Embryology and Anatomy of the Eyelid
Edward H. Bedrossian Jr.
In this chapter, eyelid anatomy is discussed in a layered structural fashion. A brief discussion of the embryology and surface topography is reviewed, and the anatomy of the eyelid is then discussed—beginning with the skin anteriorly and proceeding to the conjunctiva posteriorly. Because the dynamics of eyelid function are associated with the globe and with the surrounding orbital bones, the chapter continues with a discussion of the suspensory ligaments and the eyelid margin. The chapter concludes with a discussion of the vascular supply and the nerve supply to the eyelids. Clinical correlation is provided where applicable.
Embryology
Early Development of the Embryo
A general understanding of the development of the embryo facilitates an understanding of the development of the eyelids. The fertilized ovum is the original cell, which undergoes several divisions to form a solid clump of cells called a morula. The morula then enlarges and forms a central cavity, to become known as a blastula or blastodermic vesicle (Fig. 5.1). The outer wall of the blastula forms the placenta. The blastodermic vesicle embeds itself in the uterine mucosa, enlarges, and forms two cavities—each with a single layer of cuboidal epithelium. The upper cavity is the amnion; the lower is the archenteron or yolk sac. The embryo develops from the embryonic plate at the area of contact between the two. At this stage, the embryonic plate consists of two layers: an outer or dorsal ectoderm (epithelial lining of the amnion) and an inner or ventral entoderm (epithelial lining of the yolk sac). A central depression (the primitive streak) followed by a groove develops on the ectodermal surface of the embryonic plate. A middle layer (intraembryonic mesoderm) appears, thus dividing the embryonic plate into three germinal layers from which all tissues of the body develop. The neural groove closes to form the neural canal (24th day). The surface ectoderm within the neural canal is known as the neuroectoderm.1,2,3
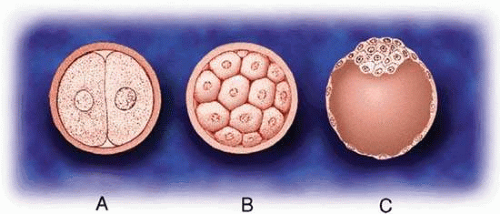 Figure 5.1. Early cell division: (A) fertilized ovum, (B) morula, (C) blastula. |
At the anterior end of the embryonic plate, three head folds form: the forebrain, the midbrain, and the hindbrain. At the front of the forebrain, a small depression is noted on each side of the midline. This depression is the anlage of the eye and is called the optic pit. Toward the end of the third week of gestation, the optic pit deepens until it contacts the surface ectoderm and becomes the primary optic vesicle. At this stage, the eyes are at the side of the head at an angle of 180° (Fig. 5.2). The embryo consists of a head with the three divisions of the brain, a segmented body with spinal canal, and a tail fold. That portion of the mesoderm closest to the spinal canal is known as paraxial mesoderm. The primary optic vesicle then undergoes invagination to form the secondary optic vesicle or the optic cup. This starts at 2.5 weeks’ gestation and is complete by 1 month.3,4,5
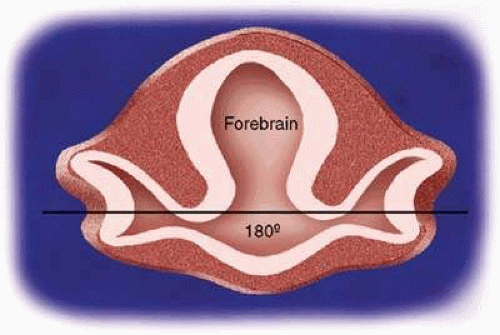 Figure 5.2. Fetal optic axis. At 3 to 4 weeks’ gestation, the primary optic vesicles are at 180°. |
Segmentation
