping easier during surgery. Therefore, donor tissue over 40 years of age is preferable for DMEK. As with DSEK, DMEK donor tissue can be prepared several days before the surgical procedure [42]. Other variations of donor stripping have been reported by Kruse [43] and Jardine [44], with the latter technique leaving one side of the donor attached so that the tissue can be laid back in place for endothelial cell density assessment by the eye bank.
A newer method for detaching the Descemet’s membrane with air has been termed PDEK [45]. The developer claims that this method detaches Dua’s [46] layer along with the Descemet’s membrane and endothelium, allowing use of younger donors and reportedly easier unfolding of the tissue [45]. However, donor diameters are limited to about 7–7.5 mm because of the diameter of Dua’s layer.
(b)
Graft insertion, unfolding, and positioning: The DM scroll can be loaded into a glass pipette or IOL cartridge and injector and inserted through a 2.4–3-mm wide corneal incision. Various types of IOL cartridges are suitable for graft delivery including Carl Zeiss inserters (Jena, Germany) and Viscoject (Medicel AG, Wolfhalden, Switzerland) (Fig. 4.1, fifth row). A variety of new glass tubes have also been used including the Straiko modified Jones tube for DMEK (Gunther Weiss, Portland, Oregon). Graft adhesion is reported to be better with use of a closed system without any addition of viscoelastic [47].
Several graft unfolding maneuvers are available (Fig. 4.2, third and fourth row). Dapena et al. [48] described a standardized “no-touch” technique for DMEK transplants. A glass injector is used to deliver the DMEK roll into the anterior chamber with the endothelium facing the cornea. A small air bubble is delivered between the double rolls to unfold the graft. After unfolding, the air bubble is removed, and an air bubble underneath the graft (between iris and graft) is injected for graft fixation [48]. Liarakos et al. [49] described 4 standard (standardized no-touch DMEK, Dirisamer technique, Dapena maneuver, and single sliding cannula maneuver) and 3 auxiliary techniques (flushing, manual centration, and bubble bumping) for unfolding the graft in the anterior chamber depending upon the orientation and how tightly the DM is curled. Essentially, the DM scroll in the anterior chamber is opened using short quick bursts of BSS. A portable slit beam or optical coherence tomography attachment on the operating microscope can be used to confirm the graft orientation [50]. After the scroll is partially unwrapped, a small air bubble is injected under the donor to secure the orientation [40]. The recipient corneal surface is stroked to center and unfold the graft completely, followed by air fill in the anterior chamber. The patients are advised to keep supine position for 60 min to allow for donor adherence.
Hybrid Techniques
Hybrid techniques have been developed to combine the optical outcomes of DMEK with the easier handling of DSEK. Studeny described transplantation of a posterior corneal lamella consisting of endothelium and DM centrally with a stromal supporting rim (DMEK-S), and McCauley et al. described a partially automated variation (DMAEK) [21, 22]. The bare central endothelium and DM provide excellent optical outcomes, comparable with those of successful DMEK patients, while the stromal rim provides support to the fragile and thin central portion of the donor. This helps to maintain donor shape and orientation while preventing scrolling, allowing for easier delivery into the anterior chamber while maintaining correct orientation. The donor tissue is dissected as in DSEK using either hand dissection or a microkeratome. The Descemet’s membrane is then detached from the posterior stroma using a big bubble technique (Fig. 4.1, third row). Rapid big bubble formation can cause rupture of DM. More importantly, the bubbles can sometimes develop in the periphery of the cornea, instead of the center. Peripheral bubbles are thinner and tend to rupture and break easily. If a peripheral bubble forms, the donor tissue can no longer be used for the hybrid technique, but an attempt can be made to convert the tissue for use with DMEK. The DMEK-S or DMAEK donor tissue is inserted into the eye using the pull-through technique with the aid of a Busin glide, and air is injected to attach the donor to the recipient stroma. Donor insertion and positioning is easier than DMEK because the tissue unfolds spontaneously because of the added rigidity afforded by the skirt of stromal tissue. Both centers developing the hybrid techniques have discontinued their use because of increased donor loss relative to DMEK and increased need for reinjection of air to promote donor adherence. Nevertheless, hybrid donor tissue can still be ordered from eye banks as precut tissue options.
Ultrathin DSAEK
Some surgeons have reported better visual acuity and faster visual recovery with thinner endothelial grafts [24]. Busin et al. described a microkeratome-assisted double-pass method for obtaining ultrathin posterior lamellar grafts (<100 μ) [23]. The first pass is done with a 300- or 350-μm microkeratome head to debulk the cornea. The thickness of the residual bed determines the selection of the microkeratome head for the second pass, which is necessarily made going the opposite direction to help avoid perforation, because the blade penetrates deepest at the beginning of the pass. Nomograms which take into account donor thickness, corneal storage medium, pressurization of the artificial anterior chamber, and cutting speed have been devised to help select the appropriate microkeratome head size to obtain thin EK donor tissue with either single- or double-pass techniques [24]. Some eye banks reportedly prepare ultrathin DSAEK by varying the pressure inside the artificial anterior chamber to control the depth of cut. The risk of tissue loss from perforation is higher with ultrathin grafts compared with standard DSEK grafts.
