Diagnostic Indocyanine Green Angiography: Clinical Applications
Nicole E. Gross
Jason S. Slakter
Lindsay M. Smithen
Lawrence A. Yannuzzi
Christina M. Klais
John A. Sorenson
Richard F. Spaide
Yale L. Fisher
Dennis A. Orlock
The special properties of indocyanine green (ICG) dye and the advent of digital imaging techniques have provided for enhanced imaging of the choroid for more accurate and specific diagnoses and possibly for new insight into therapeutic strategies. ICG angiography has demonstrated its greatest potential in the diagnostic and therapeutic management of chorioretinal inflammatory diseases and, more particularly, in the area of age-related macular degeneration. An awareness of these potential advantages as well as limitations in our current understanding of ICG angiography is important to appreciate its true clinical applications.
OCCULT CHOROIDAL NEOVASCULARIZATION
The Macular Photocoagulation Study Group has provided clear and scientifically proven guidelines for the treatment of classic choroidal neovascularization (CNV) secondary to age-related macular degeneration.1,2,3,4 Unfortunately, as many as 85% of newly diagnosed exudative cases do not exhibit the classic features of CNV.5 Photodynamic therapy (PDT) using the photosensitizing drug verteporfin has recently been introduced as a method of treating a highly selective group of patients with neovascular age-related macular degeneration (AMD).6,7,8,9 PDT with verteporfin has been shown to control progression of CNV with resolution of associated serosanguineous complications and stabilization or improvement of the vision in a small subset of these patients. In the past, these patients have generally had a poor natural course. The ability to achieve a better definition and localization of the neovascular lesions in these patients with ICG angiography provides an extremely beneficial and practical clinical application for this diagnostic modality.
The first examination of CNV using ICG angiography was performed in 1976 by Patz and associates.10 Using this early film-based system, they were able to identify only 2 of 25 choroidal neovascular lesions. In a follow-up report by Bischoff and Flower of 100 ICG angiograms in patients with age-related macular degeneration, “delayed or irregular choroidal filling”11 was detected in some patients. Using ICG angiography, Hayashi and colleagues12,13 were able to detect CNV and to confirm the findings of fluorescein angiography in patients with well-demarcated or classic CNV. They demonstrated that leakage of ICG from CNV was slow compared with the rapid leakage of fluorescein. Follow-up reports using digital imaging systems as well as scanning laser ophthalmoscopy suggested that ICG angiography might be more useful in the area of occult CNV by providing enhanced imaging of the abnormal vessels.14,15,16,17
In a landmark article, Yannuzzi and associates18 demonstrated that ICG videoangiography was extremely useful in identifying well-demarcated localized areas of neovascularization in what had been classified as occult CNV by standard fluorescein angiography.19,20,21,22,23,24 In this study, 39% of 129 patients with “occult CNV” originally diagnosed as determined by fluorescein angiography were given a revised diagnosis of “well-defined neovascular lesions” based on the information obtained from the ICG study (Fig. 1). One study revealed that approximately 40% of patients with occult CNV diagnosed actually presented with early, well-defined focal areas of fluorescence on ICG videoangiography.25 They further defined two potential subgroups of occult CNV: those with and those without serous pigment epithelial detachments (PEDs) accompanying the occult neovascular process. They also pointed out that ICG angiography offered a potential advantage in identifying neovascular lesions when there was clinical evidence of recurrent CNV after previous laser photocoagulation treatment.
