Embryology and Anatomy of the Orbit and Lacrimal System
Embryology and Anatomy of the Orbit and Lacrimal System
Ann P. Murchison
Jurij R. Bilyk
Frederick A. Jakobiec
EMBRYOLOGY
The optic cup and subsequent optic vesicle determine the formation of the surrounding orbit and orbital soft tissue contents. A major discovery of experimental embryologists was the extensive contributions of the cranial neural crest to the connective tissues of the head and neck region, which are due to the local absence of paraxial somites.1,2,3 These connective tissue contributions of the neural crest are collectively referred to as mesectoderm or ectomesenchyme (Fig. 32.1). In the orbit, the fibrous and fibroadipose tissue, the meninges of the optic nerve, the sclera and episclera, the vascular pericytes and striated extraocular muscle satellite cells, the peripheral nerve cellular elements, and the osteocytes and cartilaginous elements are distinctive in being progeny of the neural crest anlage.
Conversely, endothelial cells forming the inner lining of orbital vessels are believed to be an ingrowth into the orbital region of true mesoderm; whether the striated extraocular muscle cells are ingrowths from the preotic somites or whether they represent in situ differentiations of true mesectodermal rather than mesodermal cells is debatable. The latter possibility is more plausible if one remembers that neural tumors are well known to be able to produce heterologous striated muscle differentiations (e.g., in intraocular medulloepitheliomas and in peripheral nerve sheath malignancies [so-called triton tumors]).4,5,6,7,8 Further, certain smooth muscle tumors of the ciliary body and orbit may show unusual neural characteristics in their growth patterns; these have been referred to as mesectodermal tumors.9,10,11 Extremely unusual dysontogenetic tumor masses may occur around the orbit and can combine connective tissue and neural elements (ectomesenchymomas).12
The scaffolding of the orbital bones is laid down within the first 2 months of embryogenesis.13 Migration of the neural crest cells proceeds over the face along two routes, which meet in the area of the orbit.14 The maxillary wave of neural crest cells curves around the developing eye from below, while a frontonasal anlage migrates over the prosencephalon and approaches the optic stalk from above (Fig. 32.2). Thus, the floor and lateral walls of the orbit are contributed by the maxillary process, whereas the lacrimal and ethmoidal bones are contributed by the frontonasal process. The significance of this migratory pattern cannot be overemphasized and is paramount for understanding the location of congenital orbital, eyelid, and lacrimal anomalies (Fig. 32.3). A failure of fusion between the neural crest waves results in clefting syndromes, at least 30 of which involve the orbit.15 Also, the typical location of dermoid cysts at the frontozygomatic and frontoethmoidal suture lines is the result of a sequestration of surface ectoderm in areas of neural crest cell fusion. Finally, it appears that the superficial spread and deep invasion of basal cell carcinoma on the midface may be at least partially due to the location of the embryonic fusion planes.16
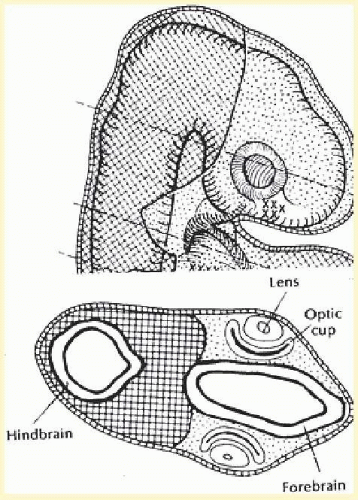
FIG. 32.1 Parasagittal and axial sections through the head of an embryo show the eventual ventral location of the migrated neural crest cells (dotted area) in relation to the paraxial mesoderm (crosshatched area) around the hindbrain. (Johnston MC, Bhakdinaronk A, Reid YC. An expanded role of the neural crest in oral and pharyngeal development. In: Bosma JF, ed. The Fourth Symposium on Oral Sensation and Perception. Bethesda, MD: National Institutes of Health; 1973:37-52. HEW Pub No 73-546.)