Humans are segmented beings. Segmentation begins simultaneously with closure of the neural groove (24th day). Segmentation extends posteriorly and anteriorly to the head region, where segmentation is lost. Instead, five branchial or pharyngeal arches form. At 5 weeks’ gestation, a sheet of immature mesoderm originates from the first branchial arch (mandibular arch). The first branchial arch consists of a small dorsal portion known as the maxillary process, which extends forward beneath the eye to develop into the lower eyelid. Cephalad to the first branchial arch, mesenchymal proliferation creates other folds that form other facial processes: the frontonasal, medial nasal, lateral nasal, and mandibular processes (Fig. 5.3).1,2,3,4,5,6,7,8
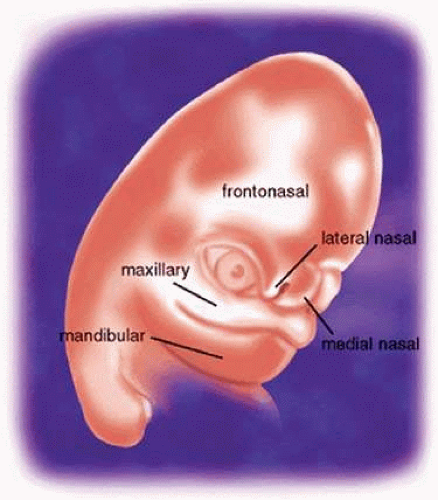 Figure 5.3. The facial processes. |
Eyelid Formation
The maxillary process lies in apposition to the paraxial mesoderm of the eye and the nasal process. Between them is a groove of thickened ectoderm, which becomes buried as the maxillary process overgrows the nasal process. This occurs at 5 weeks’ gestation and is the first indication of the nasolacrimal duct. The maxillary process extends superiorly to form the lower eyelid at 6 weeks’ gestation. In doing so, the inner end folds in a layer of ectodermal tissue that is continuous with the nasolacrimal duct at its lower end. Before the lower lids are apparent, the upper lids are formed by an extension of orbital or paraxial mesoderm known as the frontonasal process. Thus, the upper lid arises from the frontonasal process slightly before the lower lid arises from the maxillary process. The inner end of the upper lid also folds in a portion of ectodermal plate, which forms the upper canaliculus. This unites with the lower canaliculus at the upper end of the nasolacrimal duct.6,7,8
Lid Fusion
At 1.5 months’ gestation, the lateral canthus is formed by the union of the upper and lower eyelid folds. The two lids come together and temporarily fuse from within outward at 8 weeks’ gestation (Fig. 5.4A). Closure is complete at 10 weeks’ gestation. Desmosomal adhesions between the lid margins isolate the eye from the amniotic fluid.1 All lid structures are formed during this period of adhesion (Fig. 5.4B). The Riolan muscle can be identified by the end of the third month. Hair bulbs of eyelashes appear first in the upper lids, then in the lower lids in an anteroposterior direction.2 Development is slightly more advanced in the upper lid, compared with the lower. At the beginning of the fourth month, the meibomian glands begin to appear. The posterior half of the lid shows a greater condensation of basal lamina and collagen fibers, indicating the tarsal plate region. The meibomian glands grow into the tarsal plates—first in the upper then in the lower lids. The apocrine Moll glands also appear around the cilia follicles during the fourth month, followed shortly by the sebaceous glands of Zeis.3,6
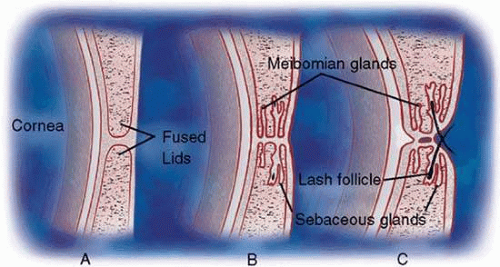 Figure 5.4. Eyelid development. A. Eyelid fusion (8–10 weeks’ gestation). B. Development of margin structures (3–4 months’ gestation); eyelid dysjunction (5–6 months’ gestation). |
At 2.5 months’ gestation, the levator palpebrae superioris develops. It separates from the superior rectus muscle at the fourth month of gestation. Clinically, failure of separation of these muscles would result in congenital ptosis.
