Endogenous Fungal Endophthalmitis
Roy D. Brod
Harry W. Flynn Jr.
Darlene Miller
Endogenous or blood-borne fungal infections of the inner eye remain an uncommon but serious cause of ocular inflammatory disease. The incidence may have increased in recent years because of several factors, including the increasing number of immunosuppressed patients receiving antineoplastic, immunomodulating, and other therapeutic regimens; organ transplant patients; as well as the use of newer potent broad-spectrum antibiotics that reduce normal flora.1,2,3 Patients with a history of intravenous substance abuse and low birth weight premature infants also contribute to the increased number of endogenous fungal endophthalmitis cases.4,5,6,7,8,9,10,11,12 The number of AIDS patients developing this complication is declining as a result of improved treatments with highly active antiretroviral therapy (HAART) that reduce the risk of opportunistic infection.13
The endogenous infection may involve only the choroid and retina (as in localized fungal chorioretinitis), may progress into the vitreous or anterior chamber fluids (fungal endophthalmitis), or may involve all ocular tissues (fungal panophthalmitis). Various fungi have been reported to cause endogenous intraocular infection, but by far the most common is Candida species.1 Candida albicans is the most common yeast isolate, and Aspergillus, a mold, is the second most common fungal organism in reported series.1,14 Other fungi reported to cause intraocular infection are shown in Table 11.1.1,2,4,5,6,7,8,9,10,11,12,15 A myriad of ocular inflammatory and neoplastic conditions can resemble endogenous fungal endophthalmitis (Table 11.2). In some cases, differentiation is relatively straightforward; in others, it can be challenging. In most of these conditions a detailed history, careful examination, and appropriate laboratory studies will lead to the correct diagnosis 4,16,17,18,19
Table 11.1 Classification of Fungi Recovered in Endogenous Fungal Endophthalmitis | |||||||
|---|---|---|---|---|---|---|---|
|
Table 11.2 Differential Diagnosis for Endogenous Fungal Endophthalmitis | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
This chapter will review the classification of fungi, predisposing factors, signs and symptoms of the systemic and ocular fungal infections, diagnosis, treatment, and complications. Because Candida species are by far the most common cause of endogenous fungal endophthalmitis, most of the chapter will focus on these organisms.
Classification of Fungi
There exist more than 50,000 species of fungi, but only 100 to 150 of them have been implicated in clinical disease (Table 11.1). This diverse group may be classified or differentiated by morphology (unicellular [yeast/yeastlike] or multicellular [molds]), pigmentation (moniliaceous or dermatiaceous), virulence (pathogenic or opportunistic), or clinical presentation (cutaneous, subcutaneous, or systemic).
Yeasts or yeastlike fungi (e.g., C. albicans) are single-cell organisms, typically round or oval, that form discrete, smooth, creamy and moist colonies (Fig. 11.1) within 24 to 72 hours on routine microbiologic media. They reproduce or multiply by budding. The characteristic appearance is shown in Figures 11.2 and 11.3. Molds (e.g., Aspergillus fumigatus) are multicellular fungi that contain tubular structures (hyphae) and grow by branching and longitudinal extension. These are identified by their macroscopic (Fig. 11.4) appearance (e.g., cottony, woolly, powdery) or microscopic structures (conidia, hyphal segmentation) and color (Fig. 11.5). Some fungi may grow with both yeastlike and hyphal morphology in tissues or culture.