Surgical Considerations with Ocular Comorbidities
EK is most straightforward in an eye with a normal anterior segment and a stable posterior chamber IOL. Because of the well-known advantages of DSEK over PK, the indications for EK have expanded to eyes with anterior segment complexity such as those with pupillary abnormalities, peripheral anterior synechiae, glaucoma-filtering procedures, glaucoma tube shunts, prior PK, or anterior chamber IOL. While DSEK can be attempted successfully in all mentioned conditions, the decision for DMEK is more reserved because the DM graft is delicate and requires more manipulation to position the graft in comparison to DSEK. When deciding about the type of EK, the potential advantages of a given procedure need to be weighed against the technical ease in an individual case-based scenario.
Aphakic Eyes with Complete or Partial Aniridia
In eyes with aphakia with complete or partial aniridia, a potential concern is intraoperative or postoperative graft detachment, which may result in graft dislocation into the posterior segment. Several options are available to manage this situation depending upon the extent of iris abnormality [17]. A DSEK pull-through technique with or without a suture is typically used. If forceps are used to pull the tissue in, a fixation suture can be used to secure the donor once air fills the anterior chamber and the donor is in position [33]. A posterior chamber IOL (sulcus/scleral fixated) with or without iris reconstruction/pupilloplasty can be planned simultaneously or a few weeks before an EK procedure. In eyes with large iris defects, the host DM stripping should be avoided or performed cautiously to prevent the fragments from falling into the posterior segment. Furthermore, in aphakic eyes, the air bubble used to promote graft adhesion may migrate to the posterior segment intra- or postoperatively, leading to shallow anterior chambers and iridocorneal touch. Prolonged air tamponade and proper head positioning may be additional measures to promote graft adhesion.
In aniridic eyes with an artificial iris implant, the graft can slide between the edge of the implant and the wall of the eye and fall into the posterior segment. To prevent this from happening, air should be injected under the graft before it is released from the insertion forceps, and a temporary fixation suture should be used to hold the graft in place [17]. Alternatively, the graft can be inserted with a suture pull-through technique, and the pulling sutures can be used to affix the graft until adherence is confirmed in the postoperative period [33].
Phakic Eyes
In eyes with significant cataract, a triple procedure (cataract surgery with DSEK or DMEK) is the preferred approach. This approach is also advantageous with DSEK because cataract extraction deepens the anterior chamber and facilitates unfolding of the graft. In patients with endothelial disease and clear crystalline lenses, one may contemplate endothelial keratoplasty alone [51]. It is prudent to avoid iatrogenic damage to the clear lens and the endothelial graft by avoiding anterior chamber fluctuations. As with PK, following EK the rate of cataractogenesis is accelerated as a result of intraocular manipulations during surgery and the postoperative use of steroids. The probability of cataract progression requiring extraction is significantly associated with the age of the patient [52]. Subsequent phacoemulsification utilizing a soft-shell technique and dual ophthalmic viscoelastic devices (OVDs) in patients who develop visually significant cataracts after DMEK has been found to result in minimal endothelial cell loss and no graft detachment [53].
Prior Glaucoma-Filtering/Tube Surgery
In an eye with prior glaucoma-filtering or aqueous shunt surgery, it may be difficult to achieve an air fill in the anterior chamber as the injected air finds its way into the subconjunctival space through the ostium. Therefore several attempts at achieving air fill may be required. Also, after obtaining adequate air tamponade, the intraocular pressure (IOP) needs to be strictly monitored to avoid extremes of high pressure for prolonged periods, which can be detrimental to the already compromised optic nerve. In the rare cases where the air just escapes easily and the pressure cannot be increased enough to firm the eye, a few drops of viscoelastic can be placed over the end of the tube or ostium of the filter to block the flow. Viscoelastic should not be used until the graft is in place to prevent it from coating the graft interface. Once the patient sits up, the viscoelastic will fall away from superior tubes and ostia, so postoperative IOP spikes should not be an issue.
In the eyes with glaucoma drainage devices, it is important to ensure that mechanical contact between the graft and tube is avoided by properly trimming and repositioning the tube, as required. In eyes with a trabeculectomy, once the patient sits up, the air may fill the trabeculectomy bleb leading to high intraocular pressures. Thus, checking patients a few hours after surgery is important.
Vitrectomized Eyes
Eyes with prior vitrectomy and associated iris/zonular defects may have difficulties in graft adhesion, because air may escape into the vitreous cavity increasing the risk of appositional angle closure/graft detachment. Similar to other situations, prolonged air tamponade may help avoid these problems.
