Purpose
To determine the effect of pars plana vitrectomy (PPV) with inverted internal limiting membrane (ILM) flap technique for macular hole with or without retinal detachment in highly myopic eyes.
Design
Retrospective, interventional case series.
Methods
Ten eyes of 10 patients with macular hole with (4 eyes) or without (6 eyes) retinal detachment in high myopia (axial length more than 26.5 mm) were treated by PPV with inverted ILM flap technique.
Results
Macular hole closure was observed in 8 eyes (80%) following the initial surgery (in 5 eyes without retinal detachment and in 3 eyes with retinal detachment). In 4 eyes with retinal detachment caused by macular hole, retinas of 3 eyes were reattached by the initial surgery. Postoperative best-corrected visual acuity improved by more than 2 lines in 5 eyes (50%), was unchanged in 4 eyes (40%), and worsened by more than 2 lines in 1 eye (10%).
Conclusions
Inverted ILM flap technique might contribute to a high closure rate of macular hole and be a preferable adjuvant to the treatment of macular hole in high myopia with or without retinal detachment.
In highly myopic eyes, macular hole is one of the most vision-threatening complications, with or without retinal detachment caused by macular hole. Important causative factors of macular hole might be related to the tangential traction attributable to the premacular vitreous/membrane and the inverse traction attributable to the elongation of posterior staphyloma. However, the pathogenesis of macular hole in high myopia has not been clearly elucidated.
Surgical management of retinal detachment attributable to macular hole by pars plana vitrectomy (PPV) with gas tamponade was first reported in 1982. Since then, there have been many reports on the adjunctive procedures that can be used to improve the macular hole closure rate and the retinal reattachment rate, such as the removal of the epiretinal membrane (ERM), removal of the internal limiting membrane (ILM), endolaser photocoagulation of the macular hole rim, and silicone oil tamponade. The initial macular hole closure rates in high myopia after PPV with gas tamponade were reported to range from 25%-100%, with or without retinal detachment, which are poor anatomic success rates postoperatively compared with those of idiopathic macular hole.
On the other hand, Michalewska and associates reported the efficacy of inverted ILM flap technique for idiopathic large macular hole in 2010. According to the report, the inverted ILM flap technique prevents the postoperative flat-open appearance of macular holes and improves both the functional and anatomic outcomes of PPV for macular holes with a diameter greater than 400 μm. The mechanism of macular hole is different in highly myopic eyes vs nonmyopic ones. But regarding relatively poor macular hole closure rate and poor visual improvement, macular hole in high myopia is thought to be similar to idiopathic large macular hole in nonmyopia, which led us to hypothesize that the inverted ILM flap technique may be an effective treatment of macular hole in high myopia.
In the study described herein, we evaluated the effect of PPV with the inverted ILM flap technique for the treatment of macular hole with or without retinal detachment in highly myopic eyes.
Methods
This study is a retrospective and interventional case series. Each patient was informed about the risks and benefits of the surgery, and written informed consent was obtained in accordance with the guidelines for Otsu Red Cross Hospital, where this study was conducted. All investigations in this study adhered to the tenets of the Declaration of Helsinki. Since this was a study that retrospectively reviewed medical records and there were no confidentiality issues involved, the Institutional Review Board / Ethics Committee of Otsu Red Cross Hospital waived the need for approval of this research.
We reviewed the medical records of consecutive patients who had macular hole in high myopia and who were treated by PPV with the inverted ILM flap technique and sulfur hexafluoride (SF6) gas tamponade between January 13 and June 22, 2012. All patients underwent comprehensive ophthalmologic examinations, including measurement of axial length, best-corrected visual acuity (BCVA) using the 5-m Landolt C acuity chart, and dilated indirect and contact lens slit-lamp biomicroscopy. Axial length was measured preoperatively by A- and B-scan ultrasonography. When the measurements of axial length in an eye with retinal detachments were found to be abnormally low, the error was corrected using digital calipers to evaluate the distance from the cornea to the surface of retinal pigment epithelium rather than to the surface of the detached retina. Optical coherence tomography (OCT) examination was performed before and after surgery in all eyes using commercially available spectral-domain OCT (Spectralis HRA+OCT; Heidelberg Engineering, Heidelberg, Germany) to confirm whether the macular hole was closed after surgery. Macular hole closure was defined as the absence of a neurosensory defect over the fovea.
