Fig. 657 The original Kessel endaural incision. The triangle of excision of the skin and conchai cartilage in the first endaural incision performed by Kessel (after H. Heermann 1969)

Fig. 658 The Carlowitz endaural incision with superior and inferior parallel incisions into the concha of the auricle, removal of the conchai cartilage, and creation of a laterally-based skin flap, similar to Körner’s flap in the retroauricular incision (after H. Heermann 1969)
The narrow operating field was a great inconvenience, and Carlowitz (1919) enlarged the meatus by two parallel incisions placed posteriorly in the concha of the auricle (Fig. 658), similar to Körner’s plastic technique (Körner 1894, 1899) used in retroauricular mastoidectomy. The disadvantage of the incision in the auricular cartilage was the potential for perichondritis, and H. Heermann (1939) therefore described an intercartilaginous endaural incision (Vol. 1, Figs. 27–42, Chapters 2 and 3). In fact, Botey (1898) had already described an extracartilaginous endaural incision to enlarge the meatus, but he apparently never used it for an endaural operation.
Lempert was a great advocate of endaural mastoidectomy (Lempert 1929). Initially, he used a triangular skin excision, as suggested by Kessel (Fig. 657). The endaural operation became very popular after the introduction of the one-stage fenestration of the horizontal semicircular canal for otosclerosis. By combining the Heermann extracartilaginous endaural incision with the Surdille tympanomeatal flap (Vol. 2, Fig. 40) for his one-stage fenestration of the horizontal canal, Lempert’s endaural method soon spread throughout the world, popularizing the endaural operation. Shambaugh demonstrated that excision of the meatal skin was not necessary, using a long Surdille flap and extending the intertragal incision in a superior direction (Vol. 1, Figs. 50–54). Lempert described a modification of the Surdille flap, which was attached to the upper edges of the tympanic membrane, by performing a circumferential incision in the posterior and superior meatal wall, and allowing the meatal skin, still attached to the drum, to be elevated in order to expose the tympanic cavity (Vol. 1, Figs. 54–57) and then cover the attic region including the lateral semicircular canal.
Several other surgeons have improved endaural surgery procedures (Guns 1933, Lathorp 1943, Woodruff and Henney 1942, Tumarkin 1947).
Introducing tympanoplasty methods in the 1950s, Zöllner favored the endaural approach, in contrast to Wullstein, who used a retroauricular approach.
Techniques of Endaural Canal Wall–Downm Surgery
As mentioned above, the cavities obtained with an endaural approach are generally small, and the procedure concentrates from the outset around the tympanic cavity, attic, and antrum. The mastoidectomy is performed only as far as is needed to eradicate the disease. The various endaural approaches, i. e., the Heermann II (Fig. 659), Shambaugh (Fig. 660), and Lempert (Fig. 661) incisions, permit exposure of a smaller area of the mastoid plane than the retroauricular approach. The mastoid tip is not accessible in any of these incisions. The Farrior incision (Fig. 662), involving resection of the anterior edge of the conchal cartilage, and the Heermann III incision, extending around the auricle (Fig. 663), enlarge the exposure of the mastoid plane and the access to the sinodural angle and the sigmoid sinus, but the mastoid tip is still not fully exposed. The cortical bone of the mastoid plane is not always removed in an endaural approach, and the pathology is followed in a posterior direction from the external auditory meatus (Fig. 664), usually starting with widening of the ear canal, either from medial (inside-out) or from lateral (outside-in) and then continuing toward the attic and the antrum. The result may be a small atticoantrotomy or a larger canal wall–down mastoidectomy (Fig. 665). The amount of cortical bone removed is still smaller in the most extensive endaural approach than in a retroauricular approach (Fig. 666).
