Purpose
To determine whether the risk of graft failure in patients with glaucoma is dependent on the indication for penetrating keratoplasty (PK).
Design
Retrospective cohort study.
Methods
All patients on the United Kingdom Transplant Registry undergoing their first PK over a 7-year period with at least 1 year of follow-up were included. Data were collected on indication for PK, presence and management of glaucoma, graft diameter, recipient risk factors, and graft survival. Kaplan-Meier survival curves, a Cox regression model, and χ 2 and t tests were used in group comparisons.
Results
A total of 6255 transplants in eyes without glaucoma and 1994 in eyes with glaucoma were analyzed. Three-year transplant survival was 86% and 72% respectively ( P < .0001), and 73% in eyes with medically managed glaucoma compared to 63% in surgically managed glaucoma ( P = .07). Glaucoma patients undergoing PK for pseudophakic bullous keratopathy or Fuchs dystrophy had significantly increased relative risks of graft failure (1.5 and 1.9 with topical and 2.0 and 3.1 with oral antiglaucoma medication respectively, compared to those without glaucoma). There was no equivalent significant difference for those with keratoconus, previous noncataract ocular surgery, trauma, or noninfectious ulcerative keratitis. Endothelial decompensation accounted for a significantly greater proportion of graft failure in recipients with glaucoma (topical [9%] and oral medication [13%]) than in those without glaucoma (3%) ( P < .001).
Discssion
The presence of glaucoma carries an increased risk of graft failure, in particular from endothelial decompensation. This risk is, however, also dependent on the indication for PK, with transplants undertaken for primary corneal endothelial disease carrying a higher risk.
There is complex interaction between factors influencing outcome of penetrating keratoplasty (PK) and glaucoma management. PK is recognized as a risk factor for both the development and deterioration of glaucoma and, conversely, glaucoma itself is a risk factor for graft failure. The Australian Corneal Graft Registry attributed 8.5% of failed grafts to glaucoma and its treatment and a history of increased intraocular pressure (IOP) pre- or at transplant was associated with a 1.45 to 3.34 increased relative risk of graft failure.
Although the role of glaucoma in corneal graft failure has been recognized for many years, it is unclear if the effect of glaucoma on graft survival is intrinsically linked to the underlying corneal disease and/or dependent on other recipient risk factors. In order to investigate whether the effect of glaucoma on survival was related to the indication for transplantation, an analysis was undertaken of transplants in eyes with and without glaucoma, examining the indication for graft, medical and surgical glaucoma treatment, and other recipient risk factors for graft failure such as vascularization and ocular surface disease.
Methods
All penetrating corneal transplants registered by the United Kingdom (UK) Transplant Registry between April 1999 and March 2006, in recipients aged 17 years or above undergoing their first transplant and for whom follow-ups were completed for at least 1 year, were included. These data are held by the National Health Service Blood and Transplant (NHSBT). As in other reports, patients were classified as having glaucoma at the discretion of their treating ophthalmologist based upon 1 or more features of intraocular pressure elevation, optic disc damage, and visual field changes. A breakdown of this information regarding the type of glaucoma was not available to us. Patients were, however, classified according to whether they had 1) been treated by topical or oral glaucoma medication either prior to or following PK or 2) undergone glaucoma surgery at the time of or following PK. Data on recipient eyes and transplants recorded at registration include indication for PK, previous intraocular surgery, transplant diameter, presence of risk factors for rejection (inflammation and vascularization), medications, and previous rejection episodes, as previously described. Follow-up data routinely collected at 1, 2, and 5 years post-transplant include graft failure date, best-corrected visual acuity (BCVA), glaucoma, and steroid medications.
Statistical analyses were performed using SAS v9.1 software (SAS Institute Inc, Cary, North Carolina, USA). χ 2 tests and t tests were used, respectively, to investigate differences in categorical and continuous variables. Kaplan-Meier survival curves were used to determine graft survival and a Cox regression model was fitted to investigate the influence of glaucoma on graft survival while adjusting for other known factors. Visual acuity data were converted into logMAR units for analysis, and refractive data were transformed into Long’s matrix formalism and analyzed by the method of Kaye and Harris. The refractive error data are presented in spherocylinder form with the magnitude of the cylinder, treated as a scalar value, also included in square brackets, that is, sphere/cylinder[cylinder] axis.
Results
There were 8249 first PKs for which follow-up was reported to the UK Transplant Registry, of which there were 1994 eyes with glaucoma (24%). The return rate of completed postoperative data within the first 3 years was 85%. The mean ages at PK surgery were 57 years (SD 22 years) for patients without glaucoma (female-to-male ratio: 49:51) and 65 years (SD 19 years) for patients with glaucoma (female-to-male: 47:53).
Indications for Transplant
There were significantly more (P < .0001) patients with glaucoma undergoing PK for pseudophakic or aphakic bullous keratopathy (PBK or ABK) than without glaucoma: total 809 of 1994 (41%) vs 1138 of 6225 (18%). Conversely, of the patients without glaucoma, significantly more ( P < .0001) underwent PK for keratoconus or Fuchs dystrophy than of those with glaucoma (29% vs 11% and 25% vs 16% respectively). These data are shown for all indications in Table 1 .