Lid Dysjunction
At the end of the fifth month (weeks 21–26 of gestation), the epithelial adhesions between the lids begin to break down (Fig. 5.4C). This process is usually completed by the sixth month but may persist until shortly before birth. Holocrine production of lipids from the meibomian glands, keratinization of the lid margin, and pull of the developing eyelid retractors are responsible for the dysjunction.7,8
Abnormalities of Eyelid Development
When normal progression of lid development is interrupted, a spectrum of congenital anomalies occurs.8,9
Cryptophthalmia (ablepharon)—absence of the eyelid—is caused by failure of the eyelid folds to embryologically develop. The cornea undergoes metaplasia and is covered with skin, which passes continuously from the forehead to the cheek. Most are sporadic, but a recessive inheritance pattern has been suggested.10 Cryptophthalmia occurs bilaterally twice as often as unilaterally and is slightly more common in males. It can be associated with ear and nose malformations, cleft lip and palate, hypertelorism, laryngeal atresia, lacrimal duct defects, renal anomalies, syndactyly, and meningoencephalocele.11
Microblepharia is an incomplete lid development wherein the eyeball is not covered, resulting in congenital lagophthalmos.
Coloboma of the eyelid is a defect in the lid margin, with absence of lashes and glands. The most common site is in the upper lid at the junction of the inner third and the outer two thirds. In the lower eyelid, it is more frequently seen at the junction of the outer third and the inner two thirds. These abnormalities may be owing to the formation and pressure of amniotic bands or from failure of the eyelids to fuse during embryonic life. This may be associated with cleft palate, mandibulofacial dysostosis, limbal dermoids, lipodermoids, iris colobomas, or brow colobomas.9
Epicanthus is a fold of skin that extends from the side of the nose to the upper lid and partially hides the inner canthus. This condition is normally present in the embryo and early infancy. Frequently, it is associated with ptosis, although it may occur independently. Epicanthus is usually bilateral but may be asymmetric or unilateral. There are four known types, depending on the origin of the upper end of the fold. In epicanthus superciliaris, the fold arises in the region of the eyebrow and extends over the lacrimal sac. Epicanthus palpebralis (Fig. 5.5) has an epicanthal fold arising from the upper tarsal area, extending toward the lower margin of the orbit. The fold is equally distributed in the upper and lower lids. In epicanthus tarsalis (Fig. 5.6), the epicanthal fold arises from the tarsal fold and ends close to the inner canthus. Thus, the fold is more prominent in the upper lid. It is a normal variation of the Asian eyelid. In epicanthus inversus (Fig. 5.7), the fold arises in the lower lid and extends upward, partially covering the inner canthus, usually terminating in the upper lid.
 Figure 5.5. Epicanthus palpebralis (also known as simple epicanthus). The amount of tissue above is the same amount as below the canthal angle. |
 Figure 5.6. Epicanthus tarsalis. The epicanthal fold is more prominent in the upper eyelid. |
 Figure 5.7. Blepharophimosis syndrome. The common triad of ptosis, horizontal shortening of the palpebral fissures, and epicanthus inversus (fold more prominent in lower lid) is seen. |
Congenital ptosis is most commonly seen because of the absence or fibrotic nature of the levator palpebrae superioris. It may be unilateral or bilateral and associated with weakness of the superior rectus muscle from which the levator is derived. In the “jaw winking” phenomena, ptosis appears when the patient chews. This is caused by an abnormal association of the nerve to the levator muscle and the nerve to the external pterygoid muscle.