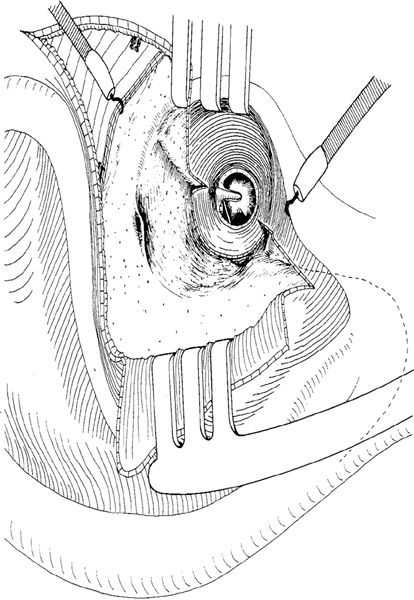
Fig. 659 The Heermann II incision, with elevation of the laterally-based skin flap of the posterior ear canal skin. A large tym-panomeatal flap is created and the entire posterior half of the bony ear canal wall is exposed, as well as part of the mastoid plane. The dashed line indicates the position of the mastoid tip

Fig. 660 The Shambaugh incision, with creation of a large Surdille flap. The ear canal far anteriorly and the mastoid plane are exposed. The dashed line indicates the extent of the mastoid tip
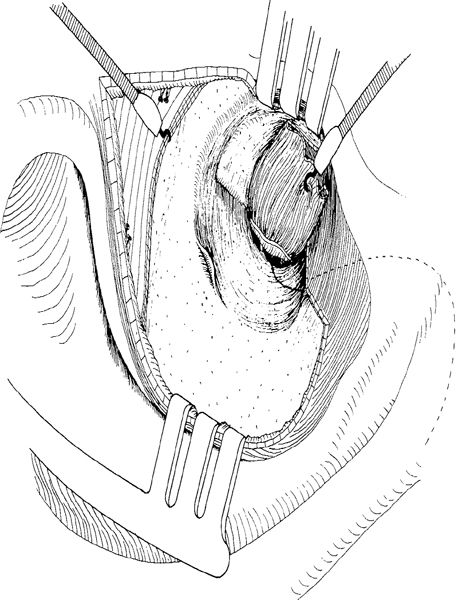
Fig. 661 The Lempert incision. The ear canal skin is elevated together with the drum. The dashed line indicates the extent of the mastoid tip

Fig. 662 The Farrior incision, with excision of a strip of conchal cartilage (arrows) enlarging the access to the mastoid process
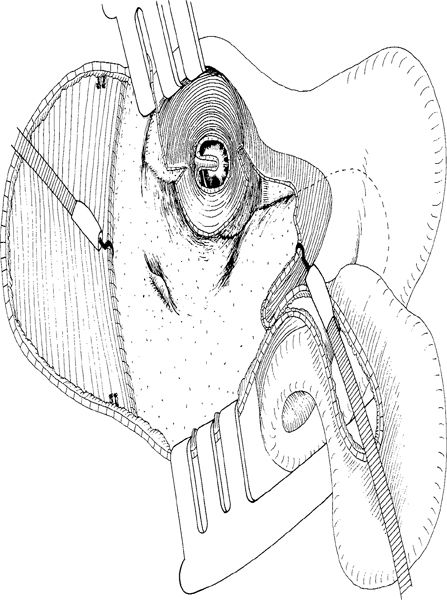
Fig. 663 The Heermann III incision, with the auricle elevated and folded interiorly. A major area of the mastoid plane is exposed, but the mastoid tip is still difficult to access
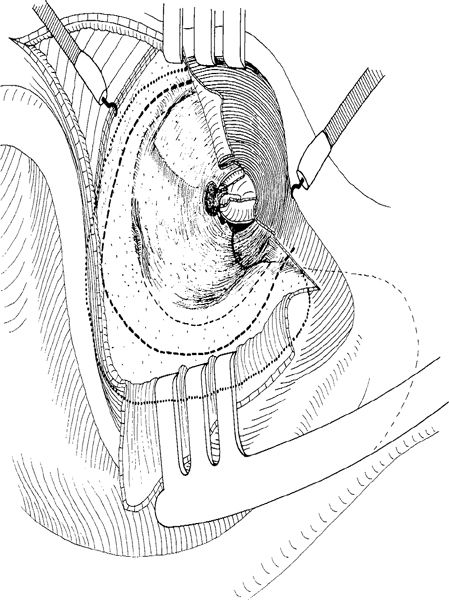
Fig. 664 The extent of removal of the cortical bone of the mastoid plane in an endaural canal wall–down mastoidectomy: no removal of the cortical bone at all (thin dashed line); some removal of the cortical bone, up to about 1 cm posterior to the suprameatal spine (thick dashed line); extensive removal of the cortical bone, requiring further retraction of the auricle (dotted line)
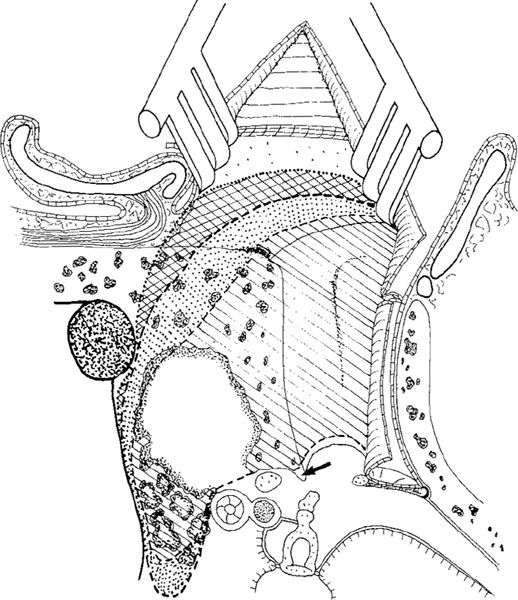
