Endophthalmitis: Categories, Management and Prevention
Ingrid U. Scott MD, MPH
Harry W. Flynn Jr. MD
Dennis P. Han MD
CLASSIFICATION
Infectious endophthalmitis is classified by the events leading to the infection and by the timing of the clinical diagnosis.1,2 The broad categories include postoperative endophthalmitis (acute-onset, chronic or delayed-onset, conjunctival filtering-bleb associated), posttraumatic endophthalmitis, and endogenous endophthalmitis. Miscellaneous categories include cases associated with microbial keratitis,3 intravitreal injections,4 or suture removal.5 These categories are important in predicting the most frequent causative organisms and in guiding therapeutic decisions before microbiologic confirmation of the clinical diagnosis (Table 1).
TABLE 1. Classification of Endophthalmitis (Most Frequent Organisms In Various Clinical Settings) | |
|---|---|
|
INCIDENCE
Postoperative endophthalmitis is the most frequent category, accounting for more than 70% of cases. In a nosocomial survey (1995–2001) of 35,916 intraocular surgical procedures performed at a university-based hospital, acute-onset endophthalmitis occurred in 17 cases (0.05%).6 In this survey, the incidence of acute-onset endophthalmitis (≤6 weeks of surgery) after cataract surgery was 0.04% and did not appear to be increased by a clear corneal approach to cataract surgery. Also in this survey, the rates of endophthalmitis were highest after secondary intraocular lens implantation (1 of 485 cases; 0.2%) and glaucoma surgery (4 of 1,970 cases; 0.2%), and lowest after pars plana vitrectomy (2 of 7,429 cases; 0.03%). There is an increased incidence of endophthalmitis in patients with diabetes mellitus, which is possibly explained by the relative immune compromise in these patients.7 Endophthalmitis may also occur infrequently in the setting of a conjunctival filtering bleb,8,9,10,11 suture removal,5 wound dehiscence, or vitreous wick.12 Chronic or delayed-onset endophthalmitis may be caused by less virulent bacteria (e.g., Propionibacterium acnes, Staphy1ococcus epidermidis) or by fungi.13,14,15,16
In reported large clinical series,17,18,19,20 endophthalmitis after penetrating ocular trauma represents approximately 25% of all cases. In one large study of penetrating ocular trauma, endophthalmitis occurred in 10.7% of cases with a retained intraocular foreign body and 5.2% of cases without a retained intraocular foreign body.20 The National Eye Trauma System Registry reported an endophthalmitis incidence of 6.9% (34 of 492 cases) after penetrating ocular injuries with retained intraocular foreign bodies.21 Metallic intraocular foreign bodies were as likely to be associated with infectious endophthalmitis (7.2%) as nonmetallic (7.3%) and organic matter (6.3%) foreign bodies.21 Rupture of the crystalline lens capsule is also a reported risk for endophthalmitis in open globe injuries.22
Compared to the postoperative and posttrauma categories, endogenous endophthalmitis occurs with less frequency and, when it occurs, usually presents in debilitated or immunocompromised patients or in patients with a history of intravenous drug abuse.23,24,25,26,27 In one large series, culture-proven fungal cases were more frequent than bacterial cases.27
In the miscellaneous category, endophthalmitis after intravitreal injections can be subdivided into infectious and noninfectious categories. In a series of over 828 intravitreal triamcinolone acetonide injections, there were no cases of infectious etiology, but pseudohypopyon from migration of triamcinolone crystals into the anterior chamber occurred in 7 patients in this report.28 Pooled data from 14,866 intravitreal injections in 4382 eyes revealed 38 cases of endophthalmitis.29 Excluding cases reported specifically as pseudoendophthalmitis (e.g., pseudohypopyon), the prevalence of endophthalmitis was 0.2% per injection.29 Noninfectious endophthalmitis cases after intravitreal triamcinolone are noted in several reports (Table 2). 30,31,32,33,34
TABLE 2. Noninfectious Endophthalmitis After Intravitreal Triamcinolone Acetonide Injection for Macular Disease | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
DIAGNOSIS
The diagnostic features of infectious endophthalmitis can be divided into two aspects: clinical recognition and microbiologic confirmation. The clinical signs of endophthalmitis vary depending on the preceding events or surgery, the infecting organism, the associated inflammation, and the duration of the disease. In acute-onset postoperative endophthalmitis, when bacteria are the etiologic agents, the hallmark of the clinical diagnosis is marked intraocular inflammation with hypopyon (Fig. 1).1,2 Other signs of acute-onset postoperative bacterial endophthalmitis include fibrin in the anterior chamber and on the intraocular lens, corneal edema, marked conjunctival congestion, lid edema, and vitritis. Retinal periphlebitis is another clinical sign that is diagnostically helpful in eyes with relatively clear media.35 Endophthalmitis caused by fungal organisms generally has less inflammation, a more indolent course, and less ocular pain. Endogenous candida cases often manifest as isolated white infiltrates in the formed vitreous overlying a focal area of chorioretinitis.24,35