Many abnormalities exist of eyelid margin differentiation. Distichiasis is a condition in which aberrant lashes develop at or near the orifices of the meibomian glands. Ankyloblepharon is an abnormal fusion of the lid margins from incomplete separation of the lid folds. The fusion may be complete but is more common at the inner canthus. A variant is ankyloblepharon filiform adnatum, in which the lid margins are connected by multiple fine bands. Blepharophimosis is a horizontal narrowing of the palpebral aperture. The triad of blepharophimosis syndrome includes ptosis, horizontal shortening of the palpebral fissures, and epicanthus inversus (Fig. 5.7). Telecanthus, lower eyelid entropion or ectropion, hypoplasia of the superior orbital rims, a poorly developed nasal bridge, and hypertelorism can also be seen with this condition.
Epiblepharon is an additional fold of skin running horizontally below the lower eyelid margin. It often is associated with loss of the eyelid crease and may be partly caused by a lack of deep anchoring of the superficial skin to the orbicularis oculi muscle. The weight of the skin fold may rotate the lower lid margin inward, creating an entropion. With growth of the face and nasal bridge, epiblepharon usually diminishes. It is seen more commonly in Asian eyelids.
Euryblepharon is a rounding or almond-shaped deformity of the lower lid at the lateral canthal angle. It may be associated with an inferiorly displaced lateral canthal tendon.
Congenital entropion is characterized by an inward turning of the eyelid margin owing to hypertrophy of the orbicularis muscle, defects in lower lid retractor, or tarsal abnormalities.12
Congenital ectropion is characterized by eversion of the eyelid margin. It is rarely seen in the upper lid. In the lower lid, it is usually seen with Down syndrome or blepharophimosis syndrome.
Surface Topography
Except for prepuce and that of the labia minor, the skin of the eyelids is the thinnest in the body. It is pliable and contains relatively little adipose tissue. It is subject to unusual amounts of stress and relaxation with each blink. Such movement predisposes the paraorbital skin to several natural and dynamic topographic landmarks (Fig. 5.8).13,14,15 The upper lid displays a prominent horizontal crease, the superior palpebral crease. It marks the upper border of the tarsus, is located about 10 mm above the lid margin in Caucasian women and 7 to 8 mm above the lid margin in men. It is accented when the lid is raised. It denotes the dividing line between loosely adherent preseptal skin and that from more adherent pretarsal skin. In the Asian eyelid, the superior palpebral crease is absent or is displaced inferiorly.
 Figure 5.8. Surface topography. |
The lower lid displays three creases. The inferior palpebral crease is less noticeable than the superior palpebral crease and marks the lower border of the lower tarsus. It courses from about 5 mm below the lower lid margin medially to about 7 mm laterally. The nasojugal crease is located below the medial aspect of the inferior palpebral crease and extends infralaterally at 45°. The malar crease originates lateral to and below the lateral canthus. It courses inferomedially until it meets the nasojugal fold 15 mm below the center of the lower eyelid margin.
The palpebral fissure is the opening between the eyelid margins. The vertical palpebral fissure is normally 9 to 10 mm, whereas the horizontal fissure measures 28 to 30 mm. The upper eyelid rests at the upper limbus in the child and about 1 to 2 mm below the upper limbus in the adult. The upper and lower lids rest over the anterior surface of the globe, allowing about 20% of its surface to be exposed in the normal palpebral fissure. The lower eyelid is generally found at the level of the lower limbus. The upper eyelid is slightly curved, with the highest point nasal to the pupil. The lowest point of the lower eyelid is slightly temporal to the pupil. The point where the upper eyelid and the lower eyelid meet medially is known as the medial commissure. The point where the upper and lower eyelid meet laterally is known as the lateral commissure. The medial canthus and the lateral canthus are the angles formed at the medial commissure and at the lateral commissure, respectively. The medial and lateral canthi are dynamic structures that move with horizontal eye movements.16 The lateral canthal angle is normally more acute than the slightly rounded medial canthal angle. The lateral commissure rests on the globe, whereas the medial commissure is anteriorly displaced by the caruncle and plica semilunaris.