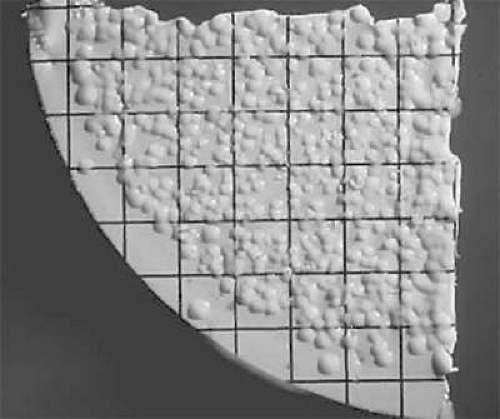 Figure 11.1. Candida albicans on culture plate growing on filter paper from vitrectomy specimen. |
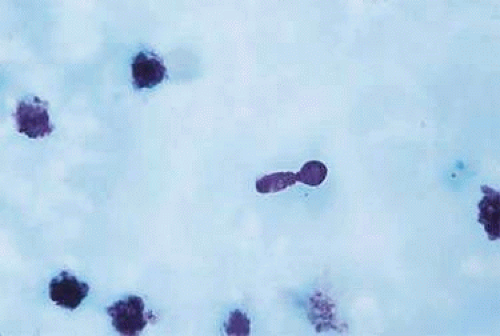 Figure 11.2. Candida albicans on Giemsa stain showing budding. |
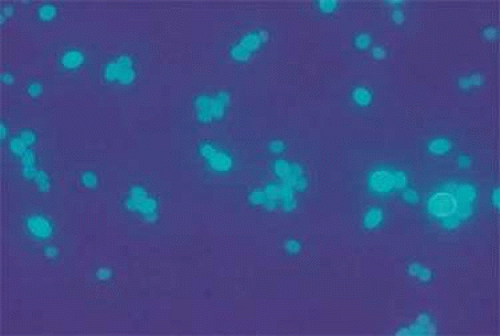 Figure 11.3. Candida albicans on Calcofluor white showing budding. |
 Figure 11.4. Aspergillus fumigatus on culture plate. |
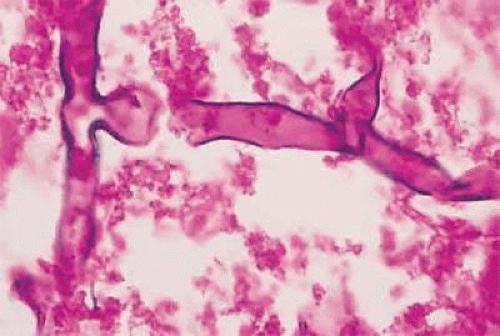 Figure 11.5. Typical broad hyphae of Aspergillus fumigatus on Giemsa stain. |
Antifungal Therapy
The management of fungal infections and endogenous fungal endophthalmitis continues to evolve with the development of newer antifungal agents. 353 The specific management approach for endogenous fungal endophthalmitis remains controversial and depends on the type of fungus, degree of ocular involvement, presence of systemic infection, and the overall health of the patient. There are three major modes of treatment: systemic (oral or intravenous) administration of an antifungal agent (Table 11.3), intravitreal administration of an antifungal agent, and pars plana vitrectomy. All three may be combined in various combinations based on clinical findings and initial response to treatment.
Table 11.3 Systemic Antifungal Agents in Current Clinical Use | |||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Amphotericin B
Amphotericin B has traditionally been the drug of choice for treating most fungal infections although it has limited activity against some non-albicans species of Candida including Candida glabrata and Candida krusei (Table 11.4).20 It still remains an important drug for treating fungal infections, but some of the newer azole compounds (e.g., voriconazole) and the echinocandins are gaining increased acceptance for treatment in many situations.
Table 11.4 Susceptibility Patterns for Common Ocular Fungal Pathogens | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Amphotericin B is one of several polyene antibiotics. It was discovered in 195621 and first used for the treatment of disseminated Candida infection in 1960. It acts by binding to cell membrane sterols, destroying the cell membrane and leading to fungal cell death. Amphotericin B is not absorbed by the gastrointestinal tract and must be given intravenously for systemic effect. It is available as amphotericin B deoxycholate. The addition of deoxycholate increases the aqueous solubility of the drug. The usual daily dose is 0.5 to 1 mg/kg; the average daily dose is 40 to 50 mg. It must be administered over a period of 4 to 6 hours combined with dextrose. For most infections, treatment needs to be continued for at least several weeks.22,23,24
Besides the need for intravenous administration, amphotericin B has other disadvantages. One of the major disadvantages is its significant systemic toxicity.22 Renal dysfunction is the most notable toxic effect and occurs in most patients if the drug is administered for a long enough time. The renal toxicity is usually reversible with cessation of the drug, but permanent renal impairment may result. Another limitation of systemically administered amphotericin B for endogenous fungal endophthalmitis is its poor intraocular penetration.25,26,27,28 For this reason, systemic treatment alone may not be effective for established endogenous fungal endophthalmitis with significant vitreous involvement. Although it is usually very effective for many types of fungal chorioretinitis and systemic fungal infections in general, these serious side effects limit the use of amphotericin B for many patients.29