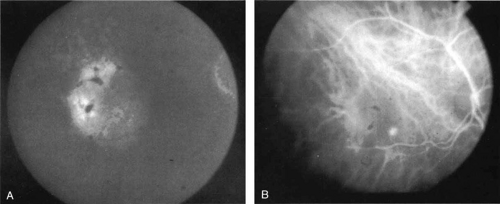 Fig. 1 A. Late-phase fluorescein angiogram of a patient with exudative age-related macular degeneration demonstrating diffuse hyperfluorescence and staining of a serous retinal pigment epithelial detachment. No localized area of classic neovascularization was identified, and the patient was classified as having occult choroidal neovascularization. B. Mid-phase indocyanine green angiogram demonstrating a focal spot of hyperfluorescence presumed to represent a localized area of choroidal neovascularization. |
Subsequently, Yannuzzi and colleagues25 and Guyer and associates26 evaluated the usefulness of ICG angiography in identifying localized areas of CNV in patients with occult CNV with or without a serous PED. In a careful evaluation of more than 680 patients, they identified 22% of patients with localized lesions that might be amenable to laser therapy—lesions that would otherwise be classified as untreatable based on guidelines for laser photocoagulation (Figs. 2 and 3). As a result of this improved imaging technique, as many as two to three times the number of patients would have been potentially eligible for laser treatment than would have been treatable based on fluorescein angiography alone.
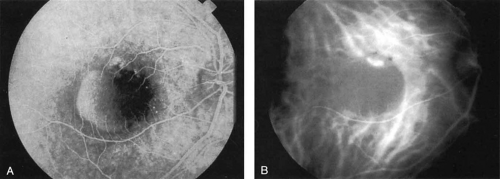 Fig. 2 A. Late-phase fluorescein study of a patient with exudative age-related macular degeneration demonstrating hyperfluorescence of the serous component of a retinal pigment epithelial detachment. There is relative hypofluorescence on the nasal aspect of the pigment epithelial detachment, and some irregular staining in the superior margin. No well-defined area of neovascularization was identified. B. Mid-phase indocyanine green angiogram demonstrating a localized area of intense hyperfluorescence corresponding to the localized area of active choroidal neovascularization. The pigment epithelial detachment is hypofluorescent. A patient with such findings was considered to be potentially eligible for laser photocoagulation therapy. |
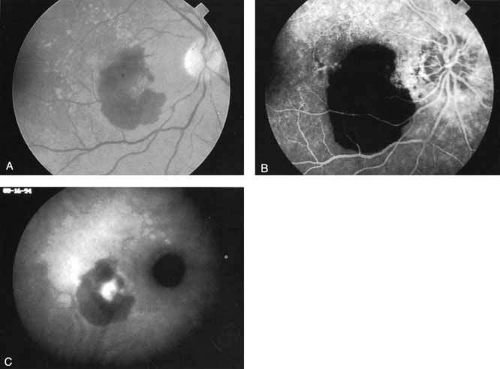 Fig. 3 A. Clinical photograph of a patient with subretinal hemorrhage secondary to exudative age-related macular degeneration. B. Late-phase fluorescein study demonstrating hypofluorescence caused by blockage by the subretinal hemorrhage. No area of choroidal neovascularization could be identified. C. Late-phase indocyanine green (ICG) study demonstrating a localized area of intense hyperfluorescence corresponding to active choroidal neovascularization. The thicker areas of subretinal hemorrhage continued to block fluorescence, even in the ICG study, but a localized area of presumed neovascularization is identified that would be potentially amenable to laser treatment. |
An important report by Chang and co-workers27 lends support to the rationale for interpreting the hyperfluorescence seen on ICG angiography as CNV. In this clinicopathologic study, a patient was identified who had experienced subretinal hemorrhage with early signs of occult CNV on fluorescein angiography (Fig. 4A). Fluorescein angiography demonstrated blocked fluorescence (Fig. 4B). The ICG study, however, demonstrated late staining in a well-circumscribed fashion, which the authors interpreted as a “plaque” of occult CNV (Fig. 4C). When the patient died, this area was evaluated and studied histopathologically and compared with the picture seen on ICG angiography. The area of hyperfluorescence on the ICG study corresponded precisely to a thin layer of fibrovascular tissue beneath the pigment epithelium and neurosensory retina, confirming that the late-staining tissue imaged with ICG angiography was truly a neovascular membrane (Fig. 4D).
