Other sequences, such those as with fat-saturation or suppression, can help to confirm fat content and make enhancement more conspicuous when the high signal of fat is nulled.
TABLE 27.1 COMPARISON OF CT AND MRI PRINCIPLES, PROTOCOLS, INDICATIONS AND POTENTIAL RISKS | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
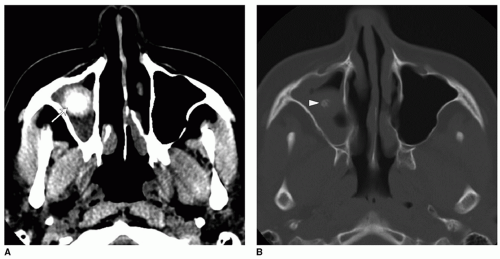 Figure 27.1 Fungus ball in soft tissue and bone windows. A: Axial CT image with soft tissue windows shows a right maxillary sinus high-density rounded mass (arrow). B: Axial CT image with bone windows shows central calcification (arrowhead) within the mass. Note that the fungus ball and mucosa have different density appearances on soft tissue window, which cannot be appreciated on bone windows. On bone windows, the calcifications and bony structures are more conspicuous. |
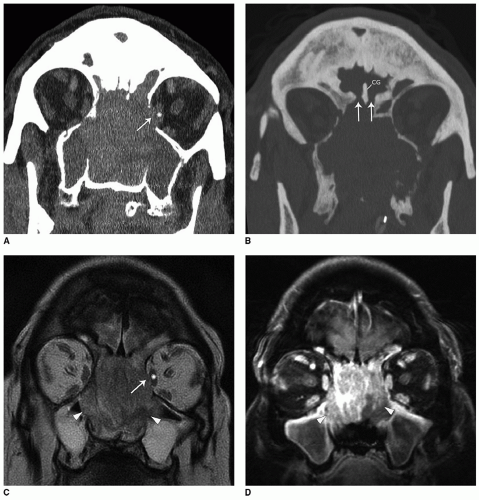 Figure 27.2 Sinonasal carcinoma with invasion of anterior cranial fossa and bony orbit. Differences between CT and MRI. A: Coronal CT image shows complete opacification of the bilateral nasal cavity and paranasal sinuses. There is bony destruction at the medial wall of the left orbit (arrow) with loss of fat plane around the medial rectus muscle (asterisk). B: Coronal CT image shows bony destruction at the cribriform plate (arrows). CG, crista galli. C: Coronal T2-weighted MRI image more clearly depicts the difference between isointense tumor mass (arrowheads) filling the nasal cavity and hyperintense inflammatory fluid in the maxillary sinuses. Tumor bows into the orbit (arrow), but a smooth contour suggesting that the periorbita is intact. The medial rectus muscle (asterisk) has normal signal and size. There is no intracranial mass despite anterior skull base bony destruction. D: Coronal enhanced T1-weighted MRI image shows enhancing tumor in the nasal cavity (arrowheads) extending into the frontal sinuses. Note that MRI is better than CT in differentiating between tumor and fluid-filled maxillary sinuses, which are T2 hyperintense and nonenhancing. |
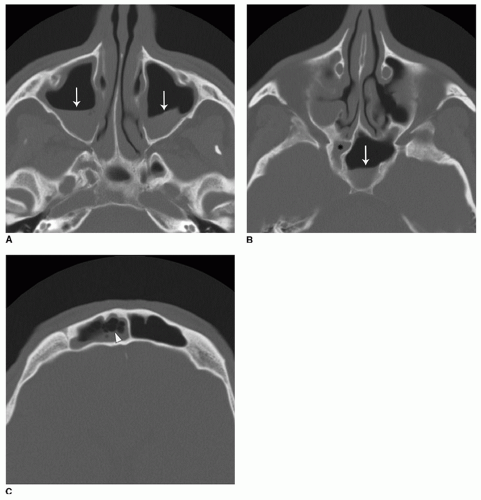 Figure 27.3 Acute sinusitis. Axial CT images through the (A) maxillary, (B) sphenoid, and (C) frontal sinuses showing layering air-fluid levels (arrows). There are also frothy secretions in the right frontal sinus (arrowhead). |
cause of acute maxillary sinusitis is odontogenic infection. This should be suspected if the CT findings of sinusitis are severe in the presence of an oroantral fistula, periodontal lucency (abscess), or a tooth root projecting into the maxillary sinus (Fig. 27.4) (5). The typical finding in chronic rhinosinusitis is significant mucosal thickening or opacification in a nonexpanded sinus, often with ostial obstruction. A characteristic, but less common sign of chronic rhinosinusitis is sclerosis and thickening of bony sinus walls, particularly seen in the sphenoid and maxillary sinuses (Fig. 27.5). Chronic rhinosinusitis may also be associated with high-density opacification that often represents viscous or desiccated secretions, but can also be a sign of coexisting allergic fungal rhinosinusitis or fungus ball.
