12 Ear and Temporal Bone Trauma • Auricular haematoma: risk of “cauliflower ear” if inadequately aspirated/drained • Earring “pull-outs”: repair under local anaesthetic (LA) • Bites/lacerations: washout, debridement, closure under LA ± antibiotics • Amputations: place ear in saline gauze, in plastic bag, on ice; consider referral to plastics for replantation if feasible • Traumatic tympanic membrane (TM) perforations: ~95% heal by 6 weeks after injury • Water exclusion and treat concurrent infection if present • Consider possibility of ossicular injury—pure tone audiogram • TM injuries common • Implantation cholesteatoma possible • Conductive hearing loss (HL) (from TM or ossicular chain damage) or sensorineural hearing loss (SNHL) (from impulse noise) • Vertigo usually temporary • Tissue injury caused by a change in pressure that compresses or expands gas contained in body structures • Middle ear (ME) is a noncompressible gasfilled space • In diving, failure of eustachian tube (ET) to open causes squeeze effect in ME: – Explosive injury: on descent if inadequate ET function, negative ME pressure relative to intra-labyrinthine fluid pressure; increasing cerebrospinal fluid (CSF) fluid pressure then transmitted to inner ear via cochlear aqueduct, which further increases pressure differential between labyrinthine fluid and ME space and causes outward bulging and rupture of RW – Implosive injury: on descent relative negative pressure develops in ME and TM retracts; if ET functioning normally sudden forceful Valsalva to equilibrate; TM approaches neutral position; relative positive pressure of ME compared with intralabyrinthine fluids so RW pushes inwards and can rupture • Other: canal “squeeze” from impacted wax; vestibular symptoms (perilymphatic fistula, caloric effect through perforation, labyrinthine decompression sickness where bubbles causing ischemia to labyrinth via AICA) • Half a million head injuries each year; up to a quarter include symptoms related to injury of the temporal bone • Various classifications, e.g., longitudinal or transverse fractures (#s) relating to orientation of fracture line; however, >80% mixed; otic capsule involvement may be a more relevant way to classify • Longitudinal (Fig. 12.1):
12.1 Pinna
12.2 Tympanic Membrane
12.3 Blast Injuries
12.4 Barotrauma
 As descend, gas compresses, TM retracts, Valsalva to open ET and equalize—pain common
As descend, gas compresses, TM retracts, Valsalva to open ET and equalize—pain common
 As ascend, increased gas volume aids equalization through ET (if pressure differential >15 mm Hg)
As ascend, increased gas volume aids equalization through ET (if pressure differential >15 mm Hg)
 Rapid change in relative pressure of ME can cause implosive or explosive forces on TM, round window (RW), or oval window:
Rapid change in relative pressure of ME can cause implosive or explosive forces on TM, round window (RW), or oval window:
 Both implosive and explosive barotrauma to inner ear can cause sudden SNHL; tinnitus and vertigo possible; large pressure differences can also cause TM rupture
Both implosive and explosive barotrauma to inner ear can cause sudden SNHL; tinnitus and vertigo possible; large pressure differences can also cause TM rupture
 Increased risks with ET dysfunction, rhinosinusitis/allergy
Increased risks with ET dysfunction, rhinosinusitis/allergy
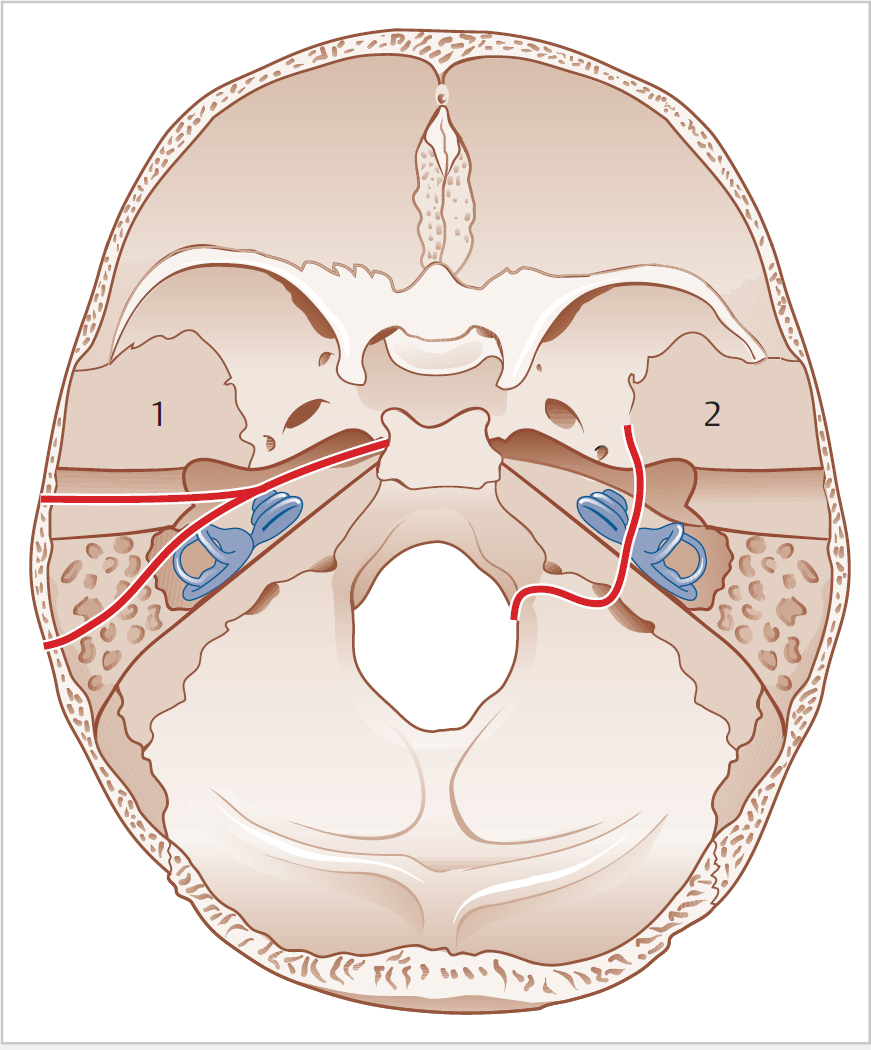
12.5 Temporal Bone Fractures
 Dominant in 80%; usually blow to side of head
Dominant in 80%; usually blow to side of head
 Symptoms mainly related to ME
Symptoms mainly related to ME
 # runs from squamous temporal bone in roof of external auditory canal to TM and roof of ME, then anterior towards labyrinth
# runs from squamous temporal bone in roof of external auditory canal to TM and roof of ME, then anterior towards labyrinth
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