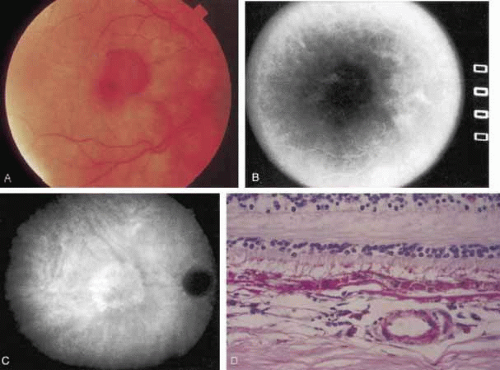 Fig. 4 A. Clinical photograph of a patient with exudative age-related macular degeneration demonstrating subretinal hemorrhage. B. Late-phase fluorescein study demonstrating blocked fluorescence from the subretinal hemorrhage. C. Late-phase indocyanine green (ICG) angiogram demonstrating a well-defined area of hyperfluorescence presumed to represent a localized plaque of choroidal neovascularization. Several months after this angiographic study was performed, the patient died and the eyes were obtained for histopathologic examination. D. Hematoxylin and eosin preparation of a section through the retina and choroid in an area corresponding to the hyperfluorescence noted on the ICG study. There is a focal area of fibrovascular tissue beneath the retina. The histopathologic study confirmed the presence of a neovascular membrane in an area corresponding to the zone of hyperfluorescence noted on the ICG study. (Chang TS, Freund KB, De la Cruz Z, et al: Clinicopathologic correlation of choroidal neovascularization demonstrated by indocyanine green angiography in a patient with retention of good vision for almost four years. Retina 14:114, 1994) |
With this clinical diagnostic and histopathologic information available, pilot studies were performed to determine the practicality of using ICG angiographic guidance in the treatment of occult CNV. Slakter and associates28 performed laser photocoagulation treatment on 79 eyes with occult CNV. The occult CNV was successfully eliminated in 57% of patients who underwent ICG-guided treatment (Figs. 5 and 6). The authors found the success rate to be higher (66%) for patients with CNV not associated with PEDs than for those with PEDs (43%). Visual acuity improvement or stabilization was achieved in 57% of all patients. Recurrences were more frequent and more difficult to control in those patients who had associated PEDs on initial clinical presentation. Additional independent studies have reported similar diagnostic and treatment outcomes with the use of ICG angiography in patients with occult CNV.29,30
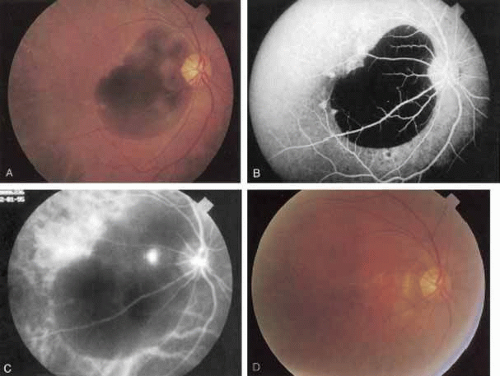 Fig. 5 A. Clinical photograph of a patient with exudative age-related macular degeneration with secondary subretinal hemorrhage. B. Late-phase fluorescein angiogram demonstrating blocked fluorescence from the subretinal hemorrhage. C. Mid-phase indocyanine green (ICG) study demonstrating blocked fluorescence from the thick areas of subretinal hemorrhage, but a localized area of intense hyperfluorescence representing active choroidal neovascularization was noted in the papillomacular bundle. Laser photocoagulation treatment was applied to this spot only. D. Clinical photograph obtained 3 months later demonstrates an atrophic scar at the site of laser treatment and complete resolution of the subretinal hemorrhage. |
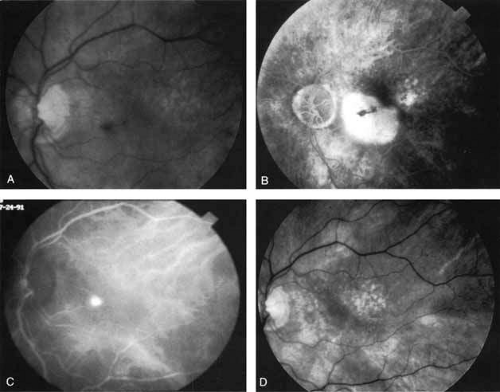 Fig. 6 A. Clinical photograph of a patient with age-related macular degeneration demonstrating a small amount of subretinal hemorrhage and a localized retinal pigment epithelial (RPE) detachment. B. Late-phase fluorescein angiogram demonstrating confluent hyperfluorescence of the serous RPE detachment. No localized area of neovascularization that would have been amenable to laser treatment was identified. C. Mid-phase indocyanine green angiogram demonstrating a focal, intensely hyperfluorescent spot representing a localized area of choroidal neovascularization. Laser photocoagulation treatment was applied only to this area. D. Clinical photograph obtained 2 months later demonstrates complete resolution of the exudative changes and a small atrophic scar at the site of laser treatment. (Yannuzzi LA, Slakter JS, Sorenson JA, et al: Digital indocyanine green videoangiography in choroidal neovascularization. Retina 12:191, 1992) |