Failed Prior PK
EK under a failed graft can successfully restore the graft clarity and avoid repeat PK. However, in situations where the refractive result of the prior PK was unsatisfactory, it may be better to consider a repeat PK, rather than EK. As mentioned earlier in the DSEK technique section, the DM may be left intact in a failed graft if it does not show any abnormalities [13, 28]. This prevents the weakening of the graft-host junction that may occur inadvertently during the stripping maneuver. In eyes with prior therapeutic PK, the DM may be hazy and require removal for optimal results [54]. If stripping is planned, it should be made internal to the graft-host junction or even in a small area overlying the pupil to avoid disrupting the incision. If a DMEK is planned under a failed PK, then DM needs to be stripped inside the PK graft-host wound because a DMEK graft does not adhere well to intact host DM [55].
The graft can be over-, under-, or same-sized. Oversizing provides the advantage of a larger endothelial cell reserve, while undersizing avoids the need for the EK graft to conform to the irregularity at the graft-host junction that may interfere with the graft attachment process. Particularly with DMEK, an uneven posterior profile of a previous failed PK can make positioning of the donor DM and endothelium more difficult, and reinjection of air to promote graft attachment is required more often than it is in virgin eyes.
One of the most remarkable findings in a series of 60 eyes with DSEK after failed PK was that neither neovascularization nor the number of previous graft failures increased the risk of graft failure. The only preoperative characteristic associated with increased risk of graft failure was previous filtration surgery, either trabeculectomy or aqueous shunt [56].
Iridocorneal Endothelial (ICE) Syndrome
These eyes may have a very shallow anterior chamber because of broad peripheral synechiae [14]. In addition they may have undergone a prior glaucoma-filtering surgery/drainage surgery for IOP control. Extensive synechiolysis may be required for deepening the anterior chamber. Postoperatively, frequent follow-up and aggressive control of IOP are needed for graft survival [57].
Pediatric Endothelial Keratoplasty
DSEK can be more challenging in pediatric eyes as compared with adults. The main reasons for performing EK in pediatric eyes are for failed graft, congenital hereditary endothelial dystrophy (CHED), and pseudophakic corneal edema. Surgical challenges involve insertion and unfolding of the donor tissue in the small anterior chamber of a child, avoiding trauma to the crystalline lens, postoperative positioning requirements, and anesthesia issues [58]. CHED eyes in particular are difficult because of poor visibility. These young eyes have very thin DM, which can be difficult to strip. Pediatric eyes can have a positive vitreous pressure, which can make the surgical maneuvers difficult. Discussing with the anesthetist the need for hypotensive anesthesia during graft insertion and the use of an anterior chamber maintainer during the surgery helps in maintaining the anterior chamber during the DSEK surgery.
Surgical Outcomes
Visual Acuity
When compared with PK, the visual recovery is remarkably rapid, occurring within a few weeks of EK, and mean visual outcomes continue to improve for up to several years afterward, although delayed improvement is more common in DSEK than DMEK. The average Snellen corrected distance visual acuity (CDVA) reported after DSEK has ranged from 20/30 to 20/60 in different studies, with variable follow-up periods [18, 59]. Several factors may interfere with complete visual recovery: graft folds, thickness irregularity, centration, interface haze, and residual anterior abnormalities in the host cornea [60].
DMEK virtually eliminates any thickness variation or folding of tissue to conform to the back surface of the recipient cornea, thereby resulting in better and faster visual recovery with fewer higher order aberrations from the posterior surface of the cornea [61]. Most patients achieve 20/25 or better vision within several weeks with DMEK [39, 40]. Like DMEK, DMAEK also provides superior visual recovery with high rates of 20/25 or better vision [24]. The relationship between DSEK graft thicknesses and visual acuity has been debated [62, 63]. While some believe that thinner grafts are associated with better vision, others have failed to establish this association. Thinner, well-centered, and planar grafts may induce fewer higher order optical aberrations and contribute to superior visual results. Busin et al. have reported excellent visual outcomes with ultrathin DSAEK [23].
Refractive Results
DSEK does not significantly alter anterior corneal topography, but tends to cause a mean hyperopic shift of 0.75–1.5 D through changes in the posterior corneal curvature [64]. Because of the nonplanar configuration of the DSEK donor lenticule, which is typically thinnest in the middle, a minus lens is introduced on the posterior corneal surface. Also, the increase in the thickness of the cornea caused by implanting additional stroma leads to a decrease in the radius of curvature of the posterior surface. The resulting hyperopic shift should be taken into consideration when planning a triple procedure to better achieve the target refraction. Although DMEK does not increase the corneal thickness or introduce a minus lens effect, it also results in a mean hyperopic shift of 0.25–0.50 D that is attributed to the resolution of the corneal edema after restoration of the endothelial function [65, 66].
Endothelial Cell Loss
The endothelial cell loss reported after DSEK is 18–35 % at 6 months, 31–36 % at 1 year, 31–41 % at 2 years, 44 % at 3 years, and 54 % at 5 years [34, 67–72]. Compared with the 5-year cell loss experienced with PK procedures performed in the Cornea Donor Study for similar indications, the cell loss at 5 years may be lower with DSEK [71]. Hence, despite the higher initial endothelial cell loss experienced with DSEK compared with PK, the rate of subsequent cell loss appears to be less with DSEK for reasons that have not been fully elucidated.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


