(1)
Narayana Hridayalaya Multispeciality, Bangalore, India
Surgical Anatomy and Pathology
The neck node remains the most important prognostic factor for head and neck cancer, and its management is of paramount importance. The neck nodes can be classified into five levels (Fig. 5.1). Level I is subdivided into IA (submental) and IB (submandibular). Levels II, III, and IV are deep cervical nodes along with internal jugular vein. Level II is further divided into IIA (anterior to spinal accessory) and IIB (posterior to spinal accessory). Levels III and IV are lower cervical nodes. Level V is situated posterior to the sternocleidomastoid muscle. It is further subdivided into VA (anterior to spinal accessory) and VB (posterior to spinal accessory).
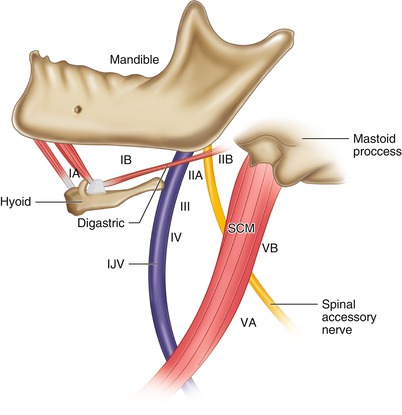
Fig. 5.1
Levels of neck
Figure 5.2 demonstrates the algorithm for neck management for head–neck squamous cell carcinoma. The treatment approach has constantly been changing over the past few years and becoming more and more selective. This shift from radical neck dissection (RND) to modified neck dissection (MND) and to selective neck dissection (SND) has helped in improving the morbidity profile after the surgical procedure. This selective approach is based on better understanding of the spread of disease to the neck. Salvage neck dissection still remains a challenge and can lead to major postoperative complications like bleeding and wound breakdown. The concept of supra-selective neck dissection is becoming popular in salvage setting where selective removal of the involved lymph node (involved level with one level above and below) is considered adequate. The oral cavity generally drains into level I to III while tongue and floor of mouth (FOM) drains into level IV as well. The primary nodal basin for the larynx and pharynx is level II to IV. The level V nodes are addressed only in case of involvement of level IV or V.
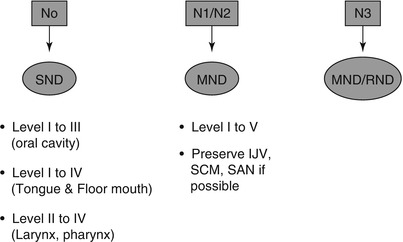
Fig. 5.2
Treatment algorithm
Surgical Concepts
The treatment approach is becoming more selective with better understanding of nodal drainage patterns.
SND is the most commonly performed operation for N0 neck. It is also becoming acceptable for multiple node-positive patients (N+) where lower level nodes are not involved. These patients must receive adjuvant radiotherapy.
MND is commonly performed for N+ neck where nodes involve level III to V. The spinal accessory nerve, internal jugular vein, and sternocleidomastoid (SCM) muscle are preserved as far as possible.
RND is generally reserved for N3 node involving surrounding structures.
The concept is to do minimal dissection as far as possible to salvage neck to avoid undue complications.
Selective and Modified Neck Dissection
This procedure demonstrates SND and MND removing level I to IV lymph nodes.



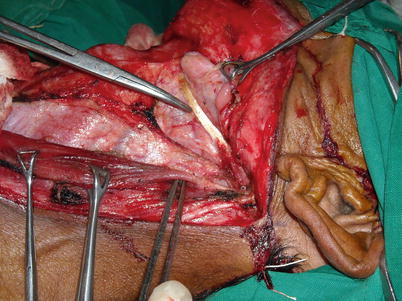
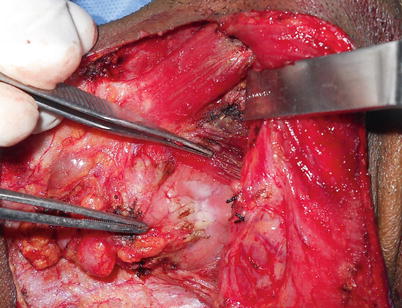
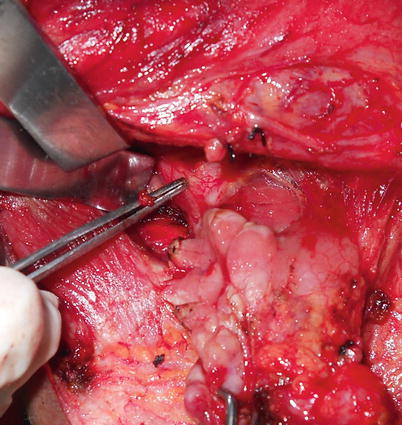
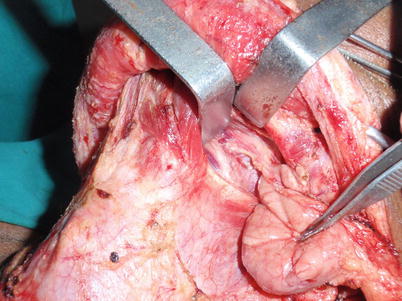