To address the toxic side effects of amphotericin B, newer lipid formulations of amphotericin B have been developed. The goal of the lipid formulations is to transport the drug throughout the body without exposing the drug to sensitive organs and tissues such as the kidney. These lipid formulations have been successful in accomplishing this goal. The maximum tolerable dose of the lipid formulations can be as high as five times the safe dose of conventional amphotericin B. Lipid formulations of amphotericin B, such as liposomes and emulsion-based carriers, are now commercially available but are significantly more expensive than amphotericin B deoxycholate. Lipid-based nanocarriers for intracellular localization in macrophage-rich organs such as the liver and spleen, as well as a possible oral formulation of amphotericin B, are under development.9,30,31,32,33
Amphotericin B can be administered by direct injection into the vitreous cavity (Table 11.5). Axelrod et al34 first demonstrated the effectiveness of this technique in 1973 in a rabbit model experiment. Doses of 5 to 10 μg were shown to be nontoxic to the rabbit eye.35,36 A single amphotericin B injection of up to 20 μg was shown to be nontoxic in the monkey eye.37 Liposomal amphotericin B was tolerated in doses that were at least fourfold higher than that.36,37 When amphotericin B is injected into the vitreous, it readily reaches the choroid and retinal tissues.38 The drug has a long ocular half-life in nonvitrectomized eyes.39,40 Concentrations from 0.4 to 1 μg/mL were found in the vitreous 5 weeks after injections of 5 to 20 μg.37 Lensectomy and vitrectomy considerably reduce the half-life to 1.8 days.39,40 These half-life data are important when considering reinjection of amphotericin B. In nonvitrectomized eyes, reinjection is probably not necessary for at least a week after the initial injection; however, in eyes that have undergone prior vitrectomy, reinjection can be considered at 3 to 4 days. The safety of intravitreal amphotericin B in human eyes is well established.41,42 A near-normal electroretinogram was recorded 1 year after injection of 20 and 30 μg of intravitreal amphotericin B over 48 and 96 hours, respectively, in a patient with postsurgical Candida parapsilosis endophthalmitis.26 In another case report, separate intravitreal injections of 10 μg amphotericin B over 14 days resulted in a normal electroretinogram 5 months and 5 years after treatment.43
Table 11.5 Intravitreal Antifungal Agents | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The efficacy of intravitreal amphotericin B in treating endogenous Candida endophthalmitis has been demonstrated in multiple reports.44,45,46,47,48,49,50,51,52 Favorable outcomes have been reported when used in combination with vitrectomy as well as when used as the sole treatment. Strains of C. albicans resistant to amphotericin B have been reported to cause endogenous endophthalmitis, but it is more common to find resistance in the non-albicans strains of Candida.53,54,55,56 Fortunately, they are a much less frequent cause of endogenous fungal endophthalmitis. Pseudallescheria boydii and Aspergillus terreus are also frequently resistant to amphotericin B.
Flucytosine
Flucytosine was discovered in 1957 and first used to treat Candida in 1968.57,58,59 Currently, it is rarely used to treat Candida infections because of the high incidence of organism resistance. Resistance occurs in 7% to 47% of Candida isolates, and additional resistance develops commonly during treatment.60,61 Flucytosine has no activity against most of the molds recovered from endogenous endophthalmitis. The advent of newer antifungal drugs has reduced the indications for flucytosine. Its current indication is for the treatment of selected cases of cryptococcal infection. The recommended daily dose is 50 to 150 mg/kg in four divided doses. Peak concentrations occur 2 to 4 hours after a 2-g oral dose. A reduced dose is necessary in patients with impaired kidney function. Side effects are much less common than with amphotericin B (Table 11.3). The combination of flucytosine with amphotericin B may improve its in vivo synergism against C. albicans.56,62,63,64 The use of intravitreal flucytosine in clinical disease has not been reported, but a 100-μg injection has been found to be nontoxic in the rabbit eye65 (Table 11.6).
