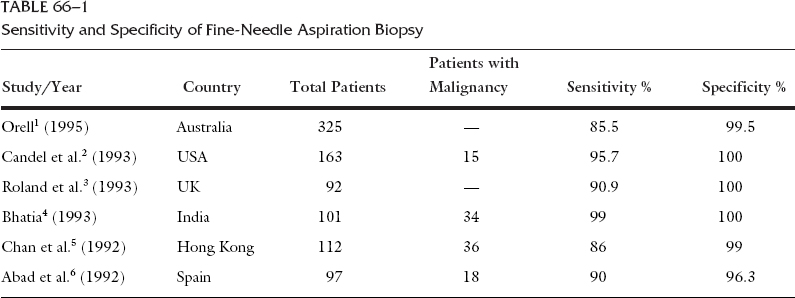
Most parotid masses represent benign neoplasms, most commonly pleomorphic adenoma, originating from the superficial lobe of the gland. Surgical excision is usually all that is required to provide both definitive diagnosis and adequate treatment. Despite this relatively simple algorithm, management of other types of parotid neoplasms is challenging because of their relative infrequency, inconsistent classification, and highly variable biologic behavior. These factors present some difficulty when one attempts to compare data from various institutions describing their experience with parotid tumors. However, some general features can be drawn from the literature regarding the incidence, pathology, and patterns of behavior of benign and malignant tumors of the parotid gland. Despite the large volume of literature describing these salient features, substantial controversy remains regarding several aspects of management of parotid tumors. Some of these controversies concern the role of fine-needle biopsy and high-resolution imaging in the diagnosis of parotid masses. Other controversies exist regarding the extent of resection in benign parotid tumors, management of the facial nerve, the role of elective neck dissection, and the indications of adjuvant radiotherapy. This chapter discusses some of these controversial issues. Fine-Needle Aspiration Biopsy The accuracy of fine needle aspiration biopsy (FNAB) in the diagnosis of salivary tumors has been well established. During the past 5 years, several studies from various countries have reported an exceptionally high degree of sensitivity and specificity. Examples of such studies are summarized in Table 66-1. The overall sensitivity ranges from 85.5% to 99%, and the overall specificity ranges from 96.3% to 100%.1–6 Diagnostic accuracy depends greatly on the experience of the cytopathologist, which in turn depends on the overall volume of patients with salivary neoplasms evaluated in any given institution. The reported sensitivity and specificity were slightly lower in community hospitals than at large academic centers.7 The most common source of diagnostic error is inadequate sampling. Among 582 FNABs of major and minor salivary glands, lack of cytologic and histologic correlation was noted in 21 cases. Of these, the cause in 10 FNABs was inadequate cytologic sampling of the lesion.8 In addition to being accurate, FNAB is safe, simple to perform, and relatively inexpensive. However, one essential question is worth asking. Is FNAB really necessary in the evaluation of parotid masses? Would it change the course of management based on clinical assessment? In an attempt to answer this question, Heller et al.9 performed a study to determine the impact of FNAB on patient management. In this study, 101 patients underwent FNAB of the major salivary gland masses. The physician’s initial clinical impression was compared with the FNAB diagnosis and the final diagnosis in each case. Overall, FNAB prompted a change in the clinical approach to 35% of patients. Examples of such changes in the planned management included avoiding a relatively large resection for lymphomas and sialadenitis. FNAB leads to better informed preoperative counseling of patients, alleviating an already high level of anxiety both to them and to their families.2 On the basis of these findings, the performance of FNAB may be helpful in treatment planning for patients who present with parotid masses.9 Imaging Studies The routine use of imaging in small well-defined masses of the superficial lobe of the parotid gland is probably not warranted, because imaging in such instances rarely alters the planned management. However, tumors presenting with clinical findings suggestive of malignancy, tumors arising from the deep lobe of the parotid gland, or tumors extending to the parapharyngeal space are better evaluated with high-resolution imaging. Computed tomography (CT) and magnetic resonance imaging (MRI) give a better understanding of the location and extent of the tumor, its relation to major neurovascular structures, perineural spread, and skull base invasion. Conventional radiography and sialography are rarely used because they provide little useful information. Nuclear imaging using technetium-99m pertechnetate is helpful only with oncocytic and Warthin’s tumors.10 Because aspiration needle biopsy can provide better information, nuclear imaging is rarely obtained. High-resolution ultrasound is useful in the hands of experienced radiologists and may detect calculi, abscesses, and cysts; it has been reported to assess up to 90% of benign versus malignant tumors correctly.11 Imaging modality of choice in evaluating parotid masses remains somewhat controversial among clinicians. Most of this controversy represents either personal or institutional bias, and there is a paucity of published data comparing the merits of different imaging modalities in the evaluation of parotid tumors. Some of these data are outlined herein. CT AND MRI Both CT and MRI provide information superior to that provided by other imaging techniques or by physical examination.12 To obtain the maximum amount of information possible, CT scanning should be performed with intravenous injection of contrast material. The normal parotid gland has a high fat content and is easily visualized