Eales’ Disease
Marissa L. Albano
Robert P. Murphy
Eales’ disease is an idiopathic obliterative vasculopathy of the peripheral retina. Vascular sheathing and focal occlusion of small peripheral retinal vessels occur early in the course of the disease. With progression, large areas of nonperfusion can develop and extend posteriorly. Neovascularization can occur, usually at the junction of the perfused and nonperfused retina, frequently resulting in vitreal hemorrhages. This disease can affect persons of all ages, but is predominantly noted to affect young, healthy males. The etiology currently remains unclear, but recent studies have indicated a multifactorial pathogenesis including mycobacterium tuberculosis, retinal autoimmunity, human leukocyte antigen, and free radical mediated damage.
The disease is named after Henry Eales, an ophthalmologist who in 1880 described a syndrome of recurrent vitreal hemorrhages in young men with epistaxis and constipation.1 He noted abnormal retinal veins and attributed the hemorrhages to increased venous pressure caused by constipation. He did not observe any new vessels or inflammation preceding or accompanying the hemorrhages. The association with constipation and epistaxis has long since been disproved, and nonperfusion, inflammation, and neovascularization subsequently have been associated with this disease.
In 1967, Duke-Elder believed that Eales’ disease was not a specific entity and that it represented the clinical manifestation of many diseases.2 Since then, refined diagnostic tests have demonstrated that many “idiopathic” hemorrhages were caused by known etiologies such as sarcoidosis, systemic lupus erythematosus, diabetes mellitus, sickle cell disease, and collagen vascular disease.
However, after elimination of these causes, a group of patients with idiopathic peripheral nonperfusion and perivasculitis of the retina remains. Investigators now generally agree that Eales’ disease is a distinct entity comprising characteristic funduscopic and fluorescein angiographic features.3
Epidemiology
Eales’ disease is uncommon in North America; however, this disorder is responsible for widespread visual loss in India, Pakistan, and Afghanistan. The incidence in India has been reported as 1 in 200 to 250 ophthalmic patients,4 and up to 1.35% in an ophthalmic referral center.5 It typically affects healthy young adults between their third and fourth decades of life. Patients usually present with symptoms of vitreal hemorrhage, such as floaters or decreased vision. The majority of patients develop bilateral involvement, although unilateral occurs as well. Most reports, including Henry Eales’ original description, indicate a male predominance. However, recent reports suggest a similar prevalence among both men and women.6
Clinical Features
Early in its course, signs of ocular inflammation are encountered in Eales’ disease. Vascular sheathing is seen in most patients (Fig. 1). The degree of sheathing ranges from thin, continuous white lines on both sides of the blood column to heavy, segmental exudative sheathing. Areas of sheathing frequently leak dye with fluorescein angiography (Fig. 2). However, there is not a direct correlation between the regions of sheathing and staining.
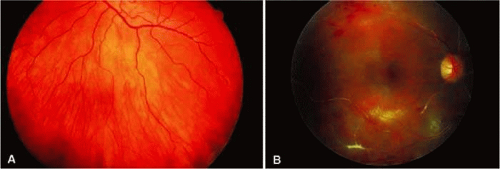 FIGURE 1. Vascular sheathing. A. Thin white lines surround retinal venule. B. Exudative-type arteriolar sheathing. |
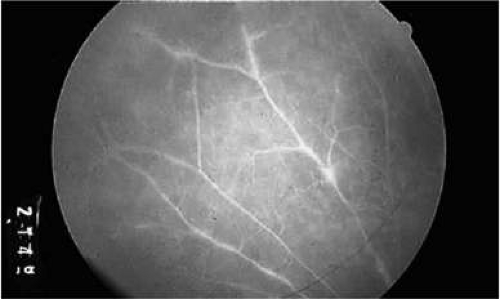 FIGURE 2. Fluorescein angiogram demonstrating abnormal vascular staining in a patient with Eales’ disease. There was venous sheathing in these areas. |
Henry Eales first described the disease to affect retinal veins, and other investigators, such as Elliot and Harris, suggested the term periphlebitis retinae for this disorder.7 However, recent reports suggest equal involvement of arteriolar and venular sheathing.7 Because of the evidence of arteriolar involvement (see Fig. 1B), this disease is considered a retinal vasculitis or vasculopathy. Others have used the term primary retinal perivasculitis.8 Cystoid macular edema, vitreal cells, keratic precipitates, and anterior chamber cell and flare have been observed in patients with Eales’ disease.3
Peripheral retinal nonperfusion is present in all patients with this disease. The nonperfusion is generally confluent and sharply demarcated from the posterior perfused retina (Fig. 3). Fine white lines representing the remains of obliterated large vessels (ghost vessels) often are seen in the area of nonperfusion. The temporal retina is most commonly affected.
 FIGURE 3. Fluorescein angiogram of the peripheral retina demonstrates the junction of normally perfused retinal vessels adjacent to an area of nonperfused retina. Notice the vascular abnormalities at the junction. |
Elliot and Spitnas et al. have documented the abnormalities at the junction between the anteroperipheral nonperfused and the posterior perfused retina.9,10 Intraretinal hemorrhages often first appear in the affected area, followed by an increase in vascular tortuosity with frequent collateral formation around occluded vessels (see Fig. 3). Microaneurysms, arteriovenous shunts, and venous beading are commonly seen at the junction (Fig. 4). Fluorescein angiography enhances these abnormalities and often demonstrates staining at the stumps of obliterated vessels.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