Sorenson and colleagues31 reported on the diagnostic and therapeutic ability of ICG angiography in patients who had clinical signs of recurrent CNV but who were found to have occult membranes on fluorescein angiography. In a group of 66 patients, 97% were identified as having localized areas of hyperfluorescence on ICG angiography consistent with recurrent CNV (Fig. 7). In laser photocoagulation treatment performed in a subgroup of 29 patients, 62% achieved anatomic resolution and stabilization of the exudative process over time. Visual acuity improved in 66%, 45% of whom achieved a visual acuity of 20/100 or better.
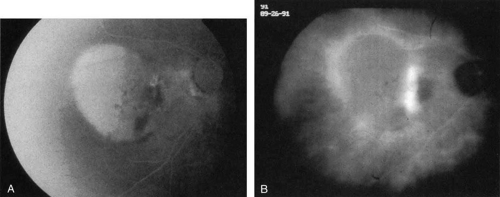 Fig. 7 A. Late-phase fluorescein study in a patient with exudative manifestations of recurrent choroidal neovascularization. There is marked hyperfluorescence of the serous component of the retinal pigment epithelial detachment, blocked fluorescence along its nasal margin, and irregular staining in the papillomacular bundle. B. Late-phase indocyanine green study demonstrating a band of intense hyperfluorescence representing recurrent choroidal neovascularization. This is noted along the margin of a localized area of hypofluorescence in the papillomacular bundle, which was the site of the previous photocoagulation treatment. Temporally, a mildly hypofluorescent retinal pigment epithelial elevation is noted. The contrast of the hyperfluorescent active recurrent neovascularization against the relative hypofluorescence of the treatment site and retinal pigment epithelial elevation helps to identify and localize the recurrent process. (Yannuzzi LA, Slakter JS, Sorenson JA et al: Digital indocyanine green videoangiography in choroidal neovascularization. Retina 12:191, 1992) |
In essence, the technique of ICG-guided laser treatment is a repetition of traditional principles employed with fluorescein angiographic imaging. The technique involves identification of a staining subretinal lesion imaged with ICG angiography, photocoagulation under ICG guidance, obliteration of the lesion, and resolution of the secondary serosanguineous complications. Obviously, stabilization or improvement of vision is a desired outcome.
Unlike fluorescein angiography, however, ICG angiographic studies have pointed out that certain principles of laser photocoagulation treatment may not hold with this new imaging capability. This is particularly true with the concept that all areas of CNV need to be obliterated to achieve a successful anatomic result. A careful evaluation of ICG angiograms in some patients with occult CNV has revealed that two forms of neovascular lesions may exist: (1) localized, intensely hyperfluorescent leaking areas of “active” CNV; and (2) more subtle and larger areas of hyperfluorescence with minimal leakage, representing “quiescent” portions of the neovascular complex (Fig. 8). A pilot study by Guyer and colleagues22 demonstrated that localized photocoagulation treatment applied to the active area of CNV alone might result in successful and long-term anatomic stabilization and improvement in the visual acuity in some patients (Fig. 9). A subsequent review of these lesions has demonstrated that they may represent a subpopulation of occult CNV known as polypoidal choroidal neovascularization, described later.
