Differential Diagnosis of Age-Related Macular Degeneration
Gabriela Papa-Oliva
Monica Rodriguez-Fontal
D. Virgil Alfaro III
INTRODUCTION
The diagnosis of age-related macular degeneration (AMD) can be challenging, particularly when the patient is in the age group commonly affected by AMD. Nonneovascular AMD is the most common type of AMD, observed in 90% of cases. Nonneovascular AMD demonstrates chorioretinal atrophy that may be difficult to differentiate from retina changes associated with other pathologies. The other major form of AMD, neovascular AMD, occurs with loss of visual acuity secondary to choroidal neovascularization (CNV). An extensive number of conditions can predispose the macula to develop CNV (1).
This chapter examines the differential diagnosis of age-related macular degeneration.
NONNEOVASCULAR AGE-RELATED MACULAR DEGENERATION
It is well known that aging produces changes at the level of the outer retina, retinal pigment epithelium (RPE), Bruch’s membrane, and choriocapillaris (2). These changes are microscopic, are sometimes not visible on clinical examination, and should be distinguished from clinically visible changes found in patients with nonneovascular AMD. Among these changes are drusen and alterations of the RPE.
Drusen are histologically defined as abnormal thickening of the inner face of the Bruch’s membrane and clinically defined as yellow or yellowish-white deposits at the level of the retina. They are classified by size (small less than 64 µm, 64-124 µm intermediate, and large greater than 125 µm), by type (soft and hard), by distribution (greater clinical significance if located in the macula inner circular area of 3,000 µm in diameter), and by the extent of fundus involvement (3,4).
DIFFERENTIAL DIAGNOSIS OF NONNEOVASCULAR AGE-RELATED MACULAR DEGENERATION
The most common diseases that can present changes similar to nonneovascular AMD are central serous chorioretinopathy (CSC), pattern dystrophy, dominant drusen, chloroquine toxicity, central areolar choroidal dystrophy, and cuticular drusen (Table 9.1).
Cuticular Drusen
Cuticular drusen or basal laminar drusen (BLD) were described by Gass in 1977 (5). Patients with BLD have
numerous, small, uniformly sized, round, slightly raised, yellow, subretinal lesions on ocular fundus examination. These lesions are grouped into small clusters and usually span the macula between the arcades (Fig. 9.1A). The drusen are hyperfluorescent during fluorescein angiography and fade in later-phase frames (Fig. 9.1B). The lesions may develop a yellowish vitelliform material anterior to RPE. As it progresses, it clears and develops a marked or minimal geographic atrophy. The vitelliform material can block choroidal fluorescence in early stages of fluorescein angiography and stain in the later phase. The staining in later frames may mimic the appearance of type 1 occult CNV.
numerous, small, uniformly sized, round, slightly raised, yellow, subretinal lesions on ocular fundus examination. These lesions are grouped into small clusters and usually span the macula between the arcades (Fig. 9.1A). The drusen are hyperfluorescent during fluorescein angiography and fade in later-phase frames (Fig. 9.1B). The lesions may develop a yellowish vitelliform material anterior to RPE. As it progresses, it clears and develops a marked or minimal geographic atrophy. The vitelliform material can block choroidal fluorescence in early stages of fluorescein angiography and stain in the later phase. The staining in later frames may mimic the appearance of type 1 occult CNV.
Table 9.1 DIFFERENTIAL DIAGNOSIS OF NONNEOVASCULAR AMD | |
|---|---|
|
Initially, the term BLD was used to distinguish these drusen from drusen associated with AMD (6). Subsequent histologic analysis demonstrated that both types of drusen were indistinguishable. Both the BLD and the drusen associated with AMD are located between the basement membrane of the RPE and the inner collagenous layer of the Bruch’s membrane (7). Furthermore, both types of drusen were shown to be histologically indistinct using light and electron microscopy. This entity should not be confused with the histopathologic terms “basal lamellar deposits” or “basal linear deposits.” Although the visual prognosis for cuticular drusen is better than the visual prognosis for patients with AMD, the possibility of CNV exists in both diseases and is associated with worse visual acuity outcomes (8).
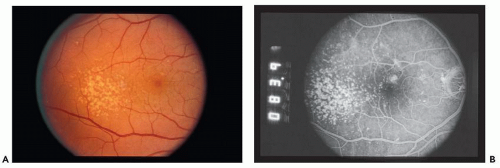 Figure 9.1 ▪ A. Basal laminar drusen. B. Fluorescein angiography showing starry-night pattern. |
Central Serous Chorioretinopathy
This idiopathic disease is most common in Caucasian, Hispanic, and Asian patients between the second and fifth decade of their lives. More often, it is diagnosed in patients with type A personality, high stress levels, or use of corticosteroids (inhaled, topical, or systemic). CSC clinically presents as a sensory retinal detachment that may also be associated with RPE serous retinal detachment. The diagnostic challenge is significant for older age groups with changes in the RPE due to multifocal serous detachments (9,10). In some cases, the formation of “gutter–like” distribution of RPE atrophy in the absence of drusen may help make the diagnosis (Fig. 9.2).
