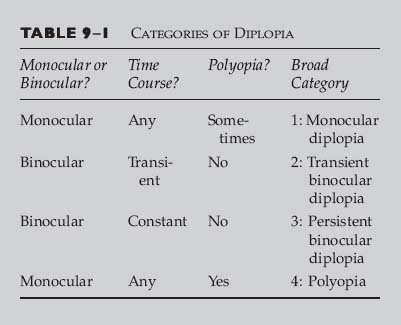
Chapter 9 In this chapter, we divide diplopia into four broad categories: monocular, transient binocular, persistent binocular, and polyopia (more than two images). The clinician should establish from the history whether the diplopia is monocular (present with only one eye open) or binocular (resolves with occlusion of either eye). If the diplopia is monocular, then the problem is almost always intraocular. If the diplopia is binocular (suggesting ocular misalignment), then further history should elucidate if the double vision is transient or constant. The history and exam should focus on characteristics of the diplopia that will aid in the localization of the lesion. Additional information includes whether the deviation is horizontal or vertical and if the diplopia is worsened in a particular gaze or head position. Before using Table 9–1, you should establish the following: • Monocular or binocular: If there is diplopia present with only one eye open, then it is monocular. If the diplopia disappears with occlusion of either eye, then it is binocular. • Time course: Is the diplopia transient or constant? • Polyopia: Are there more than two images at any time? Table 9–2 is used for monocular diplopia. Before using this table, you should establish that the diplopia is strictly monocular. This can usually be based on the history alone. Unilateral monocular diplopia is present despite covering the fellow eye and then disappears when the involved eye is occluded. Monocular diplopia, however, may occur in both eyes (bilateral but still monocular diplopia) and remains present in the involved eye with covering either eye.
DIPLOPIA AND POLYOPIA
BROAD CATEGORY 1: MONOCULAR DIPLOPIA
Refractive error (especially astigmatism, aniseikonia) Poorly fitting contact lens Corneal abnormalities Keratoconus Tear film disorders including dry eye Refractive surgery Corneal transplant Lid abnormalities (e.g., chalazion, lid malposition) Iris abnormalities (e.g., iridotomy/iridectomy, miosis) Lens abnormalities Cataract Subluxation or dislocation Intraocular lens (e.g., positioning holes, decentered lens) Retinal abnormalities (e.g., epiretinal membrane, metamorphopsia) |
Modified from Lee AG, Brazis PW. Clinical Pathways in Neuroophthalmology: An Evidence-Based Approach. New York: Thieme, 1998, with permission.
QUESTIONS TO ASK AND POINTS TO KEEP IN MIND
• Are both images clear?
 Second image is typically not as clear or is blurry in monocular diplopia.
Second image is typically not as clear or is blurry in monocular diplopia.
 Partially superimposed “ghost image” or a “halo” may be present on the first image.
Partially superimposed “ghost image” or a “halo” may be present on the first image.
 In distinction, binocular diplopia is usually described as two separate and distinct objects.
In distinction, binocular diplopia is usually described as two separate and distinct objects.
• Does pinhole reduce the symptoms? (Pinhole improves monocular diplopia.)
• Does it respond to refraction, artificial tear trial, or contact lens trial?
• Is there media opacity (e.g., dry eyes, corneal disease, and cataract)?
• Isolated monocular diplopia does not generally require any further neuro-ophthalmologic evaluation unless it fails to improve with pinhole, suggesting a cerebral or macular cause.
BROAD CATEGORY 2: TRANSIENT BINOCULAR DIPLOPIA
QUESTIONS TO ASK AND POINTS TO KEEP IN MIND
• May be noted only in certain fields of gaze (e.g., only on looking down)
• May fluctuate during the day (e.g., thyroid ophthalmopathy symptoms worse in the morning and myasthenia in the evening)
• Patients may be asymptomatic at the time of examination, and ocular misalignment may be subtle or absent
• Table 9–3 lists the causes of transient diplopia.
Transient ischemia (including migraine) Decompensation of preexisting phoria Retinal hemifield slide phenomenon Myasthenia gravis Thyroid ophthalmopathy Neuromyotonia Intermittent skew deviation Superior oblique myokymia Multiple sclerosis (days to weeks duration) |
Modified from Lee AG, Brazis PW. Clinical Pathways in Neuroophthalmology: An Evidence-Based Approach. New York: Thieme, 1998, with permission.
SUPERIOR OBLIQUE MYOKYMIA
Classic Presentation
• Disorder of unknown etiology
• Symptomatic oscillopsia, vertical or torsional diplopia, or both
• Bursts of monocular rotary oscillations
• Small-amplitude and high-frequency movements
• Low-frequency and large-amplitude intorsional movements
• Episodes usually last only a few seconds at a time
• Episodes best seen using slit-lamp exam or the direct ophthalmoscope
• Carbamazepine or propranolol may improve symptoms.
• Surgery (superior oblique tenectomy and inferior oblique myectomy) may be curative if patients fail or are intolerant to medication.