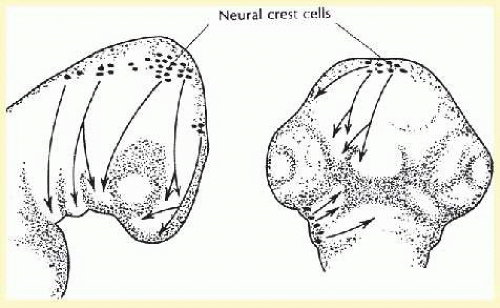
FIG. 32.2 Neural crest cells arise along the dorsolateral part of the neural tube and migrate ventrally to fill in the upper facial process in two waves. (Johnston MC. A radioautographic study of the migration and fate of cranial neural crest cells in the chick embryo. Anat Rec. 1996;156:147.)
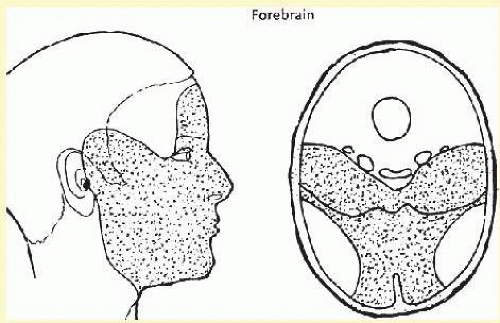
FIG. 32.3 Stippled area of the face indicates the soft tissues and bones of the skull formed by neural crest cells. Note that a portion of the lateral orbital wall and sclera is not included. (Johnston MC, Bhakdinaronk A, Reid YC. An expanded role of the neural crest in oral and pharyngeal development. In: Bosma JF, ed. The Fourth Symposium on Oral Sensation and Perception. Bethesda, MD: National Institutes of Health; 1973:37-52. HEW Pub No 73-546.)
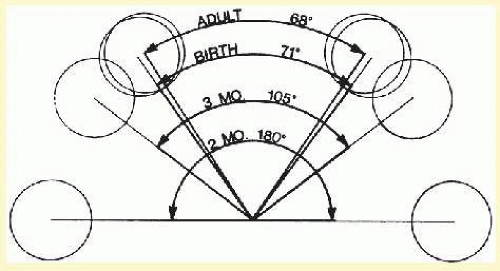
The lesser wing of the sphenoid bone is initially cartilaginous, but the greater wing and the rest of the orbital bones are membranous in nature and ossify and fuse between the 6th and 7th months of gestation. As the orbital bones develop, the eyes converge from an initial 170° to 180° relation to their final position of 68°, achieved in infancy. However, some small amount of remolding continues during childhood, as demonstrated by the orbital axes remaining somewhat divergent at birth (115° between the lateral orbital walls and the skull axis) when compared with that in adults (45°) (Fig. 32.4).15
Most of the orbital bones are formed during the 3rd month, although their ossification ensues over the next several months. At term, the orbit is nearly hemispheric, and the bony perimeters closely hug the globe.17 The ethmoidal sinuses can be observed to begin to take shape between the 6th and 8th weeks of gestation and are fully developed at birth. The remaining paranasal sinuses develop much later, with the sphenoid and frontal sinuses continuing to pneumatize into adolescence or early adulthood (Fig. 32.5). This accounts for the high incidence of orbital cellulitis from adjacent ethmoiditis in children. The lamina papyracea separating the orbit from the ethmoidal air cells is thin and perforate in children, providing easy access for microbial spread. As the remainder of the sinuses are rudimentary in children, they are rarely the source of orbital infectious processes. The lack of paranasal sinus aeration also explains the difference in fracture patterns between very young children and adults. Orbital roof fractures occur more frequently than orbital floor fractures in infants and toddlers due to the lack of frontal and maxillary sinus pneumatization, as well as the relative prominence of the brow in relation to an immature and relatively flat midface.18,19 Aeration of the paranasal sinus also allows for the formation of predictable bony buttresses in the midface and orbit, resulting in the trimalar and Lefort fracture patterns seen in adults; these patterns are distinctly uncommon in young children.
FIG. 32.4 Angular separation of the globes at 2 months’ gestation, 3 months’ gestation, birth, and adulthood. (Fries PD, Katowitz JA. Congenital craniofacial anomalies of ophthalmic importance. Surv Ophthalmol. 1990;35:87.)