on both CT and MRI; therefore, both techniques can demonstrate whether a mass is intra- or extraglandular. Generally, CT/MRI do not provide information regarding the specific histologic diagnosis, except rarely. An example of such a rare scenario is with lipoma of the parotid gland. However, CT/MRI can give useful information that may differentiate benign from malignant tumors. In contrast to benign tumors, which invariably have well-defined margins, malignant tumors usually exhibit irregular margins. Extension of the tumor beyond the confines of the gland can be adequately seen on both CT and MRI. Bony destruction of the mandible or skull base is best visualized on CT, whereas bone marrow involvement is better demonstrated on MRI. Both studies can adequately evaluate the neck for metastatic adenopathy. CT has the advantage of being less expensive and more available than MRI. However, CT images are more susceptible to degradation by dental artifact.12 MRI is superior to CT in demonstrating the internal architecture of salivary gland tumors in a multiplanar fashion, and in delineating the interface between tumor and normal salivary gland.13 Perineural spread of parotid malignancy along the facial nerve have a profound negative impact on survival and can drastically change the therapeutic plan, including the surgical approach and adjuvant therapy.14 Although perineural spread may present as abnormal nerve function, it often is asymptomatic. High-resolution imaging may be helpful in such cases in detecting perineural involvement. The criteria of nerve involvement on CT rely on bony changes along the course of the facial nerve. These changes include bone erosion, sclerotic margins, and widening of the normal diameter of the fallopian canal or stylomastoid foramen. However, these findings are late indicators of perineural spread. Perineural spread can be detected earlier on MRI, because of the better soft tissue delineation. The capability of MRI to detect the different signal intensity of tumor, fat, and nerve allow for better assessment of perineural spread. The criteria of nerve involvement on MRI include replacement of normal perineural fat with tumor, enhancement with gadolinium (regardless of size), and increased size of the nerve in question (regardless of enhancement). Using these criteria, MRI is more sensitive and specific in evaluating perineural spread than CT.14 Although parapharyngeal space masses are well visualized by both techniques, they are better delineated with MRI than CT. This is because of the different signal intensity of tumor, fat, and muscle on MRI. Most salivary tumors have low to intermediate T1 signal intensities and intermediate to high T2 signal intensities. The differential diagnoses of parapharyngeal masses include deep lobe parotid tumors, minor salivary gland tumors, and neurogenic and vascular tumors. Deep lobe parotid tumors and minor salivary gland tumors of the parapharyngeal space lie in the prestyloid compartment, anterior to the carotid artery, and displace the parapharyngeal fat medially. Deep lobe tumors are connected to the parotid gland at least in one imaging section. Minor salivary gland tumors are completely surrounded by fat.12 By contrast, neurogenic tumors and glomus tumors lie in the poststyloid compartment, posterior to the carotid artery, which is displaced anteriorly. Neurogenic tumors usually enhance intensely with gadolinium, whereas glomus tumors have a characteristic serpiginous flow voids (salt-and-pepper appearance) on MRI. OTHER IMAGING STUDIES Ultrasonography Ultrasonography has the advantage of being inexpensive, noninvasive, and simple to perform; it is also virtually free of complications. It can be used to differentiate solid from cystic masses in the parotid gland. Its use is limited by its ability to visualize only relatively superficial masses.12 Its value in evaluating the deep lobe of the parotid and the parapharyngeal space is hampered by the intervening mandibular ramus. Ultrasound guidance may improve the diagnostic accuracy of FNAB in complex masses of the parotid gland. Color Doppler Sonography Color duplex scanning is a noninvasive procedure that may be of help in the preoperative assessment of salivary gland tumors.15 Color doppler sonography has been recently used to evaluate the vascular anatomy of the salivary glands. It can distinguish between the physiologic changes that occur during salivary stimulation in normal subjects, and the flow alterations that occur in diseased glands. Specific patterns of peak systolic vascular shifts were described in various pathologic processes including Sjögren’s syndrome, pleomorphic adenoma, and malignant tumors.16 Positron Emission Tomography A recent study evaluated the ability of positron emission tomography (PET) to differentiate benign from malignant lesions of the salivary glands before surgery.17 Salivary gland masses were evaluated in 26 patients, using PET scans after the administration of fluorine-18-fluorodeoxyglucose (FDG). PET findings helped correctly differentiate benign from malignant masses in 69%, but were false-positive for malignancy in 31% of patients. The investigators concluded that FDG PET is not useful in classifying salivary gland tumors as benign or malignant.17 Extent of Resection for Benign Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