Table 11.6 Candida species Reported to Cause Endogenous Fungal Endophthalmitis | |
|---|---|
|
Miconazole
Miconazole is one of four azole drugs used as a systemic agent. Similar to the other azole compounds, it acts by inhibiting ergosterol synthesis in fungal cell membranes. It must be given intravenously because of poor gastrointestinal absorption66,67,68,69,70,71,72,73,74 (see Table 11.3). Because of its fairly significant list of side effects and availability of newer and better drugs, systemic miconazole is not currently available for the treatment of fungal endophthalmitis and is included in this chapter for historical purposes only.
Ketoconazole
Ketoconazole was approved by the FDA for systemic use in 1981.75 It acts by inhibiting fungal cell membrane sterols.76 It is well absorbed through the gastrointestinal tract and can be given orally. Gastrointestinal absorption may be variable, however, and depends on gastric acidity. Serum levels peak at about 3 to 6 μg/mL 2 hours after a 200-mg oral dose.77 It is a relatively nontoxic drug (see Table 11.3): Its major adverse effect is hepatic dysfunction, ranging from asymptomatic elevation of liver enzymes to fatal hepatic necrosis. Asymptomatic elevations in liver function studies occur in 5% to 10% of patients; serious hepatic injury occurs in about 1 in 15,000 persons treated with the drug. Because of this, it is important to monitor liver function in patients taking ketoconazole.78,79,80 It is active against various fungi; however, resistant strains have been reported.81,82,83,84
Conflicting data have been reported regarding the intravitreal penetration and efficacy of orally administered ketoconazole for treating endogenous Candida endophthalmitis.85,86,87 In some studies, undetectable vitreous ketoconazole levels were found in healthy rabbit eyes despite adequate serum levels.85 The penetration appears to be better in inflamed eyes, however. A vitreous cavity ketoconazole level of 0.92 μg/mL was detected 8 hours after a 600-mg dose in a patient with postoperative Candida endophthalmitis. This eye had undergone a previous vitrectomy.87 The safety of intravitreal ketoconazole (Table 11.6) has been shown in animal studies, but its use in treating clinical infection in humans has not been reported.88
When first developed, ketoconazole was a significant addition to the available antifungal therapeutic agents, but newer and more effective azole compounds, including fluconazole, itraconazole, voriconazole and posaconazole have now surpassed it.
Fluconazole
Fluconazole is another one of the azole group of antifungal agents.89 It was FDA approved in 1991. Its mode of action is inhibition of ergosterol found in the cell membranes of yeasts and other fungi. It is very selective for fungal cells. It is highly aqueous soluble and has excellent gastrointestinal absorption properties.90 Fluconazole is generally well tolerated, with a low incidence of adverse effects (Table 11.3). Because of its long half-life, once-daily dosing is usually adequate. The recommended dose varies depending on the type and severity of infection and ranges from 100 to 400 mg/day. Because it is weakly protein bound and highly water soluble, it penetrates well into most body tissues, including the eye and cerebrospinal fluid.86,91,92,93 It is excreted primarily by the kidney, and the dose must be adjusted accordingly in patients with impaired creatinine clearance.90,94
Fluconazole is active against a large variety of fungi, including most species of Candida. Candida krusei is well known to be resistant to fluconazole. Candida glabrata may develop resistance during therapy, and reports of acquired resistance to azoles by C. albicans have surfaced. This is usually seen in HIV-infected patients with oropharyngeal or esophageal candidiasis.95,96 Most species of Aspergillus are resistant to fluconazole.
An advantage of fluconazole in treating endogenous endophthalmitis is its excellent intravitreal penetration. Several studies have confirmed this, both in noninflamed and inflamed animal and human eyes.86,92,93,97 Two studies looked at the efficacy of treating experimentally induced Candida endophthalmitis in rabbits.98,99 In both studies, fluconazole was effective in preventing the establishment of ocular infection when administered shortly after inoculation of Candida, but it was not effective when administered 3 to 6 days after inoculation in one study and 7 days after inoculation in the other study. In both studies, the eyes were treated for only a relatively short period, and this may be a major factor in the lack of established efficacy in these studies.