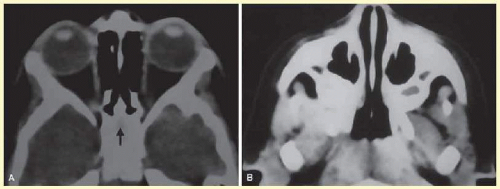
FIG. 32.5 Axial CT of paranasal sinus development in a 2-year-old child. A: Note that the ethmoid air cells are pneumatized, but the future sphenoid sinus is seen only as a faint lucency (arrow) within surrounding bone. B: Rudimentary maxillary sinuses have already partially pneumatized.
The eye reaches adult size by about age 3 years, but the adult dimensions of the orbit (a volume of 30 mL, a lid skin to orbital apex depth of 5 cm, and an overall quadrangular pear shape sweeping toward the medially situated apex) sometimes may not be attained until as late as age 16 years. As the midface develops in puberty, the vertical dimensions of the orbit increase, achieving an adult configuration. The orbit will fail to reach its normal volume if the globe is micro-ophthalmic or if radiotherapy in large doses (as for retinoblastoma or rhabdomyosarcoma) is administered. Conformers of increasingly greater diameter and soft tissue expanders can be inserted into the conjunctival cul-de-sacs of pediatric patients with anophthalmic orbits to promote orbital enlargement.20,21,22
The origin of the extraocular muscles (EOMs, ultimately destined to be four rectus muscles and two oblique muscles) is controversial. The generally accepted theory is that EOMs appear as three separate masses of mesenchyme at about 4 weeks’ gestation. The oculomotor and abducens nerves grow into the muscle masses at about 31 to 33 days’ gestation. The ciliary ganglion is identifiable at about 6 to 7 weeks’ gestation. The EOMs and their connective tissue differentiate simultaneously from superior and inferior mesenchymal complexes.23 At 7 weeks’ gestation, the muscle origins are apparent at the orbital apex. Between the 10- to 25-week stages the perichondrium ring thickens and extends forward into the orbit. The shared apical tendinous origins of the rectus muscles ultimately become the annulus of Zinn surrounding the optic foramen and superior orbital fissure. Anteriorly, the muscles fuse at the end of the 3rd month through tendinous differentiations with the sclera in the vicinity of the equator of the globe. Condensation of periocular tissue, analogous to Tenon fascia bulbi, is identifiable at 10 weeks’ gestation. Myofibrils are identifiable in the anterior portions of the muscle masses during the 6th week of gestation. Sevel has demonstrated that EOM differentiation goes through the phases of indifferent mesenchymal cell, early myoblast cell, fused myoblast cells, myotube cells, and finally mature muscle cells.24 A fibrous trochlea, which later becomes cartilaginous, is initially seen just behind the superonasal orbital rim at the 37- to 40-mm stage of gestation; through it will run the tendon of the superior oblique muscle. The trochlea may rarely become idiopathically inflamed (“trochleitis”) and may spawn rare chondromas.25,26,27
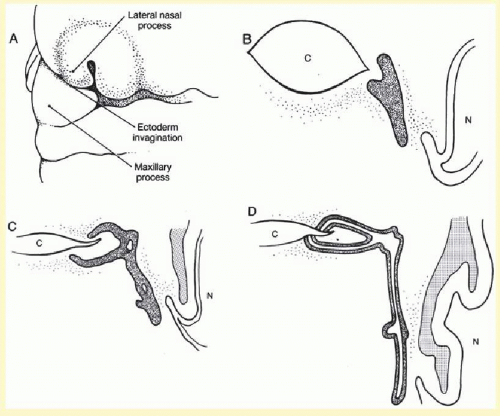
The entire lacrimal drainage apparatus is of ectodermal origin, surrounded by muscles of mesodermal source.13In utero, a solid cord of epithelium becomes buried with growth of the maxillary process in the region of the medial lower eyelid, eventually sending projections temporally to form the canaliculi and inferiorly to form the nasolacrimal duct (Fig. 32.6). Thus, both the puncta and the valve of Hasner are considered “embryologically distal” structures, explaining why most congenital abnormalities of tear drainage are found at these sites (Table 32.1).13 Canalization of the solid cord begins between 8 and 12 weeks of gestation and may continue after birth. Indeed, the most inferior portion of the nasolacrimal duct is imperforate at birth in 60% to 70% of individuals, but frequently opens in the first postnatal month.26,28,29
The main lacrimal gland forms from solid epithelial cords of conjunctiva superolaterally.13,30 The lacrimal gland develops at the 25-mm stage as epithelial buds evaginating from the basal cells of the conjunctiva in the superotemporal portion of the embryonic fornix with condensation of neural crest derived mesenchyme surrounding the epithelial buds. Initially solid cords are formed, but by 3 months’ gestation the central cells begin to vacuolate and lumina appear. The lateral horn of the aponeurosis of the levator palpebrae superioris muscle divides the lacrimal gland into a superficial palpebral and a deeper orbital lobe between the 9th and 11th weeks of gestation.