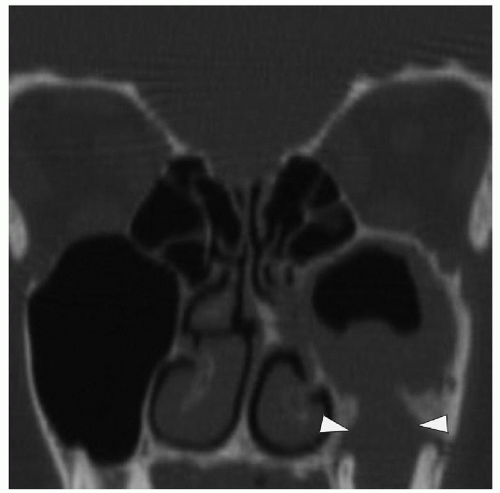 Figure 27.4 Odontogenic maxillary sinusitis. Coronal CT image shows a left molar periapical abscess (arrowheads) contiguous with the left maxillary sinus in keeping with an oroantral fistula. There is mucosal thickening and possibly fluid in the left maxillary sinus. Other paranasal sinuses are normal. |
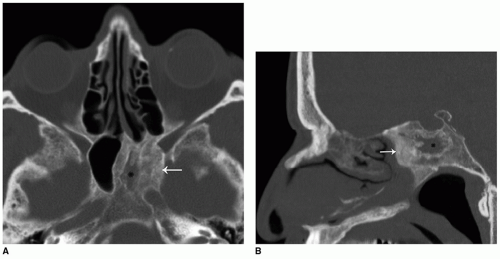 Figure 27.5 Chronic sinusitis. A: Axial and B: sagittal CT images show opacification of the left sphenoid sinus (asterisks) with bony sclerosis and wall thickening (arrows). |
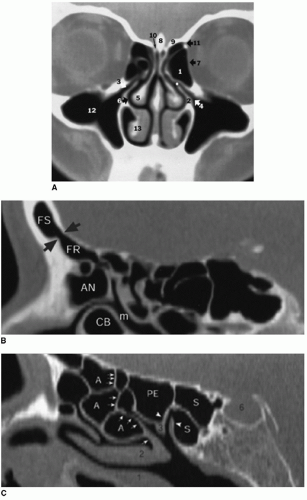 Figure 27.6 Normal paranasal sinus anatomy. A: Coronal CT image shows the normal OMC. Components of the ostiomeatal complex (OMC) are as follows: 1, bulla ethmoidalis; 2, uncinate plate; 3, infundibulum; 4, inner maxillary sinus ostium; 5, middle turbinate; 6, middle nasal meatus; *, hiatus semilunaris. The following are other important landmarks on this image: 7, lamina papyracea; 8, crista galli; 9, fovea ethmoidalis; 10, medial lamella; 11, anterior ethmoidal foramen; 12, maxillary antrum; 13, inferior turbinate. B: Sagittal CT image shows the frontal recess. The frontal ostium (arrows) produces the waist of the classic hourglass configuration. Inferiorly, a large agger nasi cell bulges posteriorly to severely narrow and distort the recess. FS, frontal sinus; FR, frontal recess; AN, agger nasi; L, lacrimal bone; CB, concha bullosa; m, middle nasal meatus. C: Sagittal CT image shows the sphenoethmoidal recess (SER) (arrowheads). S, sphenoid sinus; PE, posterior ethmoidal sinus; A, anterior ethmoidal sinus; arrowheads, SER; 1, inferior turbinate; 2, middle turbinate; 3, superior turbinate; arrows, basal lamella. |
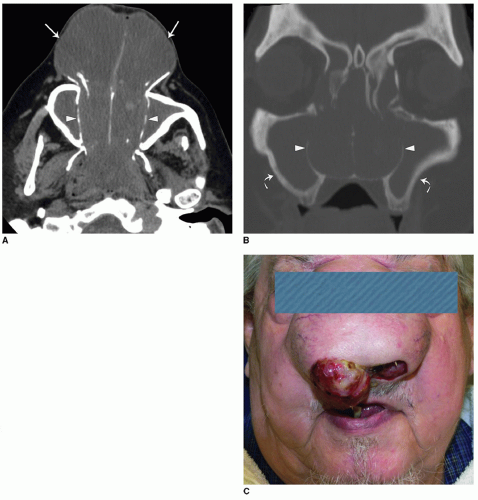 Figure 27.7 Sinonasal polyposis. A: Axial CT image shows complete opacification of the nasal cavity with soft tissue density masses projecting through the nostrils (arrows). There is bony thinning of the walls of the nasal cavity (arrowheads). B: Coronal CT image show nasal cavity opacification with thinning of the walls of the nasal cavity (arrowheads). There is also opacification of the maxillary sinuses with bony sclerosis and thickening (curved arrows). C: Photograph of polyps causing cosmetic deformity of the nose. |