Fig. 665 Resection of the cortical bone of the mastoid plane, seen in a side view. The bone from the ear canal and the edge of the mastoid plane is removed, resulting in a small atticoantrotomy (hatched area). Some resection of the cortical bone of the mastoid plane, allowing access to the posterior fossa dural plate and the sigmoid sinus (dotted area). Extensive removal of the cortical bone and the mastoid plane, providing sufficient exposure of the sigmoid sinus and posterior fossa dural plate (double–hatched area). Arrow: bony annulus
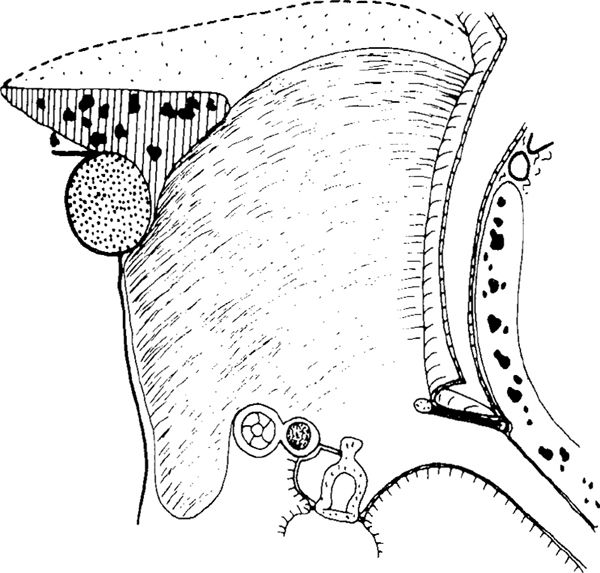
Fig. 666 The dotted area of the cortical bone of the mastoid plane, indicating the difference between bone removal in the retroauricular approach and the endaural approach
Techniques with Removal of the Bridge
When performing endaural canal wall–down mastoidectomy, the present author prefers the inside-out route, starting, after initial widening of the bony ear canal, with a posterior tympanotomy and otosclerosis drilling, providing early information about the condition of the ossicular chain (Fig. 667). If the ossicular chain is defective, further drilling can be rapidly and safely performed. The lateral attic wall is removed posterosuperiorly, providing information about the malleus head and the position of the middle fossa dural plate at the tegmen antri. Further drilling in a posterior direction opens the antrum (Fig. 668) and lowers the facial ridge. The drilling continues along the middle fossa dural plate, polishing it and ensuring that all air cells and bony overhangs are removed. The transition from the anterior bony ear canal wall over the zygomatic root to the mastoid tegmen should be smooth, so that epithelialization of the cavity can take place. Usually there are no problems in removing all pathology from the attic, the tegmen tympani, and the mastoid tegmen, because reasonable exposure of the superior part of the cavity is possible through the endaural approach (Figs. 659–662).