Several clinical case reports have demonstrated the efficacy of oral fluconazole for treating endogenous Candida endophthalmitis.100,101,102,103,104,105,106,107,108 These cases include eyes also treated with vitrectomy but without intravitreal amphotericin B, as well as eyes in which no vitrectomy was performed. In most patients, the dosage required to eliminate the intraocular infection was 400 mg/day. These successfully treated eyes include those with only chorioretinitis and minimal to no vitreitis, as well as a few eyes with significant vitreitis. Postmortem evaluation of eyes from a patient with endogenous Candida endophthalmitis treated for 2 weeks with 200 mg/day fluconazole demonstrated no evidence of organisms in the retina or choroids, but organisms were found in vitreous opacities. This case underscores the need for prolonged treatment with fluconazole when infection involves the vitreous.108 Although these successfully treated patients are encouraging, there are a few reports of progressive intraocular Candida infection despite ongoing oral fluconazole therapy.109,110
Intravitreal fluconazole (5–10 μg) (Table 11.6) has been shown to be safe and effective for treating fungal endophthalmitis in animal and human studies.111,112 Because of the lack of a distinct benefit over intraocular amphotericin B, it is more commonly used as an alternative drug when toxicity is a concern with amphotericin B.
Itraconazole
Itraconazole, like fluconazole, is in the class of triazole compounds. It was FDA approved in 1995. Its mode of action is inhibition of ergosterol found in the cell membranes of yeasts and other fungi similar to that of the other azole antifungal agents. Unlike fluconazole, however, itraconazole is very insoluble in aqueous fluids and is highly protein bound. It does not pass into the cerebrospinal fluid and penetrates into the eye less well than fluconazole. Itraconazole has the edge over fluconazole with respect to direct antifungal activity in vitro. It is well absorbed orally, and its toxicity is relatively low and similar to that of fluconazole113,114 (Table 11.3).
Despite relatively low drug concentrations in the vitreous compared with fluconazole, itraconazole appeared to have similar efficacy in a rabbit model of Candida endophthalmitis.86 In this model it was also similar to fluconazole in its effectiveness in preventing endophthalmitis, but it was less effective in established cases. In general, itraconazole does not appear to have any significant advantage over fluconazole in treating endogenous Candida endophthalmitis, but it is much more effective than fluconazole for Aspergillus endophthalmitis. It is also more effective than amphotericin B for treating infections caused by P. boydii.
Voriconazole
Voriconazole was approved by the FDA in 2002. It is a synthetic second-generation triazole. It is a derivative of fluconazole and inhibits the cytochrome P450-dependent enzyme 14-alpha-sterol demethylase, thus disrupting the cell membrane and stopping fungal growth. It is a more effective inhibitor of 14-sterol demethylase than fluconazole, and this probably explains why fluconazole-resistant pathogens are susceptible to voriconazole. It is available in both intravenous and oral formulations.115,116,117,118,119 A 1% topical solution can also be compounded from the intravenous solution.
An advantage of voriconazole is its extremely good systemic absorption following oral administration. Peak plasma levels of voriconazole are achieved rapidly after a single oral dose. The recommended intravenous and oral doses can be seen in Tables 11.3 and 11.6. Another advantage of voriconazole is its excellent intraocular penetration following systemic administration.120,121 In one study, after two oral doses of 400 mg of voriconazole, the intravitreal and intracameral concentrations were 0.81 ±0.31 μg/mL and 1.13 ±0.57 μg/mL, respectively, representing 38.1% and 53% of plasma concentration. This intraocular concentration is higher than the minimal inhibitory concentration (MIC) 90 of voriconazole for most yeasts and molds.116,120
The intravitreal toxicity of voriconazole was initially evaluated in rats.122 This study demonstrated that an intravitreal dose of 25 mg/mL injected into the vitreous of rats caused no electroretinographic or histologic abnormality in the retina. Extrapolating this data to the human eye, the authors of this study recommended a safe intravitreal dose of voriconazole of 100 μg. This dose has been used to treat cases of fungal endophthalmitis in humans without evidence of toxicity.120,121,123 Intravitreal voriconazole appears to be less toxic to the retina than intravitreal amphotericin B and may prove to be a better choice when intravitreal antifungal therapy is indicated.122 The clearance of intravitreal voriconazole was studied in nonvitrectomized rabbits. The half-life in the rabbit was 2.5 hours. The mean vitreous concentration was 18.912 μg/mL 1 hour after intravitreal injection. This declined to 0.292 μg/mL at 16 hours. The mean aqueous concentration was much lower. The authors concluded that the vitreous concentration achieved during the first 8 hours was greater than the previously reported minimum inhibitory concentrations of organisms most involved in fungal endophthalmitis. There was a relatively rapid decline in the intravitreal concentration after that, and the authors suggested that repeat intravitreal injection of voriconazole may be necessary in humans. This study was done in nonvitrectomized rabbits. Based on the clearance of drugs in eyes that previously have undergone a vitrectomy, it is likely that the clearance would be more rapid and the likelihood of requiring repeat injection greater.124
Voriconazole is fungistatic against Candida species, but is fungicidal against filamentous organisms such as Aspergillus species. It is also effective against noncandidal yeast such as Cryptococcus neoformans.116 It is ineffective against Zygomycetes. Voriconazole is more effective than amphotericin B for the treatment of invasive aspergillosis. The drug is also effective against less common fungal infections, including Fusarium species and Scedosporium. It appears that it is more effective than fluconazole for all species of Candida except Candida tropicalis.
Voriconazole has also been shown to demonstrate good in vitro activity against many dimorphic fungi, including Blastomyces dermatitidis, Coccidioides immitis, Sporothrix schenckii, and Histoplasma capsulatum.116
Systemic voriconazole also appears to be relatively safe when administered orally or intravenously. Adverse reactions include visual disturbances, liver function abnormalities, and skin reactions, including rash and photosensitivity. All these reactions appear to be transient. The visual disturbances occur in about one fifth of voriconazole-treated patients. The visual events usually begin within 30 minutes of the first dose and usually resolve within 30 minutes. Visual disturbances include increased light perception, blurring, photophobia, and color vision changes. The exact mechanism of the visual disturbance is unknown, but based on ERG tests it appears the site of toxicity is the retina. Serious drug-related reactions to voriconazole are rare.116
Posaconazole
Posaconazole is a new triazole antifungal agent that was approved for clinical use by the FDA in September of 2006.115,117,118,126 Posaconazole, like other azole antifungals inhibits the synthesis of ergosterol, the primary sterol in the fungal cell membrane. This depletion of ergosterol reduces fungal cell membrane stability. Posaconazole exhibits fungicidal activity against Aspergillus species, Candida species, as well as Zygomycetes. It has been shown to be affective against certain fluconazole-resistant Candida species, including C. krusei and C. glabrata.126 Posaconazole is available only as an oral suspension at this time.
There are a limited number of studies concerning the treatment of ocular fungal infection with posaconazole. Ocular penetration following systemic administration has not yet been studied. Posaconazole was used to successfully treat cases of ocular Fusarium infections that were refractory to previous antifungal therapy in three patients. All patients received oral posaconazole 800 mg in divided doses and experienced rapid reduction of intraocular inflammation.127 A case of Fusarium solani keratitis and secondary endophthalmitis was successfully treated with systemic posaconazole combined with topical application of posaconazole oral suspension at a dose of 100 mg per mL.128 Posaconazole may have less potential for development of resistant fungi to the drug owing to the fact that it has two different binding motifs for the 14-alpha demethylase enzyme compared to only one binding site for the other triazoles. Posaconazole has a very good safety profile. Gastrointestinal side effects are most common. Headache, menstrual disorder, and increased serum alanine transaminase levels occurred.
Since posaconazole is a newer antifungal agent, its potential use in ocular fungal infection is unknown. Studies to determine the ocular penetration following systemic administration as well as the safety of intravitreal administration are needed. It does appear to have a broad spectrum of antifungal activity and is particularly effective against the Zygomycetes. It also appears to be very effective against coccidioidomycosis and may prove to be useful in cases in which the eye is infected with these organisms. The recommended oral dose ranges from 400 to 800 mg per day in two to three divided doses.
Echinocandins
The echinocandins are a new class of antifungal agents.115,117,118 There are currently three available echinocandins. These are caspofungin, micafungin, and anidulafungin. Caspofungin was the first one to be approved by the FDA in 2001. They work by noncompetitive inhibition of 1,3-beta-glucan synthase in the fungal cell wall. This enzyme’s primary action is the synthesis of glucan polymers of the fungal cell wall. All three are particularly active against Candida, and fungistatic against most Aspergillus species. All three are relatively less effective against most other fungal species They all have a similar spectrum of activity and pharmacokinetics. A beneficial characteristic of this class of drugs is that high levels of drug remain in tissue after plasma concentrations begin to diminish. This characteristic, along with the safety and concentration-dependent pharmacokinetic properties of this class stimulated interest in the possible reduced administration frequency of the drug.129 Currently, once-daily dosing is recommended.