The superior orbital sulcus is that area between the upper eyelid crease and the superior orbital rim. With age or after enucleation, a concavity (Fig. 5.9) of the superior sulcus can be seen because of lack of supporting tissue. Convexity (Fig. 5.10) of the superior sulcus is seen with herniation of orbital fat.
 Figure 5.9. Concavity of superior orbital sulcus after enucleation of the right eye. |
 Figure 5.10. Convexity of superior sulcus from herniated orbital fat. |
Langer lines (Fig. 5.11) are present in the upper and lower lids and in the canthal areas. These natural static skin lines are formed by collagenous, reticular, and elastic fibers in the reticular layer of the dermis. Gravitational lines (Fig. 5.12) are formed with age by progressive thinning of relaxed skin. In contrast, dynamic lines (Fig. 5.13) result from repetitious relaxation and contraction of paraorbital muscles. Horizontal forehead furrows show the lateral extent of the frontalis muscle used to correct chronic physiologic ptosis. The action of the procerus and corrugator superciliaris muscles create the “frown lines” between the eyebrows.
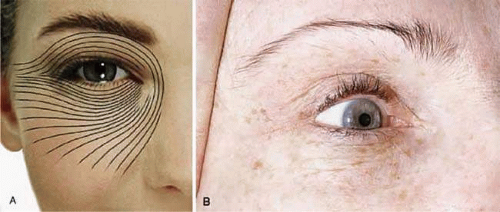 Figure 5.11. Langer lines (A) as they appear in a diagram and (B) clinically. These static skin lines are formed by collagenous, reticular, and elastic fibers in the reticular dermis. |
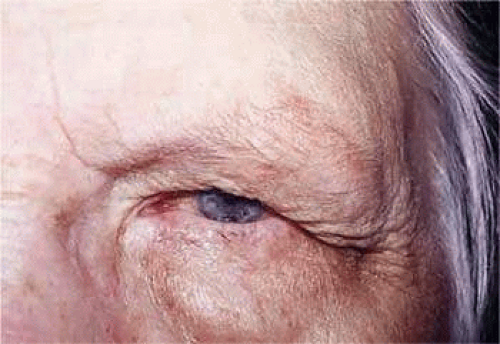 Figure 5.12. Gravitational lines formed by progressive thinning of relaxed skin. |
 Figure 5.13. Dynamic lines. Overaction of the procerus 1 and corrugator superciliaris muscle 2 create these frown lines in this patient with ocular phemigoid. |
The skin of the eyelids is thin. The transition to the thicker skin of the eyebrow above and to the skin of the malar region below is abrupt. In the preorbital and preseptal skin, subcutaneous fat is sparse. Fat is absent in the pretarsal skin. Pretarsal skin is firmly adherent to the underlying tarsus because of attachments of the levator aponeurosis.17 Clinically, edema collects under the loose preorbital and preseptal skin, leaving an identifiable border at the pretarsal skin where there are denser subcutaneous fibroadipose attachments.
Basic Eyelid Anatomy
Protractors
The orbicularis oculi muscle is a thin sheet of concentrically arranged muscle fibers covering the eyelids and periorbital region (Fig. 5.14). It is oval, with the long axis being horizontal, corresponding to the palpebral opening. Contraction of the orbicularis oculi muscle results in the protraction or closure of the eyelid. The orbicularis is firmly attached to the underlying lateral palpebral raphe, the medial canthal region, the insertions of the upper and lower eyelid retractors, the supraorbital ridge, the naso-orbital valley and the malar crease. Jones14,18 divided the orbicularis oculi muscle into three regions: orbital, preseptal, and pretarsal.
 Figure 5.14. Orbicularis oculi muscle, cadaver dissection. (A) Orbital portion; (B) preseptal portion; (C) pretarsal portion. |
The broad orbital orbicularis portion extends superiorly to the eyebrow, where it interdigitates with the frontalis and the corrugator superciliaris muscles (Fig. 5.15). Medially, it extends from the supraorbital notch in a curvilinear fashion over the side of the nose, inferiorly to the infraorbital foramen. It continues along the infraorbital margin. Laterally, it extends to the temporalis muscle. These thick course fibers play an important role in voluntary lid closure (winking) and forced eyelid closure.