collections of fluid (serous retention cysts) or collections from an obstructed seromucinous gland (mucous retention cysts). They most frequently occur in the maxillary antrum and appear as smooth, outwardly convex soft tissue density masses. On CT, it is difficult to differentiate a cyst from a polyp since both have soft tissue density. On MRI, a cyst does not enhance except for its mucosal surface. A polyp represents hyperplastic mucosa and will solidly enhance.
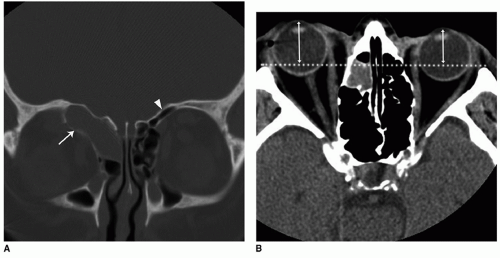 Figure 27.8 Frontal sinus mucocele with proptosis. A: Coronal CT image shows rounded expansion of the right frontal sinus with bony thinning (arrow) compared to the normal left frontal sinus (arrowhead). B: Axial CT image shows right proptosis due to mass effect from the mucocele. The dotted line is the interzygomatic line and allows comparison of the position of the right and left globe (double arrowed lines). |
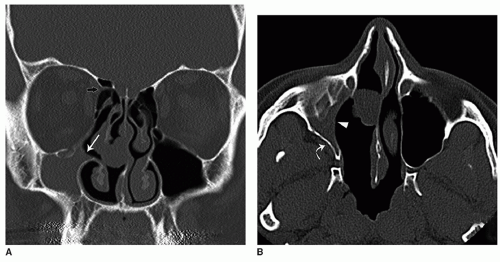 Figure 27.9 Atelectatic sinus. A: Coronal CT image shows a smaller right maxillary sinus. There is lateral rotation of the uncinate process (white arrow) that widens the space between the uncinate process and the middle turbinate. Note also the normal “nipple sign” indicating the anterior ethmoidal foramen (black arrow). B: Axial CT image shows smaller right maxillary sinus with inward bowing of the posterior (curved arrow) and medial walls (arrowhead) of the maxillary sinus. The atelectatic sinus predisposed the patient to complications during endoscopic sinus surgery (ESS). |
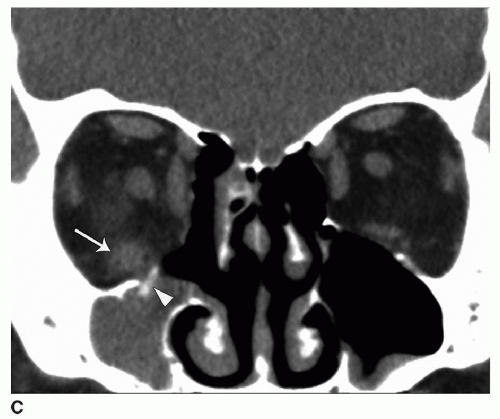 Figure 27.9 (Continued) C: Postoperative coronal CT image of patient in A and B demonstrating the ESS complication of a fracture to the floor of the orbit (arrowhead) and injury to the inferior rectus muscle with enlargement and fat stranding (arrow). Courtesy of MT Bhatti, MD, Duke University Medical Center. |
