Disorders of the Facial Nerve: Introduction
Facial nerve dysfunction can dramatically affect a patient’s quality of life. The human face is a focal point for expression and interpersonal communication, whereas facial motor movement contributes to eye protection, speech articulation, chewing and swallowing, and emotional expression. Thus, the patient with a facial palsy suffers not only the functional consequences of impaired facial motion but also the psychological impact of a skewed facial appearance.
Acute Facial Palsies
Bell’s Palsy
- Acute onset, with unilateral paresis or paralysis of the face in a pattern consistent with peripheral nerve dysfunction (all branches affected).
- Rapid onset and evolution (<48 hours).
- Facial palsy may be associated with acute neuropathies affecting other cranial nerves (particularly, cranial nerves V–X).
Herpes Zoster Oticus (Ramsay Hunt syndrome)
- Acute peripheral facial palsy associated with otalgia and varicella-like cutaneous lesions that involve the external ear, skin of the ear canal, or the soft palate.
- Involvement often extends to cranial nerves V, IX, and X, and cervical branches that have anastomotic communications with the facial nerve.
- Differentiated from Bell’s palsy by characteristic cutaneous ulcers and a higher incidence of hearing loss or balance dysfunction.
There are a variety of disorders that may be associated with unilateral facial palsies (Table 70–1). Bilateral facial palsy is much less frequent and occurs in less than 2% of patients presenting with an acute facial palsy (Table 70–2). Bilateral involvement typically reflects a systemic disorder with multiple manifestations. Because of their overlapping clinical presentation and treatment paradigms, Bell’s palsy and herpes zoster oticus (also known as Ramsay Hunt syndrome) will be considered together.
|
|
No identifiable cause is present for approximately 60–70% of cases of acute facial palsy. The clinical diagnosis of Bell’s palsy is appropriately applied in such cases. Bell’s palsy reveals several characteristics. The onset is that of an acute, unilateral paresis or paralysis of the face in a pattern consistent with peripheral nerve dysfunction (Figure 70–1). The onset and evolution are rapid—typically less than 48 hours. There may also be subtle but frequent associated dysfunction of cranial nerves V, VIII, IX, and X in association with Bell’s palsy. Pain or numbness affecting the ear, mid-face, and tongue as well as taste disturbances are common. These observations suggest that the facial weakness seen in Bell’s palsy is the inflammatory facial-motor component of a wider cranial polyneuropathy that is induced by viral agents admitted through mucosal membranes.
Figure 70–1.


(A)Prototypic case of Bell’s palsy. This 28-year-old woman experienced the onset of an acute, left-sided paralysis of the face over a 24-hour period, in a pattern consistent with peripheral nerve dysfunction. Treatment consisted of oral steroid dosing at pharmacological doses for 10 days, followed by a 2-week taper. (B) Full recovery of facial motor function 2 months after onset.
Recurrent facial palsy consistent with Bell’s palsy occurs in 7–12.0% of patients. Ipsilateral recurrences approximate contralateral involvement. Recurrences are more likely in patients with a family history of Bell’s palsy and the incidence of diabetes mellitus in recurrent Bell’s palsy patients is 2.5 times that noted in nonrecurrent cases. Immunodeficiency is also associated with recurrences.
Herpes zoster oticus (Ramsay Hunt syndrome) is a syndrome of acute peripheral facial palsy associated with otalgia and varicella-like cutaneous lesions. It accounts for approximately 10–15% of acute facial palsy cases. The lesions may involve the external ear, particularly the meatal and preauricular skin, the skin of the ear canal, or the soft palate. These findings establish the diagnosis (Figure 70–2). Hearing loss, dysacusis, and vertigo reflect extension of the infection to involve the eighth cranial nerve. Involvement often extends to other cranial nerves (V, IX, and X) and cervical branches (2, 3, and 4) that have anastomotic communications with the facial nerve. Herpes zoster oticus is therefore differentiated from Bell’s palsy by the characteristic cutaneous changes and a higher incidence of cochleosaccular dysfunction.
Figure 70–2.


