Chapter 20 Dural Herniation and Cerebrospinal Fluid Leaks
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
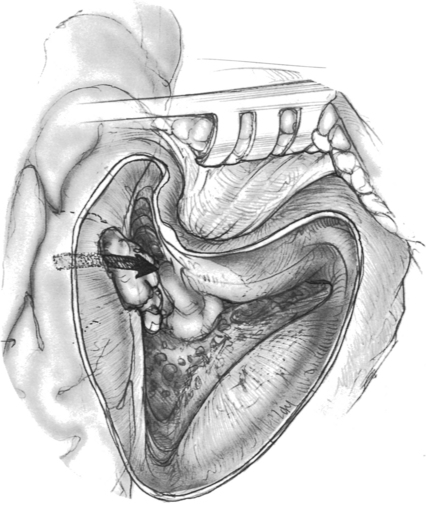
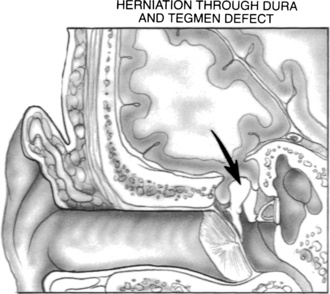
An encephalocele occurs when brain tissue herniates through a dural defect of the skull. Temporal bone encephaloceles manifest either as a mass or cerebrospinal fluid (CSF) in the middle ear or mastoid or both (Figs. 20-1 and 20-2). Encephaloceles have also been called dural herniations, brain herniations, brain prolapse, and meningoencephalocele. They have been documented since the early 1900s.1,2 They were associated with chronic suppurative otitis media and transmastoid surgery, but, with a decreasing incidence of otogenic intracranial complications in modern-day patients, they have become uncommon. Contemporary otologic literature describes a myriad of signs and symptoms that are frequently not associated with suppurative disease.3
Other causes include congenital cranial base defects, spontaneous hernias, and trauma. Iurato and associates4 reviewed 139 cases of temporal bone encephaloceles, and found that 59% occurred as a complication of mastoid surgery, 21% were spontaneous or idiopathic, 9% were a complication of chronic otitis media or chronic mastoiditis, and 9% resulted from trauma. More recently, Scurry and coworkers5 reported encephalocele formation associated with morbid obesity in eight patients. The middle cranial fossa is the most common site of occurrence; encephaloceles rarely originate from the posterior fossa.6
PATHOGENESIS
Basic knowledge of the embryology of the temporal bone is helpful in the understanding of formation of dural herniation and CSF leaks. There are four ossification centers that form the temporal bone: squamous, tympanic, petrous, and mastoid. Pneumatization follows ossification and continues into adulthood and consists of a process of marrow resorption, mucosal advancement, and bone remodeling. Disturbances in the normal ossification or pneumatization process may lead to encephalocele formation. Portions of the petrous and squamous ossification centers of the temporal bone ultimately form the roof of the middle ear and mastoid, areas that are the most likely to form encephalocele.7
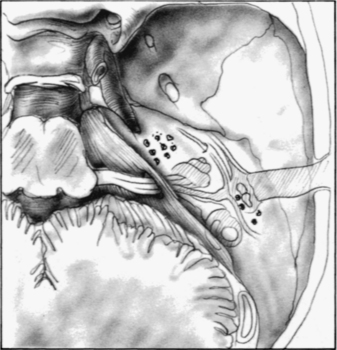
Many authors have reported multiple tegmen defects (Fig. 20-3). Ahern and Thulen8 noted a 6% incidence of multiple defects in the tegmen in 94 consecutive cadaveric specimens. Ferguson and colleagues6 noted a 22% incidence of multiple tegmen defects in 27 preserved dried temporal bones. Lang9 found tegmen defects in 20% of 70 temporal bones. Bilateral spontaneous encephaloceles could be predicted from such studies, and have been reported by Iurato and colleagues.10
The high incidence of tegmen defects is contrasted by the low incidence of spontaneous encephalocele and CSF leak formation. This observation lends credibility to the widely held belief that bony defects are necessary, but not solely responsible, for the formation of encephaloceles. The other factor that is necessary for encephalocele formation is a pathologic process at the dural level. Inflammatory process, chronic suppurative otitis media, and transmastoid surgery are the most common factors in the dura. Other factors, such as benign intracranial hypertension, obesity, and aging, also have been suggested.5,11