| Nonglaucoma | Glaucoma | Total | ||||
|---|---|---|---|---|---|---|
| Indication | N | % | N | % | N | % |
| Keratoconus | 1828 | 29.4 | 222 | 11.1 | 2050 | 24.9 |
| Fuchs dystrophy | 1529 | 24.6 | 326 | 16.4 | 1855 | 22.5 |
| Pseudophakic bullous keratopathy | 1017 | 16.3 | 698 | 35.0 | 1715 | 20.8 |
| Aphakic bullous keratopathy | 121 | 1.9 | 111 | 5.6 | 232 | 2.8 |
| Infection | 654 | 10.5 | 190 | 9.5 | 844 | 10.3 |
| Trauma | 171 | 2.8 | 75 | 3.8 | 246 | 3.0 |
| Noninfectious ulceration | 210 | 3.4 | 53 | 2.7 | 263 | 3.2 |
| Unknown opacification | 306 | 4.9 | 79 | 4.0 | 385 | 4.7 |
| Other | 389 | 6.3 | 240 | 12.0 | 639 | 7.8 |
| Total | 6225 | 1994 | 8229 | |||
Graft Survival
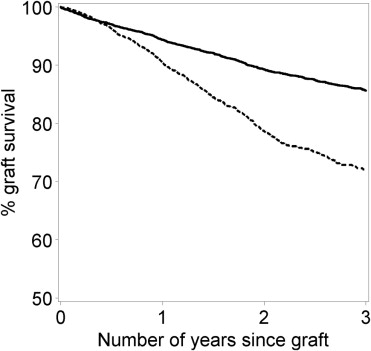
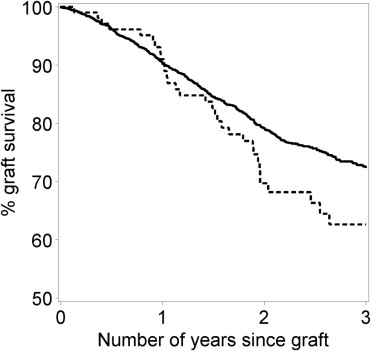
Univariate Kaplan-Meier curves showed that 3-year graft survival was lower for patients with glaucoma compared to patients without glaucoma ( Figure 1 ): 72% (95% confidence interval [CI] 70-74) and 86% (95% CI 85-87) respectively (P < .0001). Graft survival was also lower for patients who underwent glaucoma surgery compared to those whose glaucoma was managed by medical therapy alone ( Figure 2 ): 63% (95% CI 51-72) and 73% (95% CI 70-75) respectively ( P < .0001). For patients who had either combined PK glaucoma surgery (n = 32) or post-PK glaucoma surgery (n = 72), graft survival was 68% (95% CI: 45-83) and 60% (95% CI: 46-72), respectively ( P = .5).
After adjustment for a number of confounding factors, the risk of graft failure was higher for both patients with glaucoma ( Table 2 ). Graft survival, however, was also dependent on the indication for PK, that is, keratoconus (94%), Fuchs dystrophy (91%), PBK (71%), ABK (70%), infection (72%), injuries (69%), ulceration (61%), unknown opacification (85%), and other (78%) (data not shown). Relative to the risk of graft failure for patients with keratoconus, the risk of graft failure was significantly increased for patients with all other indications ( Table 2 ). In terms of other risks factors, ocular surface inflammation and infection/inflammation carried increased relative risks of graft failure of 1.5 and 1.4 respectively.
| Factor | No. of Patients | Relative Risk (95% CI) | P |
|---|---|---|---|
| Indication for graft | |||
| Keratoconus | 2028 | 1.0 | |
| Fuchs dystrophy | 1829 | 1.5 (1.2-2.0) | .002 |
| Pseudophakic bullous keratopathy | 1692 | 3.9 (3.1-5.0) | <.0001 |
| Aphakic bullous keratopathy | 230 | 3.8 (2.6-5.3) | <.0001 |
| Infection | 827 | 3.3 (2.5-4.3) | <.0001 |
| Trauma | 242 | 4.4 (3.2-6.2) | <.0001 |
| Noninfectious ulceration | 257 | 3.7 (2.6-5.3) | <.0001 |
| Unknown opacification | 378 | 2.2 (1.5-3.1) | <.0001 |
| Other | 633 | 2.8 (2.1-3.7) | <.0001 |
| Preoperative glaucoma | |||
| No | 7309 | 1.0 | |
| Yes | 807 | 1.5 (1.3-1.8) | <.0001 |
| Postoperative glaucoma medication | |||
| None | 6471 | 1.0 | |
| Topical | 1417 | 1.2 (1.0-1.4) | .02 |
| Oral with/without topical | 228 | 1.5 (1.2-2.0) | .002 |
Graft Survival in Patients With and Without Glaucoma According to Indication for PK
For patients undergoing PK for PBK/ABK there was a significant reduction in graft survival between patients with and without glaucoma (63%, n = 809, 95% CI: 59-67 vs 77%, n = 1138, 95% CI: 73-80, P < .0001). The risk of graft failure was higher if on topical or oral antiglaucoma medication ( Table 3 ). Excluding PBK and ABK, for patients who had previous ocular surgery, although there was a reduction in graft survival, there was no statistically significant difference between those with and without glaucoma (62%, n = 62, 95% CI: 50-73 vs 75%, n = 39, 95% CI: 57-87, P = .2) (data not shown).
| Factor | No. of Patients | Relative Risk (95% CI) | P |
|---|---|---|---|
| Fuchs dystrophy | |||
| Postoperative glaucoma medication | |||
| None | 1549 | 1.0 | |
| Topical | 255 | 1.9 (1.2-2.8) | .001 |
| Oral with/without topical | 25 | 3.1 (1.3-7.5 | .01 |
| Pseudophakic bullous keratopathy | |||
| Postoperative glaucoma medication | |||
| None | 1131 | 1.0 | |
| Topical | 474 | 1.5 (1.2-1.9) | .0003 |
| Oral with/without topical | 87 | 2.0 (1.4-2.9) | .0002 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