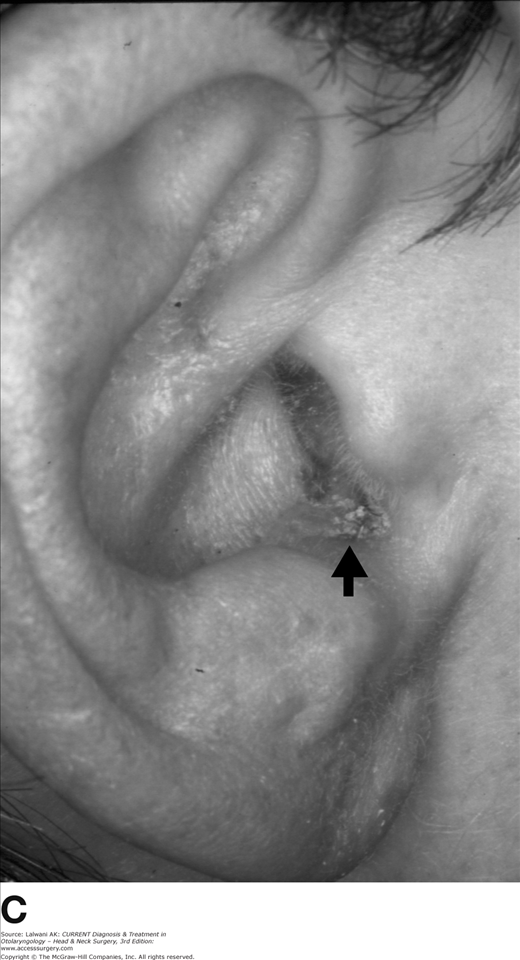
(A) Prototypic case of herpes zoster oticus. This 53-year-old woman experienced the onset of a right-sided facial paralysis with marked right-sided otalgia and throat pain. She presented 3 days after the onset of her symptoms and demonstrated minimal facial motor activity on evoked electromyography. Treatment consisted of oral steroid dosing at pharmacological doses for 10 days, followed by a 2-week taper, and acyclovir given intravenously for 1 week. (B) Full recovery of facial motor function 4 months after onset. (C) Skin lesion of the right external meatus in the same patient with oticus in the crusting phase at the time of presentation.
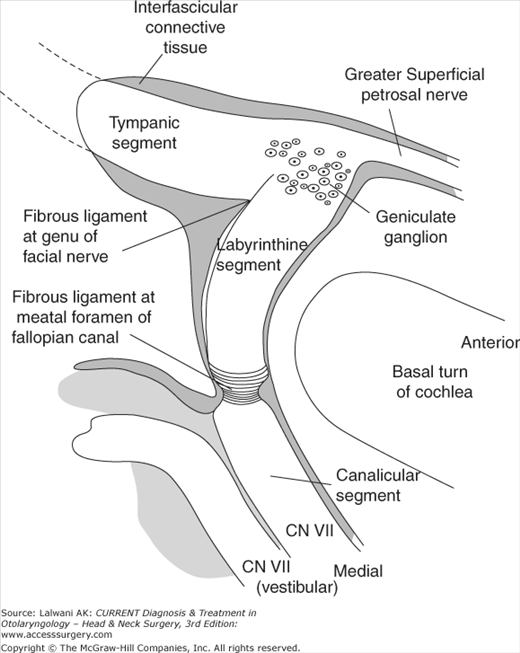
Studies of the intratemporal facial nerve suggest that Bell’s palsy and herpes zoster oticus most commonly result from the impaired facial nerve conduction within the temporal bone. The facial nerve is admitted to the temporal bone via the meatal foramen to form the labyrinthine segment of the intratemporal facial nerve. The meatal foramen in labyrinthine section of the Fallopian canal is thought to be site of constriction in Bell’s Palsy based on several lines of evidence: (1) In the labyrinthine segment, the nerve occupies more than 80% of the cross-sectional area of the canal, in contrast to occupying less than 75% in the remainder (Figure 70–3); (2) The diameter of the meatal foramen (Figure 70–3A) is substantially narrower than more peripheral segments of the facial canal with a circumferential band of periosteum that virtually seals the entry site and constricts the nerve at the this site (Figure 70–4); and (3) The facial nerve is without substantial epineurium in the meatal foramen and is instead encased by this periosteum. Thus, the meatal foramen appears to constitute a pressure transition zone or “physiological bottleneck” in the presence of neural edema. The ratio of the cross-sectional areas of the nerve to the meatal foramen is significantly smaller in pediatric temporal bones compared with those of adults. This observation may explain the low incidence of Bell’s palsy in pediatric populations.

In patients with near-total degeneration undergoing facial nerve decompression for Bell paralysis, electrical stimulation demonstrated a transition in responsiveness in the (decompressed) region of the meatal foramen. Sequential stimulation in a distal-to-proximal direction from the second genu to the meatal foramen consistently revealed substantially diminished responses proximal to the meatal foramen. These observations strongly implicate the meatal foramen as the primary pathophysiological site in Bell’s palsy.