FIG. 32.6 Lacrimal drainage system embryology. A: At 5.5 weeks’ gestation, an ectodermal invagination forms between the lateral nasal process and maxillary process, which becomes pinched off from the surface. B: At 6 weeks’ gestation, a solid cord of ectoderm is located between the primitive medial canthus and nose. C. At 12 weeks’ gestation, proliferation of the cord occurs laterally toward the eyelid and inferiorly toward the inferior turbinate. The isolated cavities shown appear at 3 to 4 months. D: At 7 months, canalization is nearly complete, with only the puncta and valve of Henle remaining imperforate. (Doxanas MT, Anderson RL. Clinical Orbital Anatomy. Baltimore, MD: Williams & Wilkins; 1984:9.)
Full differentiation of the lacrimal gland is achieved only during the 3rd and 4th years postnatally.13 Note that lacrimal gland tissue is composed of two embryologic anlagen: the ectodermal glandular units are surrounded by mesodermal muscular (myoepithelial) and fibrous tissue. An abnormal growth of both glandular and mesenchymal portions forms a pleomorphic adenoma (benign mixed tumor). Development of the lacrimal gland differs from that of the salivary glands in that the former, as already mentioned, is derived from surface ectoderm, whereas the latter are embryologically related to stomodeal epithelium. This may at least in part account for the different incidence of specific tumor types in the lacrimal gland and the salivary glands, despite their similar histologic appearance.31
TABLE 32-1 Congenital Anomalies of Tear Drainage
Dacryostenosis
Approximately 50% of infants are born without complete canalization of duct, and approximately 4% are symptomatic.
Absence of valves
Pneumatoceles may form in the area of the lacrimal sac and may fill with fluid over time or at birth (amnioceles, blue-domed cysts).
Diverticuli of lacrimal sac
These blind sacs are a result of aberrant epithelial growth and canalization. The term fistula applies if a diverticulum opens onto skin.
Punctal anomalies
Atresia results if epithelization or canalization fails to reach the puncta. Surgical exploration often reveals an intact canalicular system more proximally. Supernumerary puncta are a form of fistula.
Congenital nasolacrimal duct obstruction
By far the most common congenital lacrimal abnormality. Usually due to an imperforate valve of Hasner.
ANATOMY
This section will review the anatomy of the orbit and its surrounding structures: the cavernous sinus (CS), the paranasal sinuses, and the pterygopalatine fossa. Particular attention will be paid to the orbital apex (the superior and inferior orbital fissures, optic canal), the CS, and the pterygopalatine fossa because these areas are often difficult to understand, but remain important in diagnosing orbital and neuro-ophthalmic disease as well as in interpreting radiologic studies (CT and MRI). Although anatomically the lacrimal drainage apparatus is preseptal (eyelid structure) whereas the main secretory unit (lacrimal gland) is partially postseptal (orbital structure), the entire lacrimal system is combined in this section to unify its discussion.