Posterosuperiorly, the drilling is extended to the sinodural angle, which is cleaned. The view to the sigmoid sinus may be difficult in cases with extensive pneumatization (Fig. 669). Drilling toward the mastoid tip may also prove difficult in cases with extensive pneumatization. The facial ridge is usually low, but can be further lowered to the level of the facial nerve if necessary, due to the extension of the cavity toward the mastoid tip.

Fig. 667 Endaural canal wall–down mastoidectomy, starting with enlargement of the bony ear canal, posterior tympanotomy, otosclerosis drilling, and removal of the lateral attic wall, exposing the malleus and the defective incus. The atticotomy is completed, and the drilling continues towards the antrum
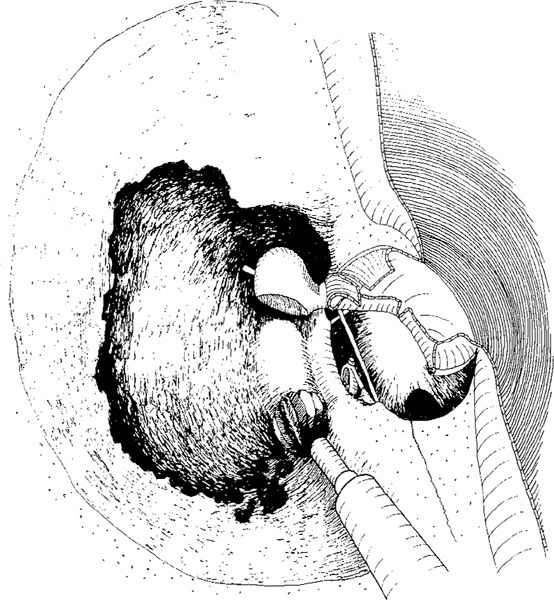
Fig. 668 Endaural canal wall–down mastoidectomy continues in a posterior direction, with opening of the antrum and lowering of the facial ridge. The defective incus is removed. The mastoid air cells are exenterated toward the mastoid tip
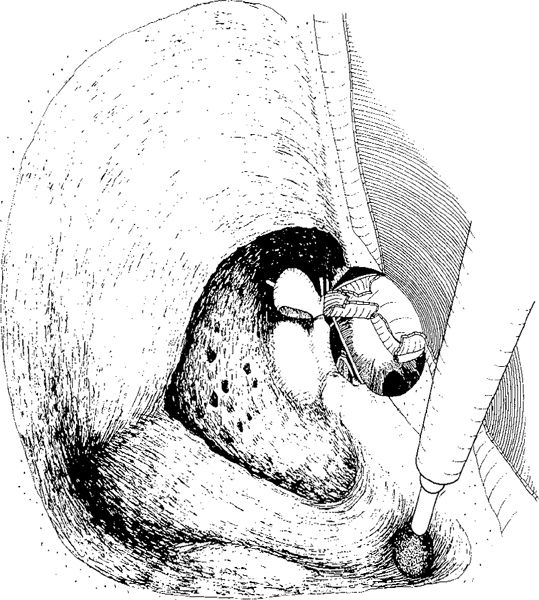
Fig. 669 Endaural canal wall–down mastoidectomy is completed, the cavity is created, the superior wall of the cavity is polished, the sinus wall is cleaned, and the sigmoid sinus is localized. Interiorly the cavity is small and the facial ridge goes straight down towards the facial nerve. If needed the cavity can be further enlarged towards the mastoid tip
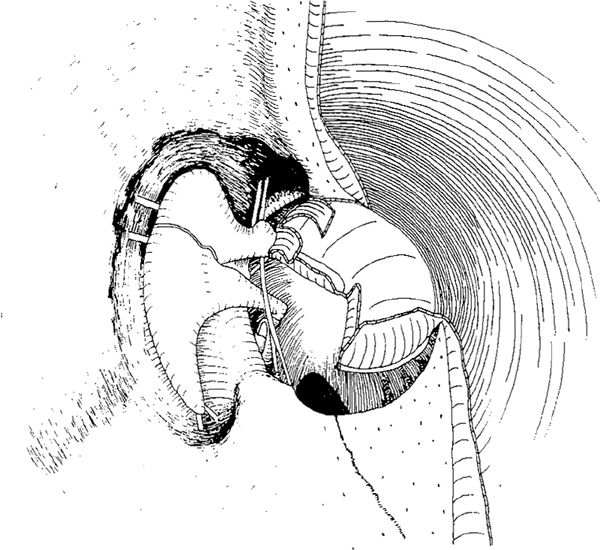
Fig. 670 The situation after a small endaural cavity in a case with an intact ossicular chain and posterior perforation. The facial ridge is low, the cavity walls are smooth, and the attic can be ventilated. There is good access to the anterior tympanum, and the the Eustachian tube orifice and anterior attic are cleaned. There is also a good view of the tympanic sinuses posteriorly

Fig. 671 Reconstruction of an endaural cavity with an intact ossicular chain. The fascia is created as an underlay graft, covering the facial ridge, the ossicular chain, and the mastoid tegmen. Ventilation of the attic can take place, but the antrum region is intended to be an open cavity
Reconstructions in Cases with No Bridge
