Electroretinography
Ronald E. Carr
The standard clinical electroretinogram (ERG) is a recording of the electrical discharges from certain outer retinal layers elicited by a flash of light. The response occurs as a result of transient movements of ions in the extracellular space induced by the light stimulus.1
Clinical Electroretinography
In the clinical setting, only the early electrical responses of the retina (within the initial 200 msec) are measured, because later responses usually are obliterated by eye blinks. Within this 200 msec time frame, two predominant responses occur: the a-wave and the b-wave (Fig. 103.1).
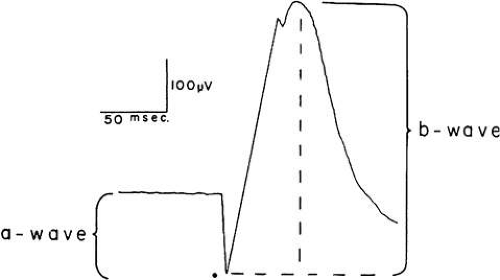 Figure 103.1. Schematic of a dark-adapted ERG in response to a high-intensity light flash (·). The a-wave amplitude is measured from the baseline to the lowest negative excursion of the trace. The b-wave amplitude is measured from the lowest point to the highest positive peak. (Reproduced with permission from Carr RE, Siegel IM. Visual electrodiagnostic testing. Baltimore: Williams & Wilkins, 1982.) |
The a-wave is the initial downgoing deflection, and it arises from the photoreceptor cells.2 The b-wave is the upgoing deflection that follows the a-wave, and it arises from the Müller cells.3 Although the derivation of the b-wave is from the Müller cells, it reflects such activity from the region of the bipolar cells.4
Under certain recording conditions, small wavelets, called oscillations, may be seen riding on the downgoing and upgoing waves (Fig. 103.2). These oscillatory potentials arise from a number of cell types in the midretinal layers.4
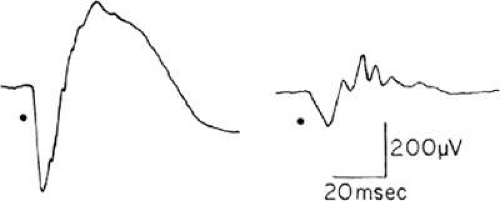 Figure 103.2. Left: Dark-adapted ERG demonstrating the oscillatory potentials riding the ascending limb of the b-wave. Right: By selective filtering, the slower components of the ERG, including the b-wave, can be eliminated, leaving only the fast-frequency components, the a-wave, and the oscillatory potentials. (Reproduced with permission from Carr RE, Siegel IM: Visual electrodiagnostic testing. Baltimore: Williams & Wilkins, 1982.) |
From the foregoing discussion, it is clear that the ganglion cells play no role in the generation of the ERG. Therefore, diseases affecting only the inner retina or the optic nerve should not alter the ERG. It is also important to realize that the standard clinical ERG is a mass response, reflecting activity from the entire retina. Thus, small localized lesions (e.g., macular degeneration) will not affect the ERG amplitude.
Methods of Examination
The electrical discharges elicited by the light stimulus are recorded directly from the eye via a contact lens placed on the cornea. The signal then is amplified and visualized on an oscilloscope or directly written out on any x-y plotter. To enhance the signal, the light usually is delivered via a Ganzfeld (full-field) bowl, a hemisphere used to scatter light throughout the entire retina. This method also avoids some of the problems associated with light scatter.
Parameters
Two major parameters are used to evaluate the ERG response in the clinical setting. The first is the amplitude of the wave, which is measured in microvolts (μV). The amplitude of the a-wave is measured from the baseline to the trough of the a-wave, whereas the b-wave is measured from the trough of the a-wave to the peak of the b-wave (see Fig. 103.1).
The implicit time is the second major parameter. It is defined as the time from the stimulus onset to the peak of the response and is measured in milliseconds. The easiest and most accurate measure of the implicit time is the b-wave under light-adapted or photopic conditions (Fig. 103.3).
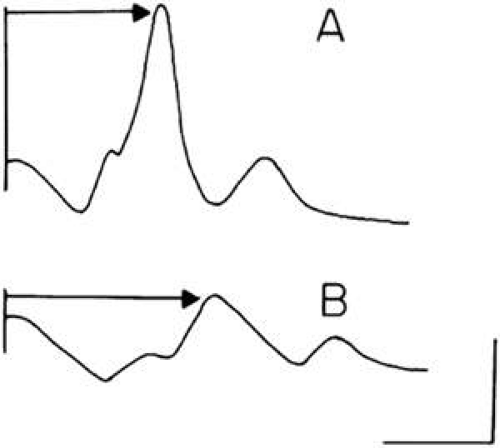 Figure 103.3. Implicit time of the ERG photopic b-wave. The implicit time is measured from the stimulus to the peak of the response. A:. Normal. B: Patient with retinitis pigmentosa showing a reduced amplitude b-wave with an increased implicit time. |
Stimulus Conditions
Certain stimulus conditions allow the isolation of either the cone or rod responses so that each receptor can be studied independently. Under photopic or light-adapted conditions with a bright background light, the rods are sufficiently dampened so that the only response is from the cones. The cone response is rapid, with a b-wave implicit time usually between 28 and 32 msec. The cone response also can be isolated by using a rapidly flickering light. The cones follow a flickering light of up to 60 to 70 Hz, whereas the rods follow a flickering light only up to 12 to 16 Hz. Therefore, a stimulus flickered at 30 Hz elicits a response only from the cone receptors (Fig. 103.4).