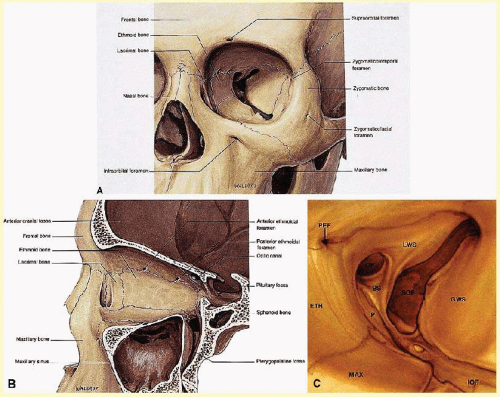
FIG. 32.7 Orbital osteology. A: Oblique frontal view. Note that the supraorbital foramen and infraorbital foramen usually lie in the same vertical plane. The supraorbital foramen may also occur as a notch. Note the discontinuity of the orbital rim medially, forming the lacrimal sac fossa. B: Parasagittal view. The largest diameter of the orbit occurs about 1 cm posterior to the orbital rim. Note the medial location of the optic foramen. The superior orbital fissure and CS lie in the same plane in the orbital apex. Note the vertical orientation of the pterygopalatine fossa located directly behind the maxillary sinus and communicating with the orbit through the inferior orbital fissure. C: Osteology of the orbital apex. GWS, greater wing of sphenoid; LWS, lesser wing of sphenoid; BS, body of sphenoid; P, palatine bone; MAX, maxillary bone; OF, optical foramen; SOF, superior orbital fissure; PEF, posterior ethmoidal foramen. (A and B modified from Dutton JJ. Atlas of Clinical and Surgical Orbital Anatomy. Philadelphia, PA: WB Saunders; 1994:8. C modified from Zide BM, Jelks GW. Surgical Anatomy of the Orbit. New York, NY: Raven Press; 1985:8.)
Osteology
The orbit may be considered a pear-shaped, conical space with a volume of about 30 mL (Fig. 32.7A).13,32 Its maximum diameter occurs approximately 1.0 cm behind the arcus marginalis, an important consideration during surgical dissection around the orbital rim (Fig. 32.7B). The dimensions of the orbit are variable; a guide of average essential measurements is summarized in Table 32.2. The orbit is composed of seven bones: the frontal, sphenoid, ethmoid, palatine, and lacrimal, as well as the zygoma and maxilla, with each wall containing different bones (Table 32.3). One mnemonic for remembering the number of bones contained within each wall is to begin medially and follow the orbital rim inferior to superior, arriving at the sequence 4-3-2-2. Note that the orbital rim is not a continuous ovoid, but rather roughly rectangular, forming a spiral that is discontinuous medially to form the lacrimal sac fossa (see Fig. 32.7A). Other important anatomic pearls regarding each orbital wall are noted in Table 32.4.
A clear understanding of the relation of the bony orbit to the skull and the midface allows for a logical interpretation of the clinical and radiographic patterns of orbital disease. The bones of the face may be considered to hang from the skull, with attachments at the frontozygomatic and frontoethmoidal sutures, as well as the sphenoid bone. Craniofacial dysjunction occurs in these areas in Le Fort III fractures, and the sites of craniofacial articulation are also the basis for the Le Fort III osteotomies used for facial reconstruction in patients with craniofacial synostoses. The complex shape of the sphenoid wing provides for an intimate communication between the CS, the orbital apex, and the pterygopalatine fossa.
Maxilla, lacrimal, ethmoid, sphenoid (anterior to posterior)
Ethmoid, sphenoid sinuses Skull base at level of frontoethmoidal suture
Radiographically, the spaces and foramina of the orbital apex may be considered to lie in three tiers (Fig. 32.8). The CS is found on the same level as the orbital apex, connecting directly with it via the superior orbital fissure (SOF) to form the middle tier. The inferior tier is formed by the inferior orbital fissure (IOF), which provides direct communication between the orbital apex and the pterygopalatine fossa, a vertically oriented space directly behind the maxillary sinus. Finally, the optic canal has no direct communication with any of the aforementioned spaces and should be considered to lie above the SOF and CS, exiting the orbit in a superomedial course through the body of the sphenoid as the superior tier.33 Orbital apical lesions can therefore gain ready access to the CS and pterygopalatine fossa (Fig. 32.9). Spread into the cranial vault through the optic canal is usually limited to lesions of the optic nerve (glioma) or nerve sheath (meningioma).
Paranasal Sinuses
The orbit is surrounded on three sides by the paranasal sinuses (Fig. 32.5). The ethmoid sinus is the only sinus to be fully pneumatized at birth. It runs along the medial orbital wall and is divided into anterior, middle, and posterior air cells by a highly variable system of septa. The most anterior and constant is the agger nasi air cell. The early pneumatization in addition to the thinness of the lamina papyracea and the vascular foramina for the anterior and posterior ethmoidal arteries results in the ethmoid sinus being the most common nidus for orbital cellulitis in children (Fig. 32.10).