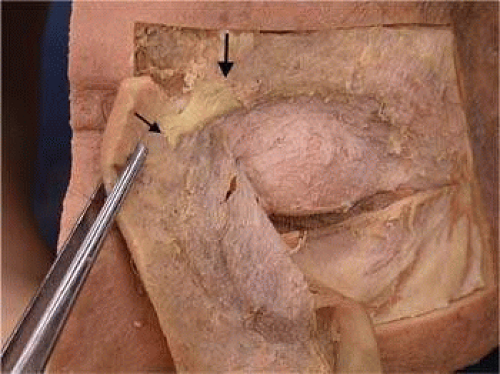 Figure 5.15. Corrugator superciliaris muscle. It originates (thin arrow) on the frontal bone at the supraorbital rim and interdigitates with the frontalis muscle subcutaneously (thick arrow) in the region of the nasal aspect of the eyebrow. |
The preseptal orbicularis overlies the orbital septum. In between is a fibroadipose layer, which is continuous superiorly with the eyebrow fat pad. If this postorbicularis layer contains a significant amount of fat, the ptosis surgeon may misinterpret it as being preaponeurotic fat. Laterally, the preseptal orbicularis muscle inserts directly onto the Whitnall lateral orbital tubercle 3 to 4 mm deep to the lateral palpebral raphe. Because of the fibrous component of this lateral attachment, Jones misleadingly termed this the lateral canthal tendon rather than the lateral canthal ligament.14,18 Medially, the insertions of the preseptal orbicularis are complicated by the lacrimal sac, its fascia, and the lacrimal crests. The medial origin of the preseptal orbicularis is thought to arise from two heads—the deep and the superficial heads. The deep head or Jones muscle18,19 is adherent to the lacrimal sac and lacrimal fascia, whereas the anterior or superficial head arises from the anterior rim of the medial canthal ligament (Fig. 5.16). Functionally, the preseptal fibers contribute to voluntary lid closure (winking) and involuntary lid closure (blinking).
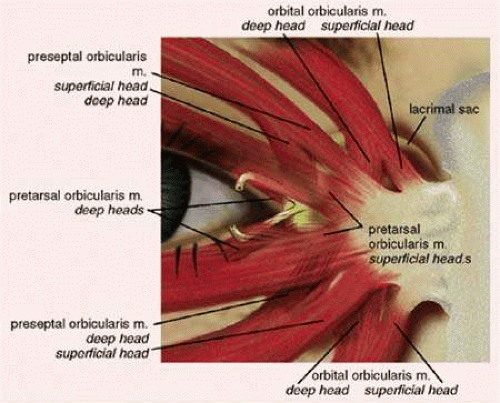 Figure 5.16. Medial attachments of the orbicularis oculi muscle. |
The pretarsal orbicularis is firmly adherent to the underlying tarsus and to the superficial insertion of the levator aponeurosis at the superior tarsal border. The medial origin of the pretarsal orbicularis is thought to arise from two heads—the deep and the superficial heads. The deep head, the Horner tensor tarsi muscle,20,21 arises from 4 mm behind the posterior lacrimal crest and from the lacrimal fascia to insert medially on the tarsi of the upper and lower eyelids. Its contraction pulls the eyelid medially and posteriorly, allowing the eyelids to follow and cover the convex globe. In addition, its lateral contraction on the lacrimal diaphragm creates a negative pressure in the lacrimal sac that draws tears from the canaliculi. The superficial head of the pretarsal orbicularis inserts on the anterior lacrimal crest and anterior limb of the medial canthal ligament. Superficial fibers also surround the canaliculi. Contraction shortens the canaliculi, forcing lacrimal fluid into the lacrimal sac. Functionally, involuntary lid closure (blinking) is primarily the responsibility of the smaller pretarsal orbicularis fibers.