Because of their unique mechanism of action, the echinocandins may be best suited for use in combination with other antifungal agents. Numerous studies have looked at the potential advantage of combination therapy with the echinocandins. In particular, there appears to be synergy when the echinocandins are combined with amphotericin B for both Candida and Aspergillus infection.130 The most recently introduced echinocandin is anidulafungin. Currently, it is available only in parenteral formulation; however an oral formulation is under development. It has the longest half-life of all of the agents in this class and has been shown to be more efficacious than fluconazole for candidemia and invasive candidiasis.115,117
The treatment of endogenous fungal endophthalmitis with this class of drugs has not been studied extensively. There are a few case reports indicating successful treatment of endophthalmitis using caspofungin in combination with voriconazole.131 One study demonstrated the safety and efficacy of intravitreal caspofungin 100 μg/0.1 mL in a rabbit model of Candida endophthalmitis.132 There is one report of Candida glabrata treated successfully with intravenous caspofungin without intravitreal antifungal therapy or vitrectomy.133 Another case report demonstrated a failure of systemic caspofungin to treat Candida albicans endophthalmitis and no detectable caspofungin in a vitreous sample obtained during vitrectomy.134 This case report is compatible with a rabbit study showing poor penetration of caspofungin into the vitreous of inflamed rabbit eyes.135 Based on these studies caspofungin is currently not recommended as single-drug therapy for intraocular fungal infection but may be useful in combination with another antifungal such as voriconazole or amphotericin B. It may also be useful for treating azole-resistant strains of non-albicans Candida. Anaphylaxis, blood dyscrasias and hepatotoxicity have rarely been reported but overall this class of antifungal agents is well tolerated with relatively few serious side effects. Other reported side effects include headache, fever rash, thrombophlebitis, hypokalemia, eosinophilia, and elevated creatinine.
Newer Antifungal Therapies
As mentioned earlier in this chapter, several recently introduced antifungals agents have demonstrated promising results in the treatment of both systemic and ocular fungal infection. Despite these recent advances, the search continues for newer and better drugs to treat fungal infections. Currently studies are underway, looking at the effectiveness of the chitin synthesis inhibitors. The nikkomycins target the chitin synthase and show activity against Histoplasma capsulatum and Blastomyces dermatitidis. Another potential group of antifungal agents are the sordarin derivatives. These agents block fungal protein synthesis and are a promising new class of antifungal agents for the treatment of Candida infection.115,136
Several other molecules with antifungal activity have been isolated from natural sources, including rustimicin, xylarin, and SCH57404. Greater knowledge of antifungal pharmacodynamics is also adding to our ability to treat fungal infections. Knowledge of these pharmacodynamic characteristics may prove helpful in guiding unconventional dosing strategies that could prove to be as effective, safe, and more convenient in critically ill patients with fungal infections. Genectically engineered drugs are also being evaluated for the treatment of fungal infections.136 Finally, increasing knowledge of how various combinations of antifungal agents interact with each other and other drug classes, either antagonistically or synergistically, may be of great value in treating fungal infections.137 Strategies to improve the host immune response are also being investigated for the management of fungal infections.130,138
Endogenous Candida Endophthalmitis
Characteristics of Candida Species
Candida species exists in both a yeast and hyphal phase, depending on the environment. Candida grows rapidly on most common culture media at room temperature. Creamy white colonies begin to appear at 24 to 48 hours after inoculation. C. albicans is a normal inhabitant of the gastrointestinal tract and mucous membranes, including the mouth and vagina.2 Immunosuppression, debilitation, or other predisposing factors may allow Candida organisms to become pathogenic. C. albicans is the most frequent species of Candida causing endogenous Candida endophthalmitis, but several other species of Candida have been isolated (Table 11.6).