The maxillary sinus borders the orbital floor and is fully pneumatized by 2 to 4 years of age. Generally, it contains no supporting septa, though a fibrous or bony septum may be found. Although the lamina papyracea is the thinnest of the orbital walls, the network of septations within the ethmoid air cells acts as a scaffolding to support the medial orbital wall, much the same way that corrugations strengthen cardboard. Thus, the orbital floor, although not the thinnest wall, is the most frequently fractured, because of lack of septations within the maxillary sinus. The posterior wall of the maxillary sinus forms the anterior wall of the pterygopalatine fossa.
TABLE 32-4 Anatomic Findings of Each Orbital Wall
Floor
Slopes downward posterior to anterior 20°
Does not reach orbital apex (ends at pterygopalatine fossa)
Only wall without sphenoid bone contribution
Roof
Contains:
Trochlea, 4 mm behind the orbital rim
Lacrimal gland fossa (postseptal)
Supraorbital notch
Medial
Medial walls parallel, 25 mm apart
“Paper thin” (lamina papyracea)
Lacrimal sac fossa (preseptal)
Lateral
Lateral walls are perpendicular to one another
Strongest wall, but offers least protection to globe (only 50% of globe covered)
Contains lateral orbital tubercle (of Whitnall)
Frontal sinus and accessory air cell pneumatization is highly variable and may continue into the teenage years. Because it drains into the anterior ethmoid air cells through a long and narrow frontoethmoidal recess, the frontal sinus is often concurrently involved in ethmoid sinus pathology and is the most common sinus to form a mucocele. Supraorbital sinuses are defined as lateral extensions of the ethmoid sinus and span the orbital roof for variable lengths. Occasionally, pneumatization to the level of the frontozygomatic suture may occur.
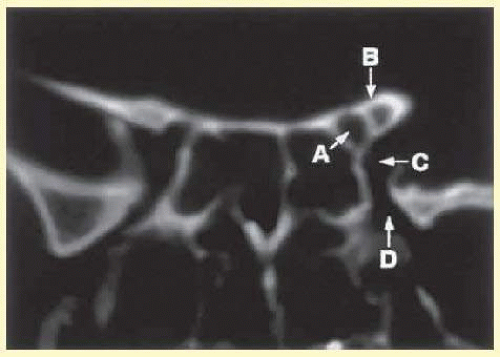
FIG. 32.8 Coronal CT image (bone window) of the orbital apex in a patient with facial trauma. Note the position of the posterior orbital foramina. The optic canal (A) is always seen in conjunction with the laterally adjacent anterior clinoid process (B) on both axial and coronal views. Slightly lower, the superior orbital fissure (C) communicates with the CS, found directly behind it. The inferior orbital fissure (D) provides communication through the orbital floor with the pterygopalatine fossa.
Finally, the sphenoid sinus abuts the orbital apex and is the last to pneumatize. Because of the proximity of the optic canal and CS (see Fig. 32.8) as well as the dehiscence in the bony covering in 24% of cases, any sphenoid sinus pathology may manifest as a parasellar syndrome (discussed later).34 Pneumatization of the sphenoid sinus may extend into the anterior clinoid process, a variation of normal anatomy encountered in 6% to 13% of orbital imaging studies.35,36 The variability in number and location of sinuses is important when planning orbital and/or sinus surgery as the skull base positioning varies between individuals.
Foramina at the Orbital Apex
The orbit is generally found to contain nine openings (Table 32.5). Only the optic foramen, superior orbital fissure (SOF), and inferior orbital fissure (IOF) will be discussed in detail (Fig. 32.8). The optic foramen is located in the medial wall of the orbit in the body and lesser wing of the sphenoid bone. The optic canal is 4 to 10 mm long and 6.5 mm wide. On imaging studies, a 1-mm difference between canal diameters is considered clinically significant. The optic canal transmits the optic nerve, the ophthalmic artery, and the sympathetic innervation to the orbit. Note that sympathetic nerves also travel with the sensory nerves via the SOF.