The information collected retrospectively from each of the medical records included age, sex, axial length, preoperative lens status, presence or absence of posterior staphyloma, retinal detachment and retinoschisis around the macular hole, area of staphyloma and retinal detachment, types of inverted membrane, preoperative and postoperative BCVA, presence or absence of reattachment and macular hole closure, and intraoperative and postoperative complications, if any. The area of staphyloma was determined based on the result of a dilated slit-lamp binocular ophthalmoscopy, and was graded according to the classification of Curtin.
The inclusion criteria were as follows: (1) clinical presentation of macular hole with or without retinal detachment; (2) an axial length of more than 26.5 mm in an eye with macular hole; (3) treatment with conventional 23-gauge 3-port PPV with the inverted ILM flap technique and SF6 gas tamponade; and (4) a follow-up period of more than 6 months from the last intraocular surgery. Eyes were excluded from the study if they had preexisting ocular diseases or a history of ocular surgery, except for cataract surgery. Other exclusion criteria included: (1) presence of peripheral retinal breaks before the primary surgery; (2) use of air tamponade, perfluoropropane (C3F8) gas tamponade, or silicone oil tamponade in the primary surgery; and (3) use of a trans-scleral approach such as macular buckling or scleral resectioning in the primary surgery.
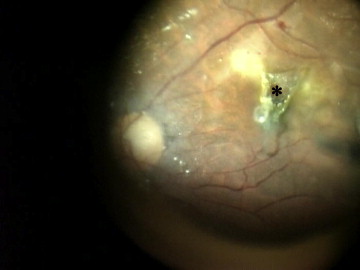
The study group included 10 eyes of 10 patients with macular hole with or without retinal detachment in high myopia. Phacoemulsification was performed on 2 phakic eyes prior to the PPV, with all of these undergoing an intraocular lens implantation. All the eyes included in this study were treated with conventional 23-gauge 3-port PPV. For this procedure, a posterior vitreous detachment was first created, followed by removal of the residual thin premacular posterior cortex. The peripheral vitreous was also excised. Triamcinolone acetonide was used intraoperatively to facilitate visualization of the vitreous and posterior hyaloids in all the eyes. The inverted ILM flap technique was basically performed according to the report of Michalewska and associates. Briefly, the ILM was peeled off in a circular fashion for approximately 2 disc diameters around the macular hole after the indocyanine green (ICG) staining procedure (0.125% solution of ICG). During the circumferential peeling, the ILM was not removed completely from the retina but was left attached to the edge of the macular hole. A rolled segment of the peeled ILM was hanging in the vitreous cavity. The ILM was then massaged gently over the macular hole from all sides until the ILM became inverted. If an ERM was present, it was peeled off with the same procedure used for the ILM. The macular hole was covered with the inverted ILM and ERM flap ( Figure 1 ). Drainage of subretinal fluid was not performed through the macular hole in all the cases with retinal detachment, but in 1 case (Patient 4) it was performed through the retinal hole intentionally created outside the macula. After fluid-air exchange, the air was then replaced with 20% SF6 gas. Patients were asked to maintain a prone position postoperatively for at least a week.
In follow-up visits at 1 week and 1, 2, 3, and 6 months postoperatively, all patients underwent visual acuity measurement, slit-lamp examination, indirect ophthalmoscopy, and OCT.
The BCVA was recorded in decimal acuity and converted to the logarithm of the minimal angle of resolution (logMAR) for statistical analyses. To evaluate the surgical effects, the preoperative and postoperative BCVA (logMAR value) were analyzed using the paired t test. A P value of <.05 was considered significant.