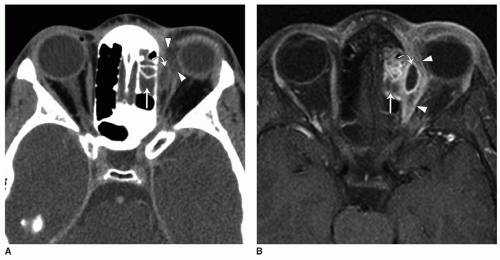 Figure 27.10 Orbital subperiosteal abscess complicating ethmoid sinusitis. A: Axial-enhanced CT image shows left ethmoid sinus opacification from acute sinusitis (arrow) and left orbit extraconal fat stranding (arrowheads). There is a small low attenuation collection (curved arrow) that is better seen on MRI. B: Axial-enhanced fat-saturated T1-weighted image shows left ethmoid sinus mucosal enhancement from acute sinusitis (arrow) and left orbit extraconal fat enhancement (arrowheads). There is a small ring-enhancing collection (curved arrow) representing an abscess. |
intracranial contents. Meningoceles and encephaloceles appear on CT as a soft tissue mass abutting the skull base with focal bony dehiscence. The diagnosis is best confirmed with MRI. Meningoceles show T2 hyperintensity due to the presence of cerebrospinal fluid (CSF). Encephaloceles are characterized by a soft tissue mass with signal isointense to gray matter and contiguity to intracranial parenchyma (Fig. 27.14).
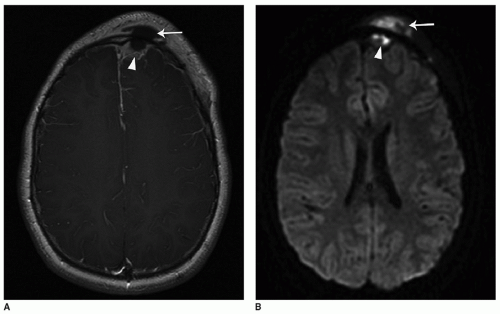 Figure 27.11 Pott puffy tumor with epidural empyema. A: Axial-enhanced T1-weighted image shows a hypointense collection overlying the left frontal bone (arrow) that is continuous with a rim enhancing extraaxial (outside brain parenchyma) collection overlying the left frontal lobe (arrowhead). B: Axial diffusion-weighted image shows bright signal in the collections indicating restricted diffusion. This supports the diagnosis of abscess. |
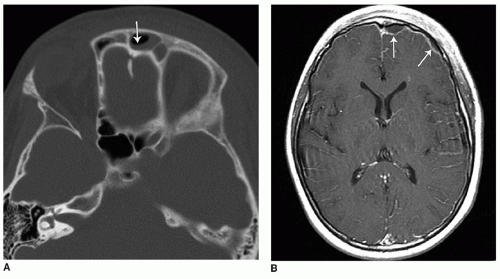 Figure 27.12 Subdural empyema complicating frontal sinusitis. A: Axial CT image shows left frontal sinus opacification with an air-fluid level (arrow) suggestive of acute sinusitis. B: Axial-enhanced T1-weighted MRI image of the brain shows a rim-enhancing crescentic extraaxial collection overlying the left frontal lobe consistent with a subdural empyema secondary to acute sinusitis. |
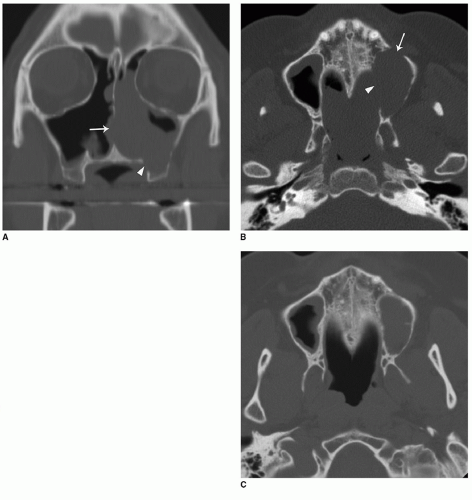 Figure 27.13 Bony destruction from sinonasal sarcoma. A:
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|