The association with chronic suppurative otitis media and transmastoid surgery is well documented in the literature.4,12,13 In the preantibiotic era, meningeal complications from chronic suppurative otitis media were common. The incidence of encephalocele during this period was increased by transmastoid trephination of peridural and brain abscesses. Encephalocele can occur in the face of chronic suppurative otitis media with or without surgery, with or without cholesteatoma.14,15 Paparella and coworkers16 reported 10 cases of encephalocele all associated with chronic otitis media, 6 of which had not had previous surgery, and 2 of which had cholesteatoma. These authors speculated that the inflammatory response led to destruction of the tegmen, followed by extension to adjacent dura and brain, resulting in herniation. Encephalocele formation can form when a dural tear occurs at the site of a bone dehiscence from a drill, scalpel, or cautery.12 Dural injuries may go unrecognized during the surgery; however, if recognized at the time of surgery, they should be repaired to prevent an immediate or delayed problem. Although chronic suppurative otitis media and transmastoid surgery are still the most common causes for encephalocele and CSF leak, a decreasing incidence has been cited because of improved surgical techniques, including the operating microscope and the use of drills versus gouges and chisels.17
CSF leak secondary to head trauma is well documented. Dura in the skull base that is adherent to adjacent bone tears along fracture lines. CSF leak usually resolves spontaneously or with lumbar drainage within 1 to 2 weeks. Savva and coworkers18 managed 26 of 29 patients with CSF otorrhea secondary to head injury successfully with conservative treatment. In contrast, only 1 of 53 patients with surgically induced or spontaneous CSF leak was successfully managed conservatively. Bony dehiscence and dural injury from head trauma can lead to either immediate or delayed encephalocele formation.
Spontaneous encephalocele and CSF leak has been attributed to multiple factors. Arachnoid granulations of the temporal bone may be a cause of spontaneous encephalocele and CSF fistula formation. Normally, arachnoid granulations protruding into the lumen of venous structures are involved in the resorption of CSF. When not associated with venous structures and surrounded by bone, they may enlarge and cause bone erosion as a result of intermittent subarachnoid pressure associated with age and physical activity. Gacek19 observed in temporal bones that in the tegmen tympani and mastoideum 22% had tissue on the dural surface, and 9% had tissue in the posterior fossa.
Rao and colleagues11 reported a series of 10 patients with spontaneous CSF leak with an average age of 58 and an increased incidence in women. They hypothesized that the increased incidence in women suggested an association with benign intracranial hypertension, although many of their patients did not have clinical findings. Scurry and colleagues5 reported an association of morbid obesity in eight patients with spontaneous CSF leak. They also posited a theory that obesity ultimately resulted in increased intracranial pressure and subsequent CSF leakage and encephalocele formation. Many of their patients did not have findings consistent with increased intracranial pressure, which questions the idea that it plays a significant role.
DIAGNOSIS
Diagnosis of encephalocele and CSF leak is primarily clinical with supportive radiologic and laboratory information. Clinical findings may or may not include a history of chronic suppurative otitis media or trauma. Middle ear effusion with conductive hearing loss is the most common presenting symptom.19–21 A subsequent myringotomy and tube results in a persistent clear, odorless, watery type of discharge.22–24 Leakage may vary with various maneuvers that increase intracranial pressure, such as supine positioning, Valsalva maneuver, and compression of the jugular vein.25 Leaning forward may elicit rhinorrhea.
A mass in the ear canal or behind the tympanic membrane is a rarely described finding.26,27 A more common finding is a soft compressible mass in the mastoid cavity arising off the tegmen that may mimic a blue dome cyst or cholesterol granuloma.28,29 Less common presentations include meningitis and seizures.2,6,17,28,30–36 Tension pneumocephalus is another uncommon presentation of temporal bone encephalocele.37
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