Patients with chronic or recurrent CSC may have decreased visual acuity as a result of RPE dysfunction, subretinal precipitates, and subretinal CNV. The presence of CNV and subretinal fluid in a patient with CSC may be difficult to distinguish from neovascular AMD. Diagnostic clues include absence of drusen, absence of hemorrhage, patches of RPE atrophy in a gutter–like distribution, and the presence of multiple pigmented epithelium detachments (Fig. 9.3).
Pattern Dystrophy
The term “pattern dystrophy” represents a group of related conditions inherited in an autosomal dominant fashion. These macular dystrophies are relatively benign disorders. They are characterized by an abnormality at the level of RPE with hyperpigmentation and variably shaped yellow or gray deposits (Fig. 9.4A and B). The patients are asymptomatic and usually have normal vision. The classic appearance of pattern dystrophy demonstrates the pigmented lesions in the shape of a butterfly. The lesions are clearly seen in the fluorescein angiography. Typically, the lesions are hypofluorescent with a surrounding hyperfluorescent rim (Fig. 9.4C and D). This configuration helps to differentiate them from soft drusen of AMD (11,12,13). Other pattern dystrophies that we need to have
in mind are reticular dystrophy of Sjögren and macroreticular dystrophy.
in mind are reticular dystrophy of Sjögren and macroreticular dystrophy.
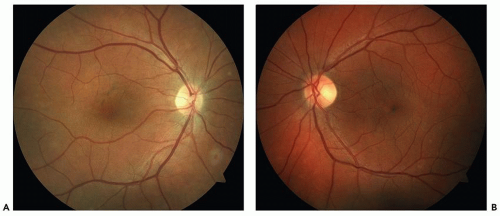 Figure 9.2 ▪ Central serous chorioretinopathy. A. Fundus photograph, right eye, showing RPE changes from CSC. B. Fundus photograph, left eye, showing RPE changes from CSC. |
Chloroquine Toxicity
Chloroquine has high affinity with melanin and is deposited in the RPE. The toxic damage is initiated by the degeneration of the photoreceptors, with subsequent degeneration of other retinal cells and the RPE. RPE mottling and non-geographic atrophy may be seen in the macular area in patients with toxic changes. The absence of drusen and a positive history of drug ingestion are essential to make the diagnosis (14) (Fig. 9.5A and B).
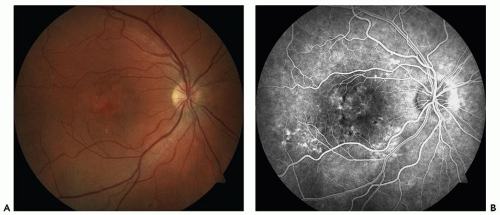 Figure 9.3 ▪ Central serous chorioretinopathy. A. Fundus photograph, right eye, showing RPE changes from multifocal serous detachments. B. Fluorescein angiography showing leakage. |
Dominant Drusen
This entity is inherited in an autosomal dominant fashion, affecting individuals between the second and third decade of their lives, and it is best observed on fluorescein angiography. Drusen may become confluent after the fourth decade. Initially, patients are asymptomatic. Eventually, central vision loss correlates with macular involvement,
and it can be distinguished from AMD only on the basis of family history (15) (Fig. 9.6).
and it can be distinguished from AMD only on the basis of family history (15) (Fig. 9.6).
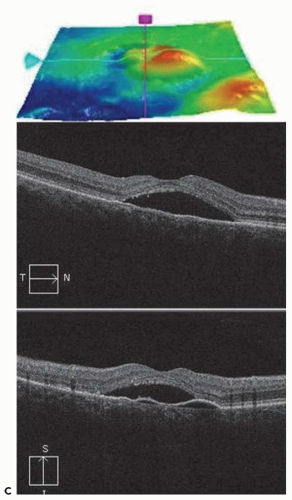 Figure 9.3 ▪ (Continued) C. OCT showing multifocal serous pigmented epithelium detachments and subretinal fluid. |
Central Areolar Choroidal Atrophy
The mean age at onset of visual loss is the fourth decade of life, with subsequent gradual deterioration in visual acuity. At early stages, the disease presents no symptoms associated with symmetric fine mottled areolar depigmentation of the fovea. In later stages, the depigmented area develops a sharply demarcated geographic atrophy that involves photoreceptors, RPE, and choriocapillaris (Fig. 9.7). In the elderly patient, central areolar choroidal atrophy may be confused with AMD (16).
NEOVASCULAR AGE-RELATED MACULAR DEGENERATION
The term CNV refers to ingrown fibrovascular tissue from the choroidal circulation into or underneath the retina. This fibrovascular tissue can progress to a disciform scar and cause irreversible vision loss. Any pathologic process that disturbs the RPE and choroid, leading to the disruption of the Bruch’s membrane, can be associated with CNV (17). There are different causes of CNV; some of those more frequently found are age-related macular degeneration, ocular histoplasmosis, multifocal choroiditis, myopia, and trauma.
CNV has been divided in two types: type I and type II. Type I CNV is characterized by a neovascular growth between the inner and outer aspects of the Bruch’s membrane, and it is more frequent in AMD. In type II CNV, neovascular growth occurs within the subsensory retinal space. Type II CNV is more frequent in young patients (18,19




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