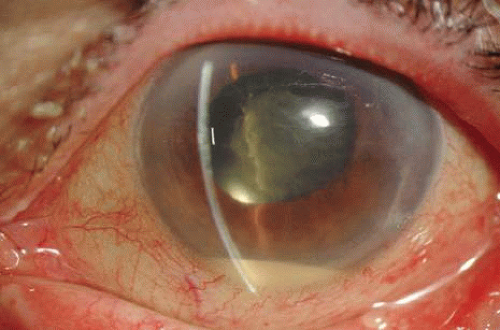 Fig. 1. Acute-onset endophthalmitis following clear corneal cataract surgery. The patient shows conjunctival congestion, prominent fibrin in the pupil, and hypopyon. |
The clinical diagnosis of endophthalmitis is confirmed by obtaining intraocular (aqueous and vitreous) specimens. A vitreous specimen is much more likely to yield a positive culture result than a simultaneously acquired aqueous specimen.36 The vitreous specimen can be obtained either by needle biopsy or by using an automated vitrectomy instrument. A needle biopsy, or limited vitrectomy approach, can be performed in a treatment room, but a three-port pars plana vitrectomy is usually performed in the operating room. One report of 138 culture-proven endophthalmitis cases showed a positive culture result in 34.8% of anterior chamber specimens, 58.2% of vitreous specimens, and 80% of vitrectomy fluid specimens.36
The technique for culturing intraocular specimens depends on the volume of the specimen and the suspected clinical diagnosis.36,37 Direct inoculation of the intraocular fluid specimen onto culture media is a traditional approach and remains a very practical technique. The specific media used for direct inoculation are listed in Table 3. This approach is especially important when limited specimens (such as a needle vitreous or aqueous aspiration) are obtained. These specimens can be inoculated directly onto the appropriate media, including anaerobic media in cases of suspected Propionibacteriurn acnes endophthalmitis. Specimens obtained with automated vitrectomy instruments are diluted by the infusion fluid but can be processed by two methods. One method for processing the vitrectomy specimen uses a membrane filter system in which the vitrectomy specimen is passed through 0.45mm filter paper that concentrates the microorganisms and particulate matter. This filter paper is then sectioned and distributed on the appropriate media.
TABLE 3. Culture Media Used for Endophthalmitis Specimens | |
|---|---|
|
An alternative method involves direct inoculation of the initially aspirated vitrectomy specimen into standard blood culture bottles (Fig. 2).37 This latter technique is particularly useful at night or on the weekend when the microbiology laboratory staff are not available to assist in the processing of the vitrectomy specimen. In a retrospective review of 83 cases, this blood culture bottle method for processing vitrectomy specimens yielded a 91% incidence of positive culture results.37 This rate of positive culture results from clinically diagnosed endophthalmitis cases was similar to simultaneously processed specimens using the membrane filter system.
 Fig. 2. Blood culture bottles may be used for vitrectomy specimens at night or on the weekend when the microbiology staff are not available. Left: The bottle is unopened and has clear media. Right: The inoculated bottle shows growth of organisms as manifested by the opaque media. |
Immunologic as well as molecular genetic technologies enable rapid and specific identification of infectious agents. These real-time techniques have been used in both clinical and experimental settings, and their future use in this area appears promising.38,39,40 Molecular genetic technology has made available specific DNA probes that will interact with the unique DNA sequence for a particular pathogen.40 Clinical application of PCR techniques continues to evolve for the more rapid diagnosis of infectious endophthalmitis.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of marked intraocular cellular inflammation after ocular surgery includes sterile inflammation (related to retained lens fragments or vitreous hemorrhage), iris trauma, pre-existing uveitis, and foreign material introduced during surgery.1,2 Retained cortical lens remnants are reported to cause more inflammation than nuclear remnants.41 These retained lens fragments may occasionally cause a marked inflammatory reaction with hypopyon, which may clinically resemble infectious endophthalmitis.42,43 Blood in the anterior chamber or vitreous cavity may also be confused with endophthalmitis, especially when the blood is long-standing and associated with anterior segment trauma during preceding surgery. Similarly, difficult or prolonged surgery, which often includes vitreous loss or vitreous incarceration in the cataract incision, may increase postoperative inflammation.