In ears with no bridge, the resulting cavity is usually an open cavity, at least in the attic region. The chance of achieving a dry cavity after an endaural canal wall–down mastoidectomy without obliteration is good, because the cavity is small and the access created by the endaural approach is large; in addition, all the skin flaps are preserved, i. e., the laterally-based skin flap in the Heermann (Fig. 659) and Farrior incisions (Fig. 662), or the large, medially-based Surdille flap in the Shambaugh (Fig. 660) and Lempert incisions (Fig. 662). These skin flaps can be further shaped either into a large, inferomedially-based flap to cover the facial ridge, or a large, anterosuperiorly-based flap to cover the medial and superior walls of the cavity.
Many variations are possible to cover the lateral parts of the endaural cavity, and these depend upon the incision used. Reconstruction of the medial part of the cavity depends on the remaining ossicular chain and drum remnant.
Intact ossicular chain. In cases with an intact ossicular chain and missing bridge (Fig. 670), repneumatization of the attic is desired. A large fascial graft is placed as an underlay graft under the drum remnant, covering the ossicles and continuing to the tegmen antri. Interiorly, it covers the facial ridge (Fig. 671). After replacement of the skin flaps, epithelialization of the fascia and the cavity is promoted (Fig. 672), and the attic is capable of being pneumatized, resulting in good hearing (Fig. 673). The rest of the cavity remains either open, with fascia or skin flaps covering the bone, or can be obliterated.
Missing incus, stapes present. In cases with a defective incus, but with the malleus head and stapedial arch present (Fig. 674), autogenous incus (Fig. 675) or a piece of cortical bone is usually interposed between the stapes and the malleus handle. The fascia, as underlay graft, covers the ear drum perforation, the interposed incus, the malleus head, and the lateral semicircular canal, as well as the medial wall of the cavity and the facial ridge (Fig. 675). After the flaps have been replaced, rapid epithelization of the medial cavity wall takes place (Fig. 676). Pneumatization of the anterior attic is either maintained (Fig. 677), or the fascia retracts around the malleus head, but even in such cases the malleus may remain mobile (Fig. 678). Retraction around the malleus head in cases with an open attic does not represent a risk of a deep retraction pocket or cholesteatoma formation.