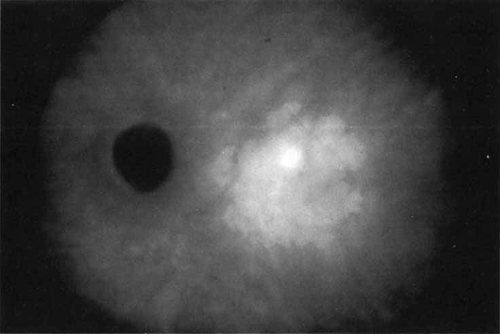 Fig. 8 Late-phase indocyanine green angiogram demonstrating a well-circumscribed are of mild hyperfluorescence in the central macula. Within this region is a localized area of more intense hyperfluorescence. This focal area is presumed to represent a more active site of choroidal neovascularization. The larger area represents a plaque of relatively more quiescent vascular growth. |
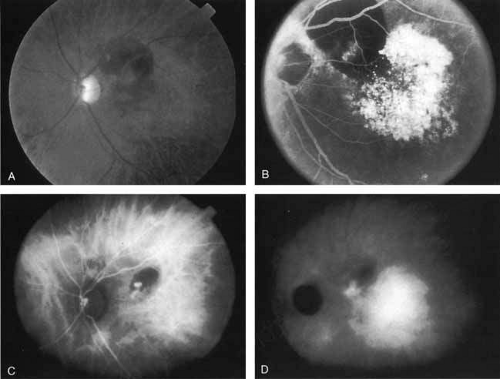 Fig. 9 A. Clinical photograph of a patient with exudative age-related macular degeneration with evidence of subretinal hemorrhage and shallow neurosensory detachment centrally. B. Late-phase fluorescein study demonstrating blocked fluorescence in the superior macula and intense hyperfluorescence and staining in the area of the neurosensory detachment (A and B, Yannuzzi LA, Slakter JS, Sorenson JA, et al: Digital indocyanine green (ICG) videoangiography and choroidal neovascularization Retina 12:191, 1992). C. Early-phase indocyanine green study demonstrating a focal area of hyperfluorescence beneath the hemorrhage. This area was presumed to be the site of more active neovascularization, D. Later-phase ICG study demonstrating the continued hyperfluorescence of the focal spot in the papillomacular bundle as well as a larger plaque of choroidal neovascularization. Laser photocoagulation was applied only to the more active focal spot of neovascularization. |
Flower revealed that feeder vessels (FVs) identified by dynamic ICG angiography, but not by FA, may be amenable to treatment with argon green laser.32 ICG angiography is then performed at regular intervals after treatment to determine the treatment response. A second laser treatment is administered if ICG angiography reveals a patent FV. A 40% success rate was found, initially, with a more recent report of 75% success.33 It appears that dynamic ICG angiography, especially high-speed ICG, detects smaller FVs and can therefore be used in treatment of these vessels. (Fig. 10)
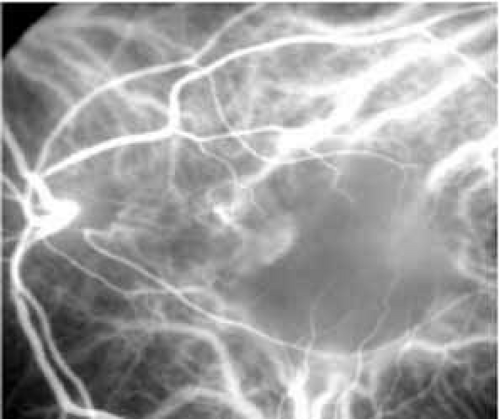 Fig. 10 High-speed indocyanine green angiography image of a feeder vessel. |
More recently, ICG angiography has begun to play an important role in the management of patients with occult CNV. In particular, the identification and management of two subsets of occult CNV, namely retinal angiomatous proliferation (RAP)34 and polypoidal choroidal neovascularization (PCV),35 are greatly enhanced with ICG angiography. RAP is a distinct subgroup of neovascular AMD in which angiomatous proliferation within the retina is the first manifestation of the process of neovascularization. As the neovascularization proliferates into the outer retina and subretinal space, the angiomatous proliferation is then surrounded by dilated retinal vessels, hemorrhages (preretinal, intraretinal, and subretinal), and exudates. One or more of the related, compensatory retinal vessels perfuse and drain the neovascularization, occasionally forming a retinal–retinal anastomosis (RRA). In these patients, the same indistinct staining seen in occult CNV is present on a fluorescein angiogram. Therefore, most cases of RAP require the use of ICG angiography to make the diagnosis (Fig. 11).34