• Usually benign, rarely associated with intracranial lesion
Red Flags
 Bilateral symptoms or signs
Bilateral symptoms or signs
 Associated neurologic deficit
Associated neurologic deficit
PAROXYSMAL SUPERIOR RECTUS AND LEVATOR PALPEBRAE SPASM
Classic Presentation
• Rare (one case of multiple sclerosis)
• Paroxysms of vertical diplopia and lid retraction lasting 3 to 4 seconds
• Magnetic resonance imaging (MRI) reveals lesion of midbrain third nerve fascicle
• Carbamazepine (Tegretol) may resolve symptoms.
OCULAR NEUROMYOTONIA
Classic Presentation
• Rare disorder in which there is tonic overactivity of an extraocular muscle after sustained action
• Episodic diplopia that occurs spontaneously
• Extraocular muscles innervated by the third nerve most commonly involved
• Prior radiation therapy to the sellar or parasellar region for tumors common
• Carbamazepine may be helpful
DECOMPENSATION OF A LONG-STANDING PHORIA
Classic Presentation
• Intermittent tropia (ocular deviation) and episodic diplopia
• History of childhood strabismus or patching
• Long-standing head tilt or turn (review old photographs)
• Large fusional amplitudes
• Full ductions and versions usually
• Comitant deviation typically
Red Flags
 Incomitant (i.e., deviation varies with direction of gaze)
Incomitant (i.e., deviation varies with direction of gaze)
 Abnormal ductions
Abnormal ductions
OPHTHALMOPLEGIC MIGRAINE
Classic Presentation
• Starts in the first decade of life
• Usually affects the oculomotor nerve (rarely trochlear)
• Episodic ocular motor neuropathy
• History of typical migraine headache
Red Flags
 Diagnosis of exclusion
Diagnosis of exclusion
 First attack occurs after childhood
First attack occurs after childhood
 No typical migraine history
No typical migraine history
 Persistent deficit
Persistent deficit
MYASTHENIA GRAVIS
Classic Presentation (See Chapter 34)
• May mimic any pattern of ophthalmoplegia
• Painless
• Worsens with fatigue and improves with rest
• Variable ocular measurements
• Ptosis
• Tensilon or Prostigmin test positive
Red Flags
 Involvement of the pupil
Involvement of the pupil
 Significant eye pain or headaches
Significant eye pain or headaches
 Proptosis
Proptosis
 Visual loss
Visual loss
 Sensory involvement
Sensory involvement
SKEW DEVIATION
Classic Presentation
• Ocular misalignment resulting from supranuclear pathway disruption
• May be constant or transient
• Comitant or incomitant vertical misalignment
• Ductions are normal
• Imbalance of graviceptive (otolith) brainstem pathways
• Associated with other brainstem (mesencephalon to medulla) or cerebellum signs and symptoms
Red Flags
 “Isolated” skew (skew usually occurs with other signs; an isolated skew is often a fourth nerve palsy)
“Isolated” skew (skew usually occurs with other signs; an isolated skew is often a fourth nerve palsy)
 Abnormal ductions
Abnormal ductions
RETINAL HEMIFIELD SLIDE PHENOMENON
Classic Presentation
• Complete or nearly complete bitemporal hemianopsia
• Disruption of fusion and decompensation of previous phoria
• Intermittent diplopia and difficulty with near vision
• No ocular motor palsy
BROAD CATEGORY 3: PERSISTENT BINOCULAR DIPLOPIA
QUESTIONS TO ASK AND POINTS TO KEEP IN MIND
• Binocular diplopia is usually associated with ocular misalignment. Identification of specific clinical signs and symptoms may allow identification of specific etiologies for the diplopia.
• Vertical or horizontal?
• Worse in right or left gaze?
• Worse or better with head position?
• Rare patients may notice physiologic diplopia (doubling of the distant image upon convergence on a near target).
RESTRICTIVE OPHTHALMOPLEGIA DUE TO ORBITAL DISEASE
Classic Presentation
• Orbital signs, such as proptosis, chemosis, and injection
• Forced ductions reveal restrictive component
• Etiologies of restriction
• Orbital wall fractures
• Orbital tumors
• Orbital inflammatory disease
• Muscle trauma or surgery with scarring
• Thyroid disease
THYROID EYE DISEASE
Classic Presentation (See Chapter 38)
• Systemic thyroid disease (hyperthyroidism)
• Lid retraction
• Lid lag
• Proptosis
• Chemosis and injection
• May develop exposure keratopathy
• Inferior scleral show
• Typically involves, in order of frequency, the inferior, medial, superior, and then lateral recti
• May develop compressive optic neuropathy
Red Flags
 Exotropia (usually esotropia due to medial rectus restriction)
Exotropia (usually esotropia due to medial rectus restriction)
 Ptosis (usually lid retraction)
Ptosis (usually lid retraction)
 Systemically euthyroid (although may present with eye disease without systemic thyroid disease)
Systemically euthyroid (although may present with eye disease without systemic thyroid disease)
 Strictly unilateral findings
Strictly unilateral findings
 Proptosis asymmetry greater than 4 to 5 mm
Proptosis asymmetry greater than 4 to 5 mm
 Severe pain
Severe pain
Evaluation
• Check thyroid status
• Exclude compressive optic neuropathy and exposure keratopathy
• Consider orbital ultrasound or computed tomography
SUPRANUCLEAR OPHTHALMOPLEGIA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