The optic nerve is tethered on both ends of the canal by the annulus of Zinn intraorbitally and by a dural fold intracranially. The dura of the optic nerve also has strong attachments to the periosteum within the canal.33 Because the canal flares in diameter toward the cranial end, the tightest attachments of dura to the optic canal are at the proximal end (annulus of Zinn). The location of the optic canal and the tethering of the optic nerve within it may explain the etiology of posterior indirect traumatic optic neuropathy. Cadaver studies have shown that stress on the frontal bone is transferred in a reproducible pattern to the body of the sphenoid and the optic canal, potentially resulting in optic canal fracture.37 Further, the tethering of the optic nerve at the annulus of Zinn may cause an acute “stretch injury” at this site during deceleration: as the rigid facial skeleton simply stops on hitting any rigid structure (e.g., the steering wheel in a motor vehicle accident), the soft tissue of the orbit continues to move forward until stopped by the tethered optic nerve. Both of these mechanisms may then result in edema of the optic nerve within the closed space of its bony canal, leading to traumatic optic neuropathy.
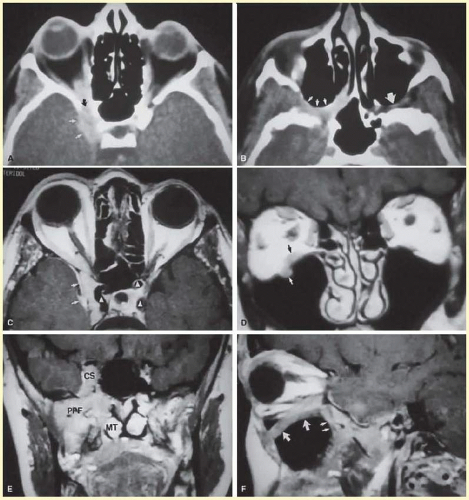
FIG. 32.9 An orbital lymphoma involving the skull base provides accentuation of the apical spaces of the orbit. A: On this axial CT, the lesion infiltrates the CS, causing bulging and local invasion of its lateral dural wall (small arrows). Invasion into the orbital apex through the superior orbital fissure (curved arrow) is seen. Note that the patient is slightly rotated in the scanner, because the anterior clinoid and optic canal are visualized on the uninvolved side. B: More inferiorly, the mass has invaded the pterygopalatine fossa (small arrows), located just posterior to the maxillary sinus. On the uninvolved side (large arrow), the fossa has areas of radiolucency, indicating the fat that normally occupies this space. C: Axial MRI, T1-weighted image with gadolinium but without fat suppression. The carotid siphon is seen within each CS as a flow void (arrowheads). Once again, note the involved lateral dural wall of the CS and local invasion of the brain parenchyma (small arrows). D: Coronal T1-weighted MR image. The inferior rectus muscle is labeled with a black arrow. The lymphoma has infiltrated the infraorbital canal (white arrow) within the orbital floor. E: Coronal MRI of the orbital apex shows infiltration from the CS to the pterygopalatine fossa (PPF). Because there is no direct communication between these spaces, the lesion must have spread through the superior orbital fissure into the orbital apex, then through the inferior orbital fissure. MT, middle turbinate. The lucency just above the CS is the anterior clinoid process, with the optic nerve within its canal seen as an opacity between the clinoid and the sphenoid sinus. F: Parasagittal MRI shows lymphomatous invasion of the pterygopalatine fossa just behind the posterior wall of the maxillary sinus (small arrows). Note the thickening of the infiltrated infraorbital canal (large arrows) as it travels anteriorly to exit about 1 cm below the inferior orbital rim.
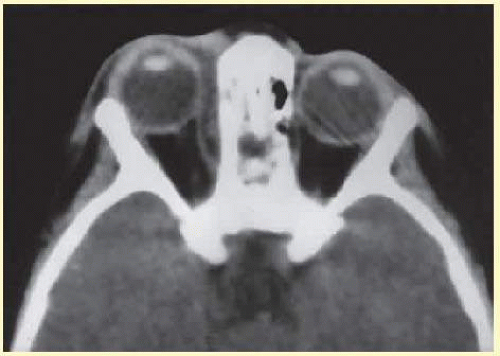
FIG. 32.10 The thin lamina papyracea provides little resistance to infection spread from the adjacent paranasal sinus. In this axial CT image of a 2-year-old child, opacification is noted within the ethmoid air cells. Note the subperiosteal collection along the medial orbital wall. In this case, the collection proved to be a sterile inflammatory phlegmon.