Fig. 672 The canal skin flaps are replaced, and the fascia is fixed at the tegmen tympani, allowing ventilation of the attic

Fig. 673 Side view of the reconstructed endaural cavity, with a ventilated attic at the level of the incus, illustrating the placement of the fascia
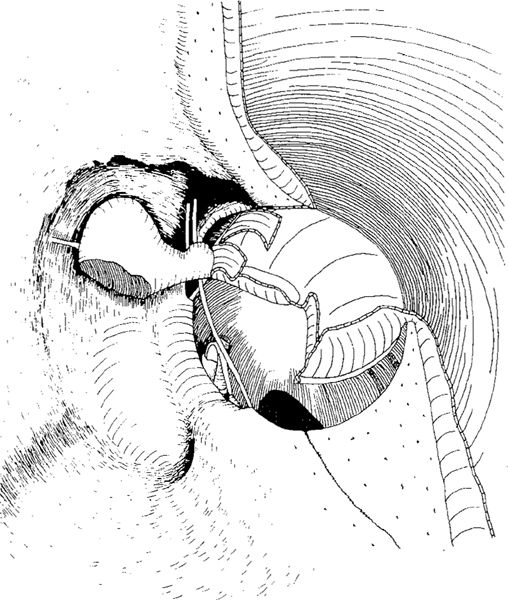
Fig. 674 The cavity after an endaural canal wall–down mastoidectomy, with the incus body removed and a posterior perforation of the pars tensa. The cavity wails are polished, except for the anterior attic, and ventilation can take place here, with an excellent view of the anterior attic and the sinuses
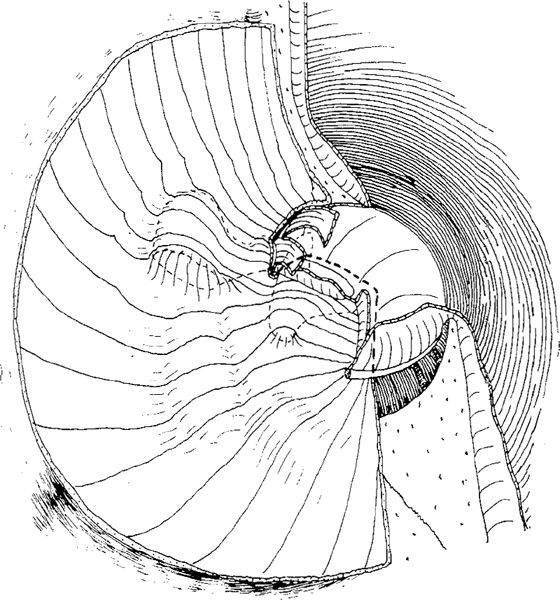
Fig. 675 Reconstruction of the cavity after interposition of the incus between the head of the stapes and the malleus handle, placing the fascia as an underlay graft. The fascia covers the head of the malleus, allowing ventilation of the anterior attic, but in the posterior attic, the fascia goes medially onto the lateral semicircular canal and the facial ridge. The posterior attic is not ventilated
Missing incus and malleus head. This situation with an intact stapes is common in attic cholesteatoma (Fig. 679). The malleus head has been resected because of severe erosion due to cholesteatoma. After interposition with an incus, autogenous cortical bone, or tragal cartilage between the stapes and the malleus (Fig. 680), a large fascial graft covers the ear drum defect, the medial wall of the cavity, the tegmen antri, and the facial ridge (Fig. 681). The cavity is safe, with no risk of retraction, and sometimes the resulting function can be quite good (Fig. 682). In cases with a missing stapedial arch and malleus head, a columella, autogenous incus remnant, or reshaped columella made of cortical bone, are usually used (Fig. 683). The reconstruction with fascia is the same as shown previously (Figs. 680–683), but the functional results are much poorer than in ears with the stapes present.
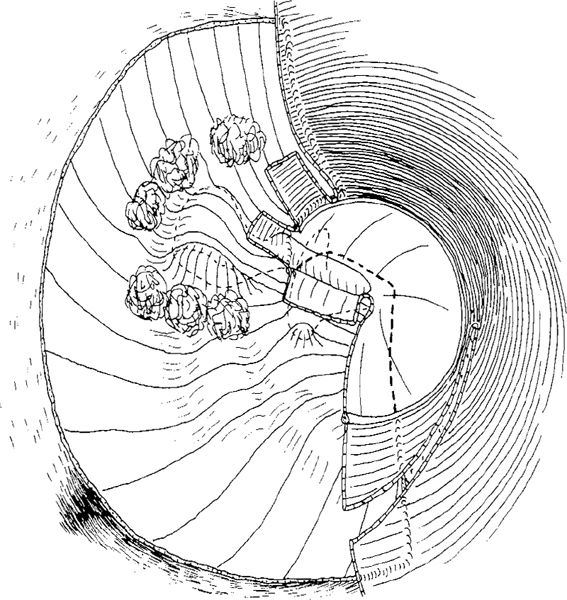
Fig. 676 The skin flaps are replaced, and Gelfoam is fixing the fascial graft
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