Toxic Anterior Segment Syndrome (TASS) is an inflammatory reaction to noninfectious agents that enter the eye during intraocular ophthalmic procedures.44,45,46,47 The typical clinical picture is the presence of diffuse corneal edema (“limbus to limbus”) and marked anterior chamber inflammation detected on the first postoperative day. Symptoms on the first postoperative day include variable pain and impaired vision. Additional hallmarks of the disease include fixed or almost fixed dilated pupil, severe elevation of intraocular pressure, and iris thinning or atrophy. The exact cause of TASS is controversial, but the most frequently implicated cause is the use of improperly cleaned or processed instruments, which allows denatured residual viscoelastic or enzyme detergents to enter the patient’s eye during cataract surgery. Treatment consists of topical anti-inflammatory medications and careful follow-up to rule out the possibility of endophthalmitis. Similar to postoperative endophthalmitis, TASS is a rare problem that can have poor visual acuity outcomes because of persistent corneal edema and chronic intraocular inflammation. It is often difficult to distinguish TASS from endophthalmitis during the early postoperative course. In the Endophthalmitis Vitrectomy Study (EVS), endophthalmitis cases were diagnosed one day after cataract surgery in 5% of patients, within 2 days in 12% of patients, within 3 days in 24% of patients, and within 1 week in 61% of patients.48,49,50,51,52,53,54,55,56,57,58 Further, in the EVS, more virulent organisms (e.g., gram-negative bacteria, Streptococcus species, and Staphylococcus aureus) were more likely to be diagnosed within 2 days of cataract surgery. These cases may also present with marked corneal edema as well as severe intraocular inflammation with varying levels of hypopyon. In the EVS, 31% of patients had a negative intraocular culture. It is possible that some of these cases may have had TASS but were clinically diagnosed as having endophthalmitis. In the EVS, 86% of patients presented with a hypopyon, but TASS may or may not present with a hypopyon early in the course of the disease.
In eyes with mild-to-moderate postoperative inflammation without hypopyon, intensive therapy with topical corticosteroids may be used initially. The careful sequential observation of such eyes will allow appropriate diagnostic and treatment approaches to be employed. Acute-onset postoperative endophthalmitis caused by more virulent organisms, such as Streptococcus species or gram-negative bacteria, will usually present with rapidly progressive clinical signs aiding in the early diagnosis of infectious endophthalmitis. Endophthalmitis caused by the coagulase-negative staphylococci may have fewer inflammatory signs and may have a delayed presentation, often creating difficulty in distinguishing between an infectious and a noninfectious etiology.
TREATMENT MODALITIES
Antibiotics can be delivered to the eye by several local routes, including direct intravitreal injection, periocular injection, and topical administration (Table 4). Endophthalmitis treatment, like the management of infections elsewhere in the body, requires selection of safe and effective antimicrobial agents. The antibiotics selected should cover the broad range of gram-positive and gram-negative bacteria causing clinical endophthalmitis. In the EVS, the use of systemic antibiotics did not improve the outcomes of acute-onset postoperative endophthalmitis in eyes that concurrently received intravitreal antibiotics.48 However, the effect of recently available systemic antibiotics with improved intraocular penetration and broader spectrum, such as fourth-generation fluoroquinolones, could possibly be of benefit in endophthalmitis treatment or prevention.81
TABLE 4. Antibiotics Considered for Local Treatment of Endophthalmitis: Concentration and Dosages of Principal Agents | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
INTRAVITREAL ANTIBIOTICS
Of all the available antimicrobial agents evaluated for intravitreal injection, only a few are used regularly in clinical practice. In the EVS, intravitreal vancomycin 1 mg in combination with amikacin 0.4 mg were used for the initial empiric treatment of acute-onset endophthalmitis.48,49,50,51,52,53,54,55,56,57,58 This combination of intravitreal antibiotics has been reported to be almost always effective for the broad range of bacterial organisms. An alternative to the aminoglycosides for coverage of gram-negative organisms is the use of intravitreal ceftazidime 2.25 mg, a third-generation cephalosporin.61,62,63,64,65,66,67 Outcomes of endophthalmitis treatment are demonstrated in Tables 5 and 6.14,59,60,64,65,66,67,68,69,70,71,88,105 No single antibiotic is effective against the broad spectrum of gram-positive and gram-negative bacteria and fungi.61
TABLE 5. Visual Acuity Outcomes Following Treatment of Endophthalmitis Caused by Various Gram-Positive Organisms* | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
TABLE 6. Visual Acuity Outcomes Following Treatment of Endophthalmitis Caused by Various Gram-Negative Organisms* | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
Repetitive injections of intravitreal antibiotics cause significant retinal toxicity in a rabbit model; eyes treated with a second or third vancomycin/aminoglycoside injection at 48-hour intervals showed progressive toxicity.72 In view of the low rate of persistent infection after initial combination therapy, repeat injection of intravitreal antibiotics are considered only in those cases with progressive inflammation caused by virulent organisms.73 Based on the initial culture report, a single intravitreal antibiotic may be selected for this repeat injection.