Predisposing Factors (Table 11.7)
Table 11.7 Conditions Predisposing to Candidemia and Endogenous Candida Endophthalmitis | |
|---|---|
|
The same factors that predispose a person to develop candidemia predispose to endogenous Candida endophthalmitis, because by definition this represents a blood-borne infection. In the 1980s, intravenous drug abuse was the most common predisposing factor,15 but in the 1990s and first part of 2000, reported cases of endogenous Candida endophthalmitis related to intravenous drug abuse declined.1 The ocular infection usually results from a transient candidemia. Intravenous drug abusers can also develop a distinctive candidiasis syndrome that includes skin and scalp nodules, osteomyelitis, and costochondritis. A published 10-year review (1984–1994) of endogenous fungal endophthalmitis demonstrated that 22% of the cases (4 of 18 patients) had a history of intravenous drug abuse.1,5,6,7,8,9,139,140,141,142,143,144,145
A more common predisposing factor in cases of endogenous Candida endophthalmitis is use of a long-term intravenous line.1,146,147 In these cases, it is likely that the Candida organisms enter the bloodstream directly from contaminated catheter tips. In a 10-year endogenous fungal endophthalmitis study reported by Essman et al,1 67% of the patients has long-term intravenous line placement. Other important predisposing factors are listed in Table 11.7.148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164 Persons with diabetes are also predisposed to develop systemic Candida infection, possibly because of increased glucose available for sustaining the Candida organism as well as the patient’s relative immune compromise and impaired wound healing. Persons with diabetes are also predisposed to develop cutaneous ulcers that may be contaminated with Candida. Corticosteroid use may also predispose to Candida infection by increasing available glucose.165 Diabetes mellitus is found in 15% to 30% of the patient population with candidemia. In one study diabetes was the single most important predisposing factor in true community-acquired candidemia.162 Multiple predisposing factors are often present in patients with systemic Candida infection or endogenous Candida endophthalmitis.166,167,168,169,170,171,172,173,174,175,176,177,178 In rare cases, endogenous Candida endophthalmitis has been reported in otherwise healthy persons with no predisposing factors or events.155,179,180 The ocular infection can occur weeks or months after the predisposing factor has been eliminated, and a careful history looking for preceding risk factors should be elicited in patients suspected of having an intraocular Candida infection.1,164,167,181,182,183,184,185
Relation Between Candidemia and Endogenous Candida Endophthalmitis
Several studies have evaluated the relation between candidemia, candidiasis, and ocular Candida infection (Table 11.8).166,186,187,188,189,190,191,192,193,194,195 This relation is important in determining which patients are at highest risk for the development of intraocular Candida infection and generating guidelines for screening these high-risk patients. The rate of development of intraocular Candida infection in patients with candidemia or candidiasis has been reported to range from 2.8% to 45%.187,188,189,190,192,193,194 Three prospective studies using more rigid clinical criteria for ocular involvement have been reported.187,192,194 The first study examined 118 patients within 72 hours of positive blood cultures for Candida. Only 11 patients (9%) had fungal chorioretinitis, and none had vitreous involvement. All patients in the study were treated with amphotericin B intravenously, and none subsequently developed vitreous involvement.190 In the second study, 214 eyes in 107 patients with a diagnosis of systemic fungal infection were studied. Of the patients examined, 93.4% already were receiving systemic antifungal therapy at the time of ophthalmologic consultation. Only 3 (2.8%) of the 107 patients examined had findings consistent with fungal chorioretinitis. No patient had vitreous involvement, and the ocular findings did not progress during the course of therapy.194 In the third and most recent study, 86 patients with candidemia were examined by an ophthalmologist and 10 patients were found to have intraocular infection.192 In these three papers reported in the 1990s and 2000s, the incidence of Candida endophthalmitis was markedly less than in previously published series in the 1970s and 1980s, in which the incidence of endophthalmitis in patients with candidemia was reported to be in the range of 30% to 40%.166,186,188,190,193 The lower incidence in recently reported studies may be related to earlier diagnosis and more aggressive initial treatment of candidemia and candidiasis by primary and intensive care physicians. Systemic antifungal drugs with better ocular penetration may also have contributed to this. Despite the lower incidence, screening ophthalmologic evaluation of hospitalized patients with documented candidemia or disseminated candidiasis is generally recommended, because early detection and treatment are important in reducing the degree of ocular damage.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