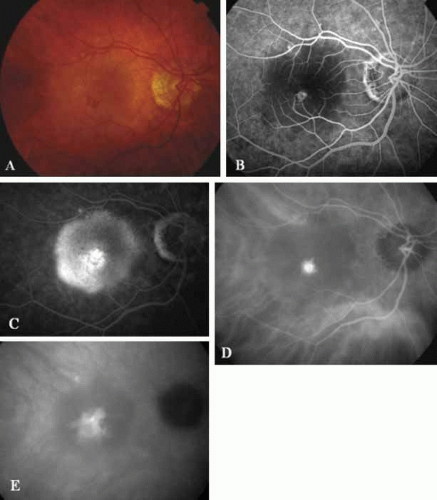 Fig. 11 A. Clinical photograph of a patient with retinal angiomatous proliferation (RAP). There is a hemorrhage with a retinal pigment epithelial detachment. B. Early-phase fluorescein angiogram demonstrates the retinal–retinal anastomosis. C. Late-phase fluorescein study demonstrates the late-staining hyperfluorescence seen in RAP lesions with a hyperfluourescent retinal pigment epithelial detachment. D. Mid-phase indocyanine green study demonstrates the hyperfluorescent hot-spot overlying the hypofluorescent retinal pigment epithelial detachment. E. Late-phase ICG angiogram demonstrates late hyperfluorescent leakage (CME) into the retina. |
ICG angiograms of RAP lesions reveal a focal area of intense hyperfluorescence corresponding to a so-called hot-spot of neovascularization with some late extension of the leakage within the retina caused by intraretinal neovascularization (IRN) within the deep layers of the retina. As the IRN progresses down into the subretinal space, the neovascularization present in the choroid joins the IRN to form a large, neovascular complex. At this stage, clinical and angiographic evidence of a vascularized PED (V-PED) is often present. ICG is the preferred method of imaging a V-PED because the serous component of the PED remains hypofluorescent while the vascular component displays hyperfluorescence. ICG angiography may be able to capture direct communication between the retinal and choroidal component of the neovascular complex as they meet to form a retinal choroidal anastomosis (RCA).34 Treatment options of RAP lesions include: traditional laser photocoagulation of the stage 1 and early stage 2 lesions, surgical excision of stage 2 lesions in conjunction with laser diathermy, as well as PDT, alone and in combination with other treatments, particularly triamcinolone acetonide.36,37 Other therapies, both singly and in combination, are currently undergoing investigation for this unique form of neovascular AMD.
Although initially reported exclusively in middle-aged, black females, PCV has since been recognized as a variant of CNV that can be found in all patients with AMD. This entity is characterized by the presence of an inner choroidal vascular network ending in an aneurysmal bulge clinically seen as a red–orange, spheroid, polyp-like structure. Leakage and bleeding from the choroidal vascular abnormalities result in multiple, recurrent, serosanguinous RPE detachments.25,39,40,41 ICG can be used to identify and characterize the vascular abnormality with high sensitivity and specificity.19,20,21,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59 Early-phase images of the lesions show a distinct network of vessels within the choroid. Patients with juxtapapillary involvement show a radial, arching pattern with an inner network of vascular channels extending and connecting with smaller, spanning branches that are more numerous and increasingly prominent at the edge of the PCV lesion.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