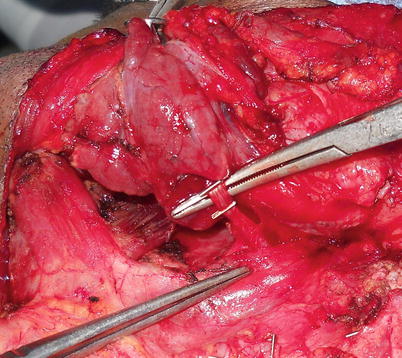

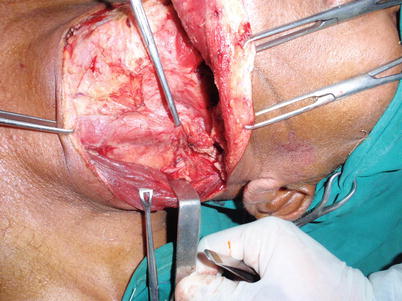
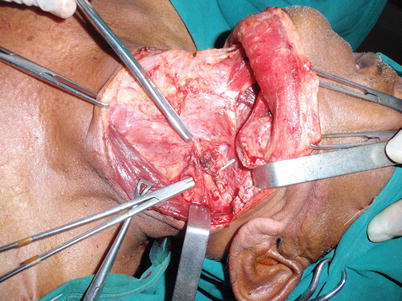
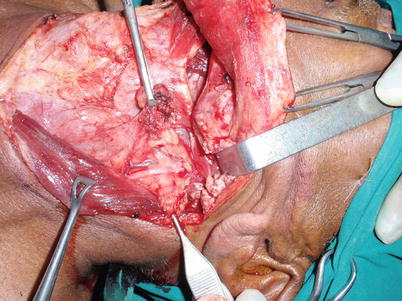
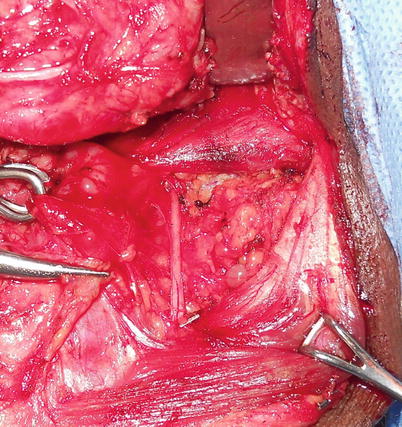
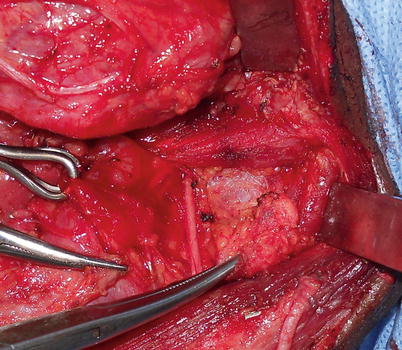
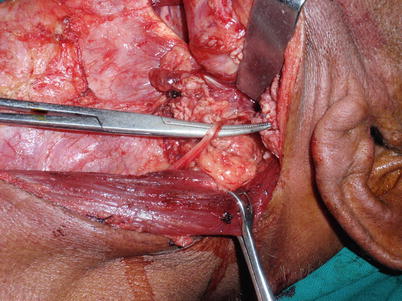




Fig. 5.3
Upper transverse cervical incision. The vertical incision in submental area can be restricted based upon surgeons comfort
Fig. 5.4
Upper flap is raised in subplatysmal plane. In case of large matted node, platysma can be left attached to node and flap can be raised in subcutaneous plane
Fig. 5.5
Identification of marginal mandibular nerve. This nerve runs in deep fascia and can be exposed by opening the deep fascia near angle of mandible. For malignant case, one can raise flap in sub-platysmal plane and gradually dissect marginal nerve from deep fascia. The facial nodes are removed with specimen. For benign case, the flap can be raised deep to deep facia while removing submandinular gland completly without exposing the nerve and thereby preserving it. The facial nodes are left behind with this approach which is inappropriate for oral cancers
Fig. 5.6
Identification of facial vessels below the nerve. They are ligated and then lifted up to preserve marginal nerve
Fig. 5.7
The photograph shows clearance of level IA both belly of digastric muscle is exposed fully to remove all tissue from mandible to hyoid
Fig. 5.8
The next step is to expose the posterior belly of the digastric tendon. This is a very important step as this clearly defines the anatomy of the neck. The facial vein is the only structure that runs above it and can be ligated. All other important vascular structures run deep to this muscle
Fig. 5.9
Exposure of mylohyoid muscle while removing submandibular gland. There are small veins in this area that need proper hemostasis
Fig. 5.10
Exposing the lingual nerve that is tethered to deep portion of gland. This band contains small vessels and release of this band frees the lingual nerve
Fig. 5.11
Both the hypoglossal and lingual nerves are seen in this photograph. The hypoglossal nerve is in the floor of the gland and runs deep to fascia
Fig. 5.12
Isolation of facial artery that enters in the gland just above the posterior belly of digastric near angle of mandible
Fig. 5.13
The facial artery is ligated and gland along with facial node is removed
Fig. 5.14
The dissection starts to clear level II nodes. The first step is to identify spinal accessory nerve. The SCM muscle is retracted backward. Key is to stay right on muscle taking all fascia anteriorly. There is a small blood vessel just above the nerve, and this can serve as a guide to the nerve
Fig. 5.15
The nerve is exposed. It is advisable to use bipolar cautery in this region
Fig. 5.16
Lymph nodes and surroundings tissues are dissected out at level 2A and 2B
Fig. 5.17
The nerve is exposed in its entire length
Fig. 5.18
The anatomy of level II nodes. The nerve divides it into level A and B. Clearance of level IIB is important and should be carried out by exposing digastric and SCM muscle till mastoid process
Fig. 5.19
The level IIB clearance. The posterior occipital artery can be encountered here sometimes and can be ligated
Fig. 5.20
The IIB nodes are mobilized under the nerve to IIA compartment. This isolates and secures the nerve. It is important to minimize handling of the nerve during this entire procedure. Skin incision till mastoid process significantly enhances the exposure and aids in this process
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