VITRECTOMY
The potential advantages of vitrectomy for infectious endophthalmitis include the ability to obtain an adequate vitreous specimen without the theoretically harmful tractional effects of needle aspiration on formed vitreous. Vitrectomy also debulks the vitreous cavity, allowing the removal of the majority of infecting organisms and other inflammatory mediators. Finally, the vitrectomized eye theoretically should allow improved drug circulation throughout the vitreous cavity.
Disadvantages of vitrectomy include the requirement for instrumentation, possibly available only in an operating room setting, which may be associated with a delay in initiating treatment. The view of the posterior segment is frequently obscured by fibrin and inflammatory debris on the surface of the intraocular lens or in the anterior chamber, making vitrectomy surgery difficult and potentially hazardous. The view of the posterior segment can be improved frequently by aspirating or peeling the inflammatory material from the anterior segment or surface of the intraocular lens (IOL).74
Another disadvantage of vitrectomy is its effect on reducing the half-life of injected intravitreal antibiotics.75 Doft and associates studied the ocular clearance of amphotericin B injected into the vitreous in a rabbit model of unmodified phakic eyes, Candida-infected phakic eyes, aphakic eyes, and aphakic vitrectomized eyes. With the use of high-pressure liquid chromatography to assess drug level, the half-lives of drug disappearance after a single amphotericin B 10-mg intravitreal injection were 9.1, 8.6, 4.7, and 4.1 days, respectively. The authors summarized that this rapid disappearance of amphotericin B from vitrectomized eyes must be considered in the clinical management of patients with fungal endophthalmitis.
Vitrectomy for endophthalmitis can be performed using either a two-port (vitreous cutter and infusion needle or irrigating light pipe) or three-port technique (sutured infusion cannula, endoilluminator probe, and vitreous cutter), depending on the surgeon’s preference and the clinical circumstances. A pars plana vitrectomy (PPV) is often recommended for endophthalmitis cases with light perception visual acuity and with moderate (red reflex present and poor view of fundus detail) or severe (no red reflex visible) vitritis. In such cases, preoperative echography is generally performed to rule out retinal detachment and to document the presence or absence of a posterior vitreous detachment. When there is a posterior vitreous detachment, the vitrectomy surgeon can remove more opaque vitreous near the posterior pole and have greater confidence in avoiding contact with the retina. In EVS, the goal of the three-port PPV was to remove at least 50% of the formed vitreous.
A concentrated undiluted vitreous specimen can be obtained at the beginning of the procedure by manual aspiration into a syringe attached to the aspiration line of the vitrectomy handpiece. The intraocular specimens are evaluated using stained smears and direct cultures.
THE ENDOPHTHALMITIS VITRECTOMY STUDY
The EVS was a multicenter, National Eye Institute (NEI) sponsored trial that evaluated PPV and systemic antibiotics in acute postoperative endophthalmitis.48,49,50,51,52,53,54,55,56,57,58 The EVS also evaluated a variety of clinical and microbiologic factors relating to endophthalmitis. The study enrolled 420 patients with symptoms and signs of endophthalmitis occurring within 6 weeks of cataract extraction or secondary intraocular lens implantation. Patients were randomized to treatment with PPV or to vitreous tap/biopsy and to treatment with or without systemic antibiotics. All patients in the study received intravitreal antibiotic therapy (vancomycin 1 mg and amikacin 0.4 mg), and topical and systemic corticosteroids. Patients who appeared clinically worse 36 to 60 hours after presentation underwent reinjection of intravitreal antibiotics. Similarly, patients who were initially randomized to tap/biopsy and had worsening conditions also underwent vitrectomy. The main endpoint of the study was best-corrected visual acuity at 9 to 12 months after presentation. A secondary endpoint was media clarity.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