Intraneural inflammatory changes, consistent with a viral infection, have been identified in the temporal bones of a Bell’s palsy patient who died 13 days after onset. Substantial leukocytic infiltration and demyelinization of the somatic portion of the facial nerve were evident, most prominently in the proximal, intratemporal segment of the nerve. Although small vessel congestion was present, there was no evidence of arterial thrombosis. Other studies have demonstrated that intraneural vascular congestion and hemorrhage in the labyrinthine segment of the nerve were most prominent.
Most postmortem studies from patients with Bell’s palsy demonstrate that diffuse involvement of the facial nerve in its intratemporal course was typical. Evidence of an inflammatory neuritis suggesting a viral etiology is frequently evident, though not uniformly observed.
The likelihood of the meatal foramen as the critical site for nerve injury in herpes zoster oticus is supported by neuropathological findings demonstrating a sharp demarcation between the degenerated nerve distal to and normal nerve proximal to the meatal foramen.
The several postulated mechanisms of nerve injury underlying Bell’s palsy are not necessarily exclusive of one another. Several pathological events may be sequential and synergistic in manifesting a clinical facial palsy, and the disease may represent a spectrum of entities with varied pathogeneses. Although inflammation and ischemia likely dominate early processes in Bell’s palsy, neural blockade and degeneration as well as subsequent fibroblastic response likely manifest later in the sequence. Given the confinement of the nerve trunk within the meatal foramen, it is likely that compression at this site is a critical if not determinative event in the genesis of Bell’s palsy and is triggered by one or a combination of the above etiologies. Histopathological findings suggest that the facial palsy component of herpes zoster oticus is manifest by a similar process of entrapment, with typically a higher risk of irreversible degeneration of nerve fibers.
There is a significant resemblance between Bell’s palsy and other neuropathies known to be of viral origin. Poliomyelitis, mumps, Epstein-Barr virus, and rubella infections can manifest a neuritic component characterized by progressive neural dysfunction, often with subtotal regeneration as is often observed with Bell’s palsy and herpes zoster oticus. There are multiple lines of evidence for a viral etiology in Bell’s palsy based on clinical observations and experimental models reported over the last 20 years. Rabbit facial nerve trunks inoculated with herpes simplex virus demonstrate facial motor dysfunction that progressed to paralysis within the first week after inoculation. Herpes simplex virus Type I has been identified in isolates of the herpes simplex virus from the nasopharynx of patients during the acute phase of Bell’s palsy. A higher prevalence of herpes simplex viral antibodies has been identified in patients with Bell’s palsy as compared with gender- and age-matched controls. Herpes simplex virus has a well-known predilection for sensory neurons as well as a predilection to exist in a latent phase in sensory cell bodies of the ganglion. The facial nerve contains sensory neurons with cell bodies located in the geniculate ganglion, and it is believed that infection of the facial nerve, such as a geniculate ganglionitis, underlies Bell’s palsy.
The presence of the herpes simplex virus has been detected in epineurial biopsies from a patient undergoing facial nerve decompression for Bell paralysis. While this finding further links Bell’s palsy with a herpes simplex viral infection, ultrastructural studies of autopsy material from asymptomatic patients has demonstrated herpes simplex viral particles in sensory ganglia of regional cranial nerves, most notably the trigeminal ganglion. Thus, evidence of viral presence in the facial nerve, although highly suggestive, does not prove conclusively that the herpes simplex virus bears a causal role in Bell’s palsy.
The role of the varicella-zoster virus as etiologic in herpes zoster oticus is supported strongly by the characteristic varicelliform rash. This rash assumes a dermatologic distribution in a pattern that mimics the distribution of afferent fibers of the facial nerve. Serological confirmation of varicella-zoster infection is often, but not always, possible. Histological studies indicate facial dysfunction with herpes zoster oticus to be the result of an entrapment neuropathy, with more pronounced nerve fiber degeneration than that typically found in histopathological studies of Bell’s palsy.
The herpes simplex and varicella-zoster agents are both DNA viruses of the herpes virus group and differ subtly in their ultrastructural features. Although differences in biological behavior suggest that neuritides resulting from these viruses should manifest clinically distinguishable differences in their clinical presentation, infections from herpes simplex and varicella-zoster viruses may mimic one another. Furthermore, herpes simplex, mumps, and cytomegalovirus infections may produce a clinical picture resembling herpes zoster oticus; varicella-zoster neuritis may occur in the absence of a rash (ie, zoster sine eruptione).