Medially, both Horner and Jones muscles are essential for proper functioning of the lacrimal pump. The deep fibers medially and posteriorly are responsible for proper eyelid-to-globe apposition. Laterally, the orbital and preseptal fibers fuse over the zygoma to form the lateral palpebral raphe. The deep fibers of the pretarsal orbicularis join the inferior and superior crux of the lateral canthal ligament, which inserts 3 to 4 mm posterior to the lateral orbital rim on the Whitnall tubercle.22 It is these latter posteriorly oriented attachments that are responsible for proper eyelid-to-globe apposition and not the more superficial fibers.
Orbital Septum
Upper Eyelid
Historically, the orbital septum has been considered as a discreet, well-defined structure arising from the arcus marginalis. The arcus marginalis is a discrete line seen at the supraorbital rim, representing the condensation of the periosteum of the forehead with the periorbita of the orbit. Alternatively, the orbital septum may be considered the deep fascia of the overlying orbicularis oculi muscle.14 Others23,24 describe a loose fibrous connective tissue anterior to the orbital septum and refer to it as the suborbicularis fascia. The orbital septum (Fig. 5.17) actually is a multilayered structure.25 Fibrous septa within the submuscular fibroadipose tissue become contiguous with more compact lamellae of the orbital septum, imparting a multilayered quality to the orbital septum. Fat within the fibroadipose layer anterior to the orbital septum may be mistaken for the preaponeurotic fat pad during eyelid surgery.26
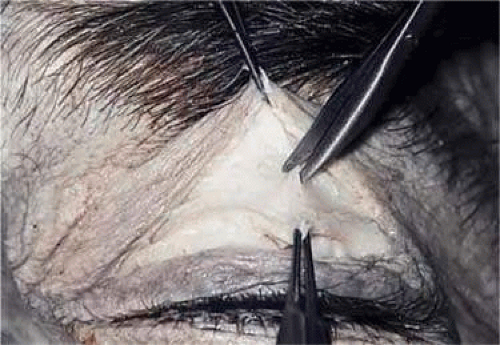 Figure 5.17. With the skin and orbicularis oculi muscle incised and retracted, the multilayered orbital septum is being cut in this cadaver. |
The orbital septum and the levator aponeurosis (Fig. 5.18) join 2 to 5 mm above the superior tarsal border. The orbital septum directly adjoins the posterior epimysium of the orbicularis for about 1 to 5 mm before joining the levator aponeurosis. The cross-sectional thickness of the orbital septum through its parallel lamella varies but is less than 1 mm. It is thickest at the arcus marginalis laterally and is thinnest in the lower lid medially. Medially, posterior orbital septal lamella are carried posteriorly by the pretarsal orbicularis muscle, which inserts on the posterior lacrimal crest. Superficial orbital septal fibers, as described by Whitnall,14 appear to cross and adhere to the lacrimal fascia before reaching the anterior lacrimal crest. At the lateral canthus, the orbital septum is also split; deep fibers insert at the Whitnall tubercle, whereas superficial fibers join at the lateral canthal raphe, just deep to the orbicularis muscle.25
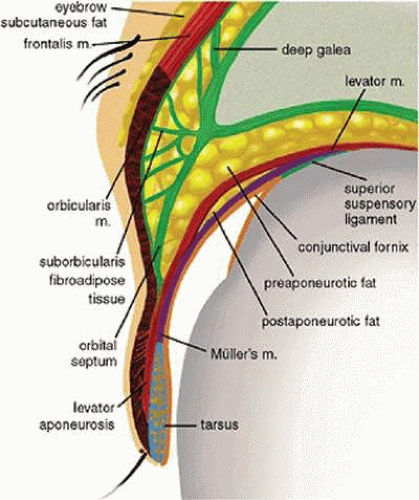 Figure 5.18. Cross section of the upper eyelid.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|