The comma-shaped SOF is 20 to 25 mm long and separates the greater and lesser wings of the sphenoid bone at the junction of the superior and lateral walls.38 Note in Figure 32.8 that it lies lateral and slightly below the optic foramen in radiographic studies. Also note that the SOF, and not the optic foramen, is located at the apex of the orbit (Fig. 32.11). The SOF is split into two compartments by the lateral rectus muscle. The medial compartment contains the oculomotor (superior and inferior divisions), nasociliary, and abducens nerves, the sympathetic and parasympathetic fibers, and superior ophthalmic vein. The lateral compartment transmits the lacrimal, frontal, and trochlear nerves. This extraconal location of the trochlear nerve is appreciated clinically after retrobulbar anesthesia. Although the anesthetic block effectively causes akinesia of the EOMs, the patient often can still intort and depress the globe because of the intact innervation to the superior oblique muscle.
TABLE 32-5 The Nine Canals and Fissures of the Orbit*
Orbital Opening
Features
Supraorbital notch (foramen)
Frontal nerve (supraorbital nerve, V-1)
Anterior ethmoidal foramen
20-24 mm behind orbital rim at frontoethmoidal suture (level of cribriform plate)
Posterior ethmoidal foramen
12 mm posterior to anterior ethmoidal foramen, 5-8 mm anterior to optic foramen
Zygomatic foramina
Zygomaticofacial and zygomaticotemporal neurovascular bundles
Nasolacrimal duct
Beginning at the lacrimal fossa and opening intranasally in the inferior meatus (beneath inferior turbinate)
Infraorbital foramen
Exits 4-10 mm below orbital rim; infraorbital neurovascular bundle (V-2)
Optic foramen
Optic nerve, ophthalmic artery, sympathetic fibers. Diameter ≈ 6.5 mm, length ≈ 10 mm.
Superior orbital fissure
Length: 22 mm
Between greater and lesser wings of sphenoid
Below and lateral to optic foramen
Split into two portions by lateral rectus
Lateral: lacrimal, frontal, trochlear nerves
Medial: CN III (superior and inferior divisions), nasociliary, CN VI, superior ophthalmic vein, sympathetics/parasympathetics
Inferior orbital fissure
Sphenoid, maxillary, and palatine bones; V-2: infraorbital and zygomatic nerves; inferior ophthalmic vein
Frontosphenoid foramina
Frontosphenoidal suture of orbital roof: anastomosis of recurrent middle meningeal and lacrimal arteries (variable)
*The tenth opening, the frontosphenoid foramen, is not present in all cases.
The 30-mm long IOF separates the lateral and inferior orbital walls. It transmits the maxillary nerve (V-2), zygomatic nerves, and inferior ophthalmic vein (as well as the pterygopalatine nerve and the pterygopalatine ganglion nerve) and directly communicates with the pterygopalatine fossa, a vertically oriented space behind the maxillary sinus. The IOF varies in its distance from the orbital rim, but may approach it quite closely (10 mm) before becoming the infraorbital canal. Unlike the supraorbital nerve, which typically exits the orbit at the level of the rim via the supraorbital notch, the infraorbital nerve exits through an ostium in the anterior maxillary wall approximately 1 cm below the inferior orbital rim. The location of the IOF and the slope of the orbital floor are two important points to keep in mind during surgical repair of an orbital floor fracture (see Fig. 32.7B). The tightly adherent periorbita at the IOF may be misinterpreted as entrapped orbital tissue. Aggressive dissection will result in severe bleeding from the infraorbital artery. The 18° to 22° upward slope of the orbital floor from anterior to posterior (see Fig. 32.7B) causes the bone to travel out of view as more posterior dissection is performed with the surgeon at the head of the operating table. If this slope is not recreated during reconstruction, posttraumatic enophthalmos may result because of an enlarged orbital space from a “flat” orbital floor.
Only gold members can continue reading. Log In or Register to continue