One time-honored concept of the genesis of Bell’s palsy holds that impaired neural conduction follows small vessel ischemia. The facial nerve derives its blood supply from an extrinsic, circumneural vessel network derived from three principle sources: (1) the labyrinthine artery (proximally), (2) the middle meningeal artery (centrally), and (3) the stylomastoid artery (distally). The circumneural system connects to an intrinsic vascular supply of small vessel tributaries within the perineurial compartment. The pathological process is thought to involve the intrinsic system of vessels. Pressure elevations within the intraneural compartments produce venous stasis, stagnation of capillary flow, and a cycle of additional edema and an elevation in intraneural pressure. Circulatory sludging and, ultimately, tissue damage through acidosis and anoxia ensue. The mechanism by which the cascade of primary ischemia is initiated remains unclear.
Several investigations have implicated immunologic injury as a potential cofactor in Bell’s palsy. Neuropathological findings of segmental demyelinization accompanied by lymphocytic infiltration of the perineurium support this etiology. Autoimmune mechanisms of nerve injury have also been suggested; evidence for humoral and cellular autoimmunity has been reported. Immunoassay methods have been used to detect acute-phase antibodies within the chorda tympani nerve from three of seven patients with Bell’s palsy. Immune complexes found in the chorda tympani nerve fibers were characteristic of viral–antibody (Type III) immunologic reaction, suggesting an immune injury triggered by the presence of viral antigens.
A wide spectrum of health care providers manage cases of acute facial palsy; an assessment of the true incidence of Bell’s palsy is therefore complicated by this wide distribution of specialists. Nonetheless, this disorder is recognized as one of the most common neuropathies and appears to be universal in its occurrence. The incidence is approximately 15–40 per 100,000 individuals in the general population.
Age and gender influence the likelihood of contracting Bell’s palsy. Bell’s palsy is infrequent in patients under the age of 10 years, but thereafter increases in incidence with age. Females in their teens and twenties carry a predilection for the disorder. Among middle-aged adults, there is a nearly equal distribution by gender with a slight male predominance in older age groups. Epidemiological surveys indicate a seasonal variation in incidence in some geographic regions.
The risk posed by diabetes mellitus in developing Bell’s palsy remains undetermined, although most studies suggest a heightened susceptibility. Several authors have demonstrated a correlation between pregnancy and acute facial palsy, particularly during the third trimester and with the presence of preeclampsia.
Immunodeficiency may also entail a heightened risk for acute facial palsy. Cranial neuropathies, including facial palsy, are observed with human immunodeficiency virus (HIV) infection, often in association with a symmetrical polyneuropathy. Facial dysfunction in this setting may also reflect either susceptibility to other infectious agents or the development of lymphoma. Facial palsy in association with HIV may occur in a clinical course characteristic of Bell’s palsy or herpes zoster oticus. Neuropathies may appear at any stage of HIV infection: early after initial infection, as part of the chronic illness characterized by the AIDS, or with AIDS-related meningitis. Case series suggest that facial palsy in the setting of HIV infection not associated with neoplasm demonstrates patterns of spontaneous recovery that are not unlike those of the general population.
Facial palsy associated with the conditions noted above is not necessarily diagnostic of Bell’s palsy. Patients should be evaluated as completely as those who do not carry these risk factors, with the notable caveat of considering the risk and benefit of radiological studies in pregnancy.
The diagnosis of Bell’s palsy is one of exclusion. Facial motor disturbance should be characterized as Bell’s palsy only after the exclusion of traumatic, neoplastic, infectious, metabolic, and congenital etiologies. Strict attention to the evaluation, particularly the history and otoscopic and neurological findings, often differentiates an acute facial palsy of another origin from a true case of Bell’s palsy.
On the clinical examination, the severity of the palsy should be recorded by one of the standard facial nerve grading schemes. In particular, one should assess for the ability to close the eyelid, as this will have the greatest functional significance. The presence of vesicles within the auricle or external auditory canal may reveal the diagnosis of herpes zoster oticus. Pain or numbness affecting the ear, mid-face, and tongue, as well as taste disturbances, are common.
Blood and cerebrospinal fluid studies will only rarely differentiate a facial palsy and are largely unwarranted for most cases of Bell’s palsy. For atypical cases though, one should consider Lyme titers and a search for a paraneoplastic syndrome.
Routine radiological evaluation is generally not recommended for most cases of acute facial palsy, particularly when the clinical course matches that of Bell’s palsy or herpes zoster oticus. However, should the patient’s recovery be incomplete over 3-months time, the palsy becomes recurrent, or associated cranial nerve deficits develop, then scans are warranted. Magnetic resonance imaging scanning with dye enhancement should include the brain, the skull base, and the temporal bone to rule out a lesion along the entire course of the facial nerve. High-resolution computed tomography (CT) scanning may be useful to define the bony detail in the course of the facial nerve within the fallopian (facial) canal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