Results
In this study, 10 eyes of 10 patients were enrolled. Characteristics of the 10 eyes are shown in Table 1 . The mean age of the patients (2 male and 8 female) was 62.0 ± 13.0 years (range, 42-85 years). The mean preoperative BCVA (logMAR value) was 0.54 ± 0.46 (range, 0.15-1.52). The mean axial length was 29.5 ± 2.0 mm (range, 26.7-33.0 mm). Seven eyes had staphyloma of type 1 (posterior pole staphyloma) or type 2 (macular staphyloma), as per the classification of Curtin. Four eyes had retinal detachment caused by the macular hole. Two eyes were phakic and 8 were pseudophakic.
| Factors | All Cases (n = 10) |
|---|---|
| Mean age ± SD, y | 62.0 ± 13.0 |
| Range | 42-85 |
| Sex, n (%) | |
| Male | 2 (20%) |
| Female | 8 (80%) |
| Mean BCVA ± SD, logMAR units | 0.54 ± 0.46 |
| Mean axial length ± SD, mm | 29.5 ± 2.0 |
| Staphyloma, n (%) | |
| + | 7 (70%) |
| − | 3 (30%) |
| Retinoschisis around MH, n (%) | |
| + | 2 (20%) |
| − | 8 (80%) |
| Area of MHRD, n (%) | |
| None | 6 (60%) |
| Within staphyloma | 2 (20%) |
| Beyond staphyloma | 2 (20%) |
| Lens status, n (%) | |
| Phakic | 2 (20%) |
| Intraocular lens | 8 (80%) |
Of the 10 eyes, 8 (80%) had initial macular hole closure after the primary PPV with the inverted ILM flap technique ( Table 2 ). Initial macular hole closure was obtained in 3 of 4 eyes with retinal detachment and in 5 of 6 without retinal detachment. Three of the 4 eyes with retinal detachment had initial retinal reattachment after the primary PPV. One eye with initial failure underwent PPV with silicone oil tamponade after the initial surgery and had final retinal reattachment. There were no intraoperative and postoperative complications in any cases.
| Patient No. | Age (y) | Sex | Axial Length (mm) | Posterior Staphyloma | Retinoschisis Around MH | MHRD (Area of RD) | Preop BCVA | Inverted Membrane | MH | Postop BCVA |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 69 | M | 31.1 | + | − | + (beyond PS) | 0.07 | ILM | Closed | 0.2 |
| 2 | 85 | F | 27.9 | + | − | + (within PS) | 0.7 | ERM+ILM | Closed | 1.0 |
| 3 | 76 | F | 29.5 | + | + | − | 0.5 | ERM+ILM | Closed | 0.6 |
| 4 | 50 | M | 27.9 | + | − | + (beyond PS) | 0.2 | ILM | Closed | 0.8 |
| 5 | 57 | F | 26.8 | + | − | + (within PS) | 0.03 | ILM | Open | 0.15 |
| 6 | 55 | F | 26.7 | − | − | − | 0.4 | ERM+ILM | Closed | 0.4 |
| 7 | 42 | F | 30.5 | − | − | − | 0.7 | ILM | Closed | 1.2 |
| 8 | 69 | F | 30.2 | − | − | − | 0.3 | ERM+ILM | Closed | 0.4 |
| 9 | 53 | F | 33.0 | + | + | − | 0.6 | ILM | Closed | 0.7 |
| 10 | 64 | F | 31.7 | + | − | − | 0.5 | ILM | Open | 0.3 |
Postoperative BCVA improved by more than 2 lines in 5 eyes (50%), was unchanged in 4 eyes (40%), and worsened by more than 2 lines in 1 eye (10%). The mean postoperative BCVA (logMAR value) was 0.32 ± 0.30 (range, −0.08 to 0.82). There was a significant difference in the BCVA before vs after the surgery ( P = .019).
Case 1
An 85-year-old woman presented with retinal detachment within posterior staphyloma caused by macular hole. OCT demonstrated retinoschisis around the macula ( Figure 2 , Top). Her initial BCVA was 0.7. By primary PPV with the inverted ILM flap technique, the ERM and ILM were inverted. One week after surgery, the retina was reattached and the macular hole was closed ( Figure 2 , Bottom). Postoperative BCVA improved to 1.0.



