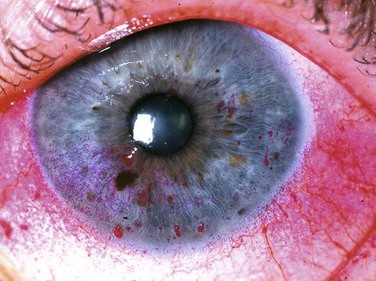
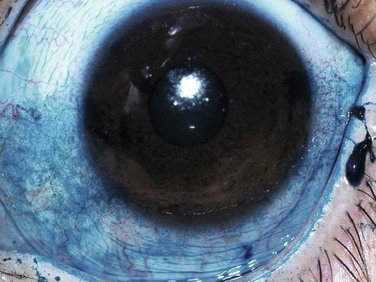
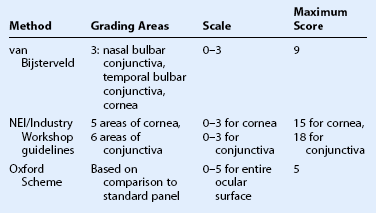
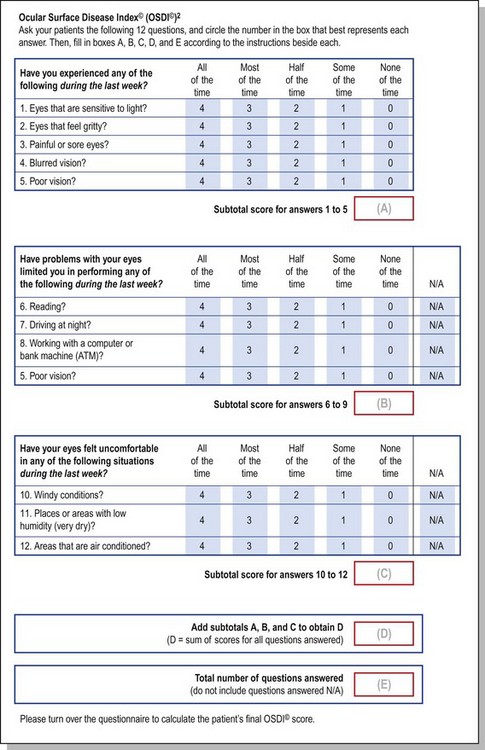
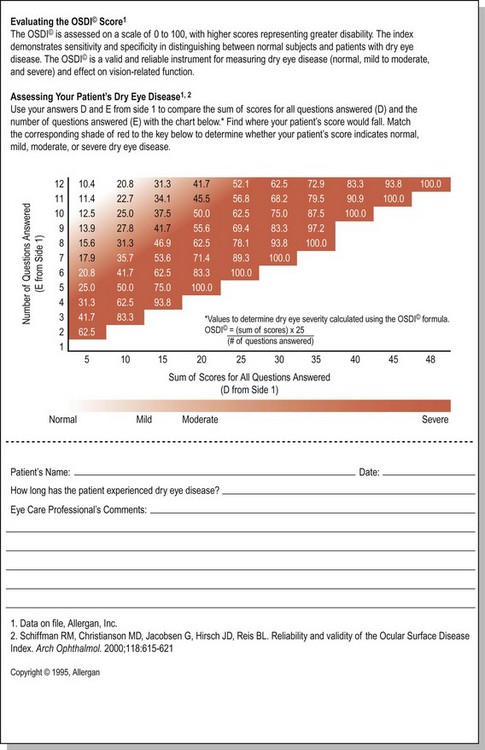
7 The slit lamp examination is a crucial part of the process when evaluating any ophthalmologic patient, and is no different for the individual with ocular surface disease. Careful, systematic examination from the outside to the inside of the eye should be performed each and every time. Care should be taken to specifically evaluate the condition of the meibomian glands (Fig. 7.1) and the entire conjunctival surface, including the palpebral areas, looking for inflammation and scarring. Once this is all performed, without anesthesia and stains, the examination can proceed to the next steps, including Schirmer testing and then ocular surface staining. The Schirmer test is a simple test that was first described in 19031 and it is still commonly performed in the office to assess aqueous tear production. There are three variations of this test, but the most popular is the Schirmer I test which measures both basal and reflex tear production. In this test, a strip of filter paper is placed on the lower eyelid margin without anesthesia, after 5 minutes, the strip is removed, and the amount of wetting is measured in millimeters (Fig. 7.2). Although this test is used frequently in the office, it has been found to lack accuracy and reproducibility: the same person’s test results taken at the same time each day for several days can fluctuate widely, and the mean Schirmer I test results for normal individuals have been reported to range from 8.1 mm to 33.1 mm.2 As such, many ophthalmologists do not even use this test anymore, but for those who do, in general, any value below 10 mm is considered abnormal. Many other ophthalmologists consider this test as a reasonable diagnostic tool only for severe dry eyes, where there is moderate reproducibility,3 with many practitioners only considering values of less than 5 mm to be significant. Fluorescein sodium is one the most frequently used methods for evaluating corneal staining, and it has been used since the end of the nineteenth century. Fluorescein penetrates poorly into the lipid layer of the corneal epithelium, and therefore, it does not stain normal cornea. Instead, the surface is stained whenever there is disruption of the cell-to-cell junctions.4 Although fluorescein is a very effective stain for the diseased cornea, it is more difficult to detect fluorescein staining of the conjunctiva because of the poor scleral contrast. However, this staining can be more readily viewed if a yellow (blue-free) filter is used. Rose bengal stain has also been used for a very long time: in this case for nearly a century. It is a derivative of fluorescein and is used to detect damage on the ocular surface, especially on the conjunctiva (Fig. 7.3). Although originally thought to stain dead or devitalized cells, rose