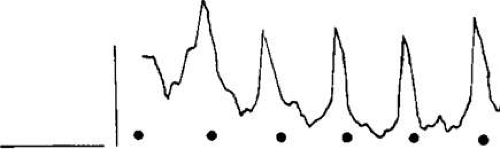 Figure 103.4. Flicker ERG. A repetitive high-intensity flash (30/sec) produces this all-cone response. Calibration: 50 msec, 200 μV. |
After sufficient dark adaptation (30 min), the rod responses are optimized under these scotopic conditions. A single bright flash gives a response that is a composite of the dark-adapted rods and the dark-adapted cones. This response is much larger and has a longer implicit time than is the pure cone response. How, then, does one look at the rods alone? Because the rods are very sensitive to light at the blue end of the spectrum, a weak blue-light stimulus produces an essentially pure rod response (Fig. 103.5).
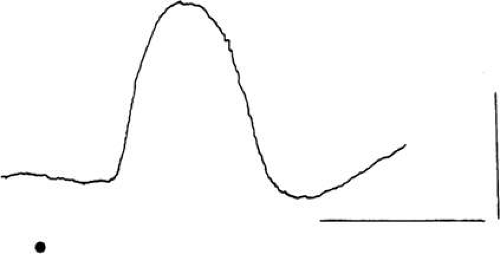 Figure 103.5. ERG response of the dark-adapted eye to a dim blue flash. Calibration: 80 msec, 200 μV. |
Finally, a red stimulus under scotopic conditions results in a biphasic response in which the initial wave represents the more rapidly responding cones and the second response the slower responding rods (Fig. 103.6). This biphasic response occurs because the rods are relatively insensitive to light at this longer wavelength.
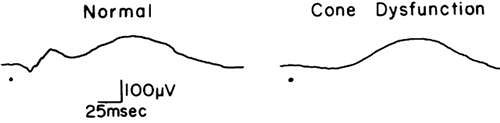 Figure 103.6. ERG response of the dark-adapted eye to a dim red flash. Left: Rod and cone systems respond with sufficient difference to allow separation of cone (initial positive response) and rod (second positive response) systems. Right: Patients with an absence of cones will show only the second (rod) portion of the ERG response. |
Standardized Protocol
To allow more reliable comparisons of ERGs between labs, a standardization of the clinical full-field ERG was established by an International Standardization Committee.5 The committee proposed standards for the following five commonly obtained responses:
A maximal response in the dark-adapted eye
A response developed by the rods (in the dark-adapted eye)
Oscillatory potentials
A response developed by the cone
Responses obtained to a rapidly repeated stimulus (flicker)
(For the details of the basic technology and clinical protocol see reference 5.)
Clinical Uses of the ERG
The ERG is helpful in diagnosing a number of disorders. It can be used:
To aid in the diagnosis of a generalized degeneration of the retina or to avoid the mistaken diagnosis of a generalized retinal degeneration
To assess family members, in cases where other individuals in the family have a known hereditary retinal degeneration
To aid in the diagnosis of patients presenting with decreased vision and nystagmus from birth
To assess retinal function in the presence of vascular occlusions
To assess retinal function with opaque media
To aid in a diagnosis when subjective complaints outweigh objective findings
Generalized Degeneration of the Retina
Among the multitude of generalized degenerations of the retina, retinitis pigmentosa is the best known. Although this term has been used generically to describe any generalized retinal degeneration, attention to a family history and evaluation of other family members; assessment of complaints that may indicate systemic disease, long-standing uveitis, or drug use; and careful evaluation of the ERG will help to clarify the diagnosis of disorders in this group and place them into better-defined entities (Table 103.1). It will also help to avoid a mistaken diagnosis of a generalized retinal degeneration.
Table 103.1. Generalized retinal degenerations | |
|---|---|
|
Any patient with a generalized heredoretinal degeneration, of which retinitis pigmentosa may be considered the prototype, has an abnormal ERG. In most cases, the ERG is extinguished or markedly reduced in amplitude and, in most instances, it has prolonged implicit times.6 In a few cases, usually early in the course of the disease, the ERG is affected only slightly in terms of amplitude (usually reduction of the b-wave), but the prolonged photopic implicit time directs the examiner to the appropriate diagnosis (Fig. 103.7).7
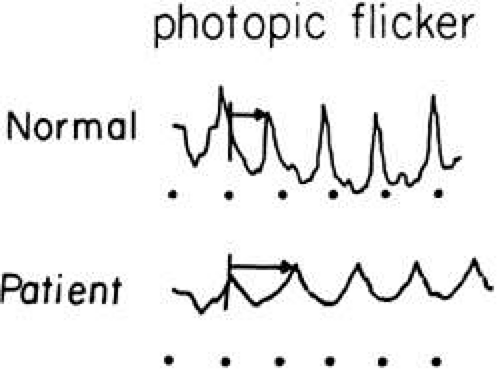 Figure 103.7. ERG recordings from a 14-year-old boy with documented autosomal dominant retinitis pigmentosa. His ERG shows a reduced amplitude and prolonged photopic implicit time, as compared with the normal. |
Case 1
A 49-year-old woman had poor night vision from childhood and recent difficulty going down stairs (Fig. 103.8). No family history of any similar disorder was known. The examination revealed vision at 20/25 OD, 20/20 OS. Both fundi showed slightly pale discs, attenuated arterioles, a moth-eaten appearance of the retina, and peripheral bone spicules. Visual fields were 10 degrees on a Goldmann perimeter (III-4E). The ERG was extinguished.
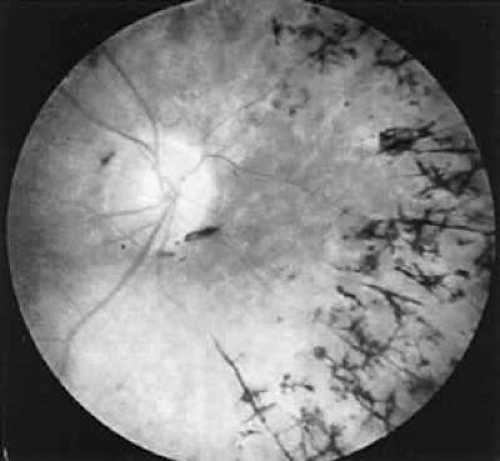 Figure 103.8. Case 1. See text for details. |
This is a classic case of retinitis pigmentosa, with the ERG providing confirmatory evidence to the typical history, clinical picture, and visual fields.
Case 2
A 5-year-old boy was seen for evaluation because of a family history of choroideremia (Fig. 103.9). His maternal grandfather had this disorder, but the patient and all other family members had no complaints. Examination revealed vision at 20/20 in each eye. Both fundi showed mild pigment granularity, but the discs and arterioles were normal. The ERG was markedly reduced in amplitude under all testing conditions.
 Figure 103.9. Case 2. See text for details. |
This boy has electrophysiologic evidence of a generalized tapetoretinal degeneration. More definitive fundus changes will appear in the future, and symptoms consistent with a widespread retinal degeneration will ensue. Evaluation of his mother showed funduscopic evidence of a choroideremia carrier state. All her psychophysical and electrophysiologic tests were normal.
Case 3
A 57-year-old woman was referred because of increasing complaints of difficulty with her night vision and her side vision (Fig. 103.10). She had a long history of low-grade uveitis and a progressive decrease in central vision. Examination revealed visual acuity of 20/100 OD, 20/80 OS. The vitreous showed multiple small cells. Both retinas showed narrowed arterioles and strands of pigment in the far periphery. Multiple areas of atrophy of the RPE were seen throughout. An ERG was extinguished.
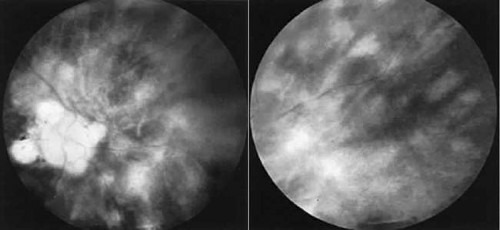 Figure 103.10. Case 3. Left: Posterior pole. Right: Peripheral retina. See text for details. |
This patient had birdshot choroiditis, an inflammatory disorder of the choroid with severe secondary photoreceptor degeneration. The ERG gives evidence of widespread degeneration, but the history and clinical findings preclude the diagnosis of a generalized heredoretinal degeneration. This disorder of birdshot choroiditis may produce a “pseudo-retinitis pigmentosa” picture (Table 103.2).8
Table 103.2. Pseudoretinitis pigmentosa | |
|---|---|
|
Case 4
A schizophrenic 29-year-old woman was seen for routine eye examination with vision of 20/20 in each eye and no ocular abnormalities noted (Fig. 103.11). She was seen for the second time 6 months later with complaints of a rapid decrease in central vision. Vision was 20/100 OD and OS. Both fundi showed heavy clumping of pigment throughout the macular area and a scattering of pigment granules throughout the rest of the retina. The ERG was extinguished.
 Figure 103.11. Case 4. See text for details. |
The ERG gives evidence of a widespread retinal degeneration. The clinical course and rapid change in the retinal picture is not found in retinitis pigmentosa. Further history revealed this patient to have been on high doses of Mellaril for the 5 months preceding her second evaluation. This known retinotoxic drug was indicted as the cause of the bilateral retinal degeneration.9
Case 5
A 2-year-old deaf boy was referred with a diagnosis of Usher syndrome (retinitis pigmentosa and deafness) (Fig. 103.12). His vision seemed good in both eyes, and the parents were unsure as to his ability to see in darkness. Both fundi showed a generalized granularity throughout. The ERG was normal.
 Figure 103.12. Case 5. See text for details. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