bengal is currently believed to stain any part of the ocular surface that is not adequately protected by the tear film,4,5 specifically, in areas lacking membrane-associated mucins.6 Though an excellent diagnostic tool, rose bengal has been shown to be toxic to epithelial cells, and patients often complain about the burning and stinging upon instillation. Lissamine green is a synthetic organic acid dye that stains in a similar fashion to rose bengal, but without causing stinging and without affecting the viability of the cells. For this reason, it has gained popularity in its use. However, staining with lissamine green is dose-dependent and an inadequate volume results in weak staining that can be overlooked. A minimal dosage of 10–20 µL is recommended for accurate diagnostic ability (Fig. 7.4). There are three commonly used methods to grade ocular surface staining: the van Bijsterveld system,7 the NEI/Industry Workshop guidelines,8 and the Oxford Scheme.9 At the present time, there is no evidence that any one method is superior to another for grading the ocular surface staining patterns (Table 7.1). The tear break-up time (TBUT) is defined as the time interval between a complete blink and the first appearance of a dry spot in the tear film after fluorescein administration.10,11 It is believed that this represents an unstable tear film, whereby the mucous layer may rupture, allowing the aqueous to come in contact with exposed epithelium,12 but the exact mechanism is poorly understood. Like the Schirmer test, the TBUT test has been criticized as being unreliable and not reproducible. Many factors may lead to its non-reproducibility, including the volume of fluorescein administered, as well as the presence of preservatives, such as benzalkonium chloride, which may shorten TBUT. Despite this unreliability, it is generally agreed that a TBUT of less than 10 seconds suggests tear film instability, and less than 5 seconds suggests definite dry eye.13 The Ocular Surface Disease Index (OSDI) is a questionnaire that has been validated to discriminate between normal, mild to moderate, and severe dry eye disease as defined by the physician’s assessment and a composite disease severity score (Fig. 7.5). The OSDI has also been correlated significantly with the McMonnies Dry Eye Questionnaire, the National Eye Institute Visual Functioning Questionnaire, the physical component summary score of the Short Form-12 Health Status Questionnaire, patient perception of symptoms, and artificial tear usage.14 It has been demonstrated to have the necessary psychometric properties to be used as an end point in clinical trials, and as such, it could be an important tool for in-office support for the diagnosis of ocular surface disease that is easy to administer.15
Diagnostic Techniques in Ocular Surface Disease
Slit Lamp Examination
Schirmer Testing
Ocular Surface Staining
Tear Break-up Time
Patient Questionnaire
Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine