Fig. 1
Endoscopic view of laryngomalacia at time of supraglottoplasty. Note curled epiglottis and anteromedial displacement of supra-arytenoid mucosa
If an infant has been intubated or suctioned around the time of birth, details about the mode of instrumentation, size of endotracheal tube, and duration of intubation can also shed light on etiology. A neonate who has been intubated even for a few seconds to suction meconium in the delivery suite can suffer laryngeal trauma. While such trauma is almost always minor, a few infants have developed laryngeal granulomas that cause inspiratory stridor and hoarse cry a few days after birth [2].
The history should also include details about feeding, including changes in stridor quality and intensity during and after feeding. An infant with stridor who has feeding difficulties or poor weight-gain may have more severe airway obstruction. Feeding difficulties may reflect poor coordination of swallow during the increased work of breathing with airway obstruction. Poor feeding in the presence of stridor can occur with laryngotracheal lesions that directly impair swallowing. Infants with large laryngeal clefts can have stridor from inspiratory collapse of the redundant posterior supraglottic tissues surrounding the cleft, as well as the more classic aspiration of feeds through the abnormally patent posterior larynx. Infants with gastroesophageal reflux can develop noisy breathing from an edematous, irritated larynx, or from aspiration of refluxate or swallowed feeds. While neonates with laryngomalacia can have associated esophageal or even pharyngeal reflux of gastric contents, such reflux may result secondarily from increased intrathoracic pressures created by the airway obstruction at the laryngeal level [3].
A history of an abnormal cry, perhaps high-pitched, hoarse, or even aphonia, focuses the evaluation for stridor to glottic (true vocal cord) lesions. Neonates can have inspiratory stridor from unilateral vocal cord paralysis, as the one immobile cord causes relative airway narrowing at the glottic level. These infants have hoarse or weak cry because the immobile vocal cord, usually paralyzed off the midline (the so-called paramedian position), cannot abut the mobile vocal cord during phonation or cry. Neonates with bilateral vocal cord paralysis have more severe stridor and airway obstruction, but the quality of cry may be closer to normal than in those with only one immobile vocal cord. Neonates with abnormal cry can also have abnormalities of vocal cord structure, such as an anterior glottis web that both restricts vocal cord motion and narrows the glottis airway (Fig. 2). Small glottic webs may not cause stridor, but large webs can cause severe airway compromise and stridor, as they have longer lengths of fused vocal cords and are often associated with subglottic stenosis.
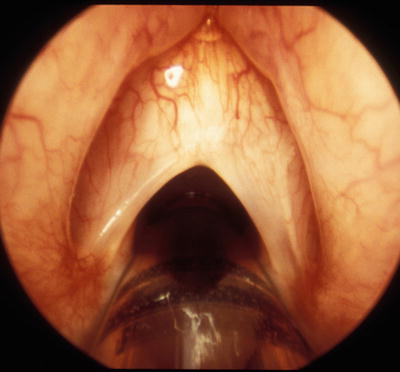
Fig. 2
Anterior commissure web causing dysphonia but almost no stridor, as web extends for about 1/3 of glottis length
A history of barky or croupy cough or history of treatment for recurrent or atypical croup-like illnesses points to a subglottic abnormality. Any history of laryngeal instrumentation suggests the possibility of subglottic stenosis or cysts, although congenital subglottic stenosis can present as recurrent croup-like illness without any history of previous intubation. A subglottic hemangioma can cause barky cough and stridor that may transiently respond to the steroid treatment given for presumed croup. Subglottic hemangiomas usually cause inspiratory or biphasic stridor in the first few months of life, but not at birth, as the airway lesion proliferates early in infancy [4] (Fig. 3).
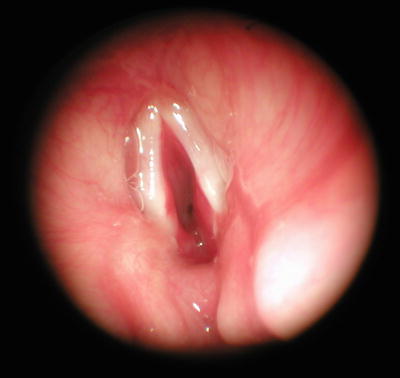
Fig. 3
High-grade airway obstruction from near circumferential involvement of subglottic hemangioma
A detailed history should also elucidate any possible syndromic diagnoses, familial disorders, or multi-system diseases that could explain neonatal stridor. Familial neonatal vocal cord paralysis has been described. Neonates with central nervous system abnormalities such as hydrocephalus or Arnold-Chiari malformation can present with stridor secondary to vocal cord paralysis. Children with congenital heart anomalies can have tracheal compression from cardiac enlargement or from associated anomalous intrathoracic vasculature; unilateral vocal cord paralysis is similarly associated with congenital heart disease. Vocal cord paralysis and subglottic stenosis are both seen in young children after corrective cardiac surgery and postoperative respiratory support [5].
A careful past surgical history is critical to determine the etiology of neonatal stridor, particularly for those who have had intervention to close a patent ductus arteriosus (PDA) or have required extracorporeal membrane oxygenation (ECMO) with cannulation of neck vessels [6, 7]. PDA ligation and ECMO have been associated with unilateral vocal cord paralysis causing neonatal stridor, dysphagia, and dysphonia, by impaired function of the left recurrent laryngeal nerve (PDA) and the cervical vagus nerve (ECMO) motor innervations to the larynx.
The SPECS stridor history mnemonic, described by Hollinger, is a useful construct to focus history-taking, and to determine the speed of subsequent evaluation and need for intervention [8]. The assessment includes: S—Severity, P—Progression, E—Eating, C—Cyanotic spells: Apparent life–threatening events, S—Sleep: Obstruction so severe that retractions occur even during sleep.
Severity
The subjective impression regarding the severity of the obstruction and any accompanying respiratory distress, determines the urgency of planned investigations. The seemingly well neonate with mild stridor, no respiratory distress, and good feeding can have an orderly evaluation usually in the office setting, but the infant with signs of severe airway compromise requires immediate intervention for diagnosis and possible intervention. While this assessment is mainly that of the bedside physical examination by experienced observers, the observations of parents and other caregivers are important.
Progression
Stridor that is present at birth suggests a fixed congenital narrowing such as choanal atresia, laryngeal web, vocal cord paralysis, and subglottic or tracheal stenosis. If the stridor progresses during the first few weeks of life, and symptoms change with position and awake/asleep state, a dynamic lesion such as laryngomalacia is possible. If symptoms worsen steadily over time, with louder or more persistent stridor or worsening associated signs and symptoms, an enlarging airway mass such as subglottic hemangioma may be present.
Abrupt onset of stridor, with rapid progression, suggests infectious or inflammatory airway issues, such as viral croup, tracheitis, or epiglottitis. Such laryngeal infection is unusual in neonates. This clinical picture is also seen with airway trauma or foreign body aspiration. While foreign body aspiration is often seen in toddlers and young children, the rare reports of neonatal foreign body aspiration usually involve iatrogenic airway foreign bodies associated with neonatal respiratory support [9].
Eating
Any history of feeding difficulties, symptoms of aspiration, or failure to thrive suggests more severe airway obstruction or an anatomic lesion that affects swallowing as well as airway patency. Lesions of the nasal cavity, nasopharynx, and pharynx are more likely to cause feeding difficulties than those in the lower airways. Slow feeds, frequent pauses for breathing, and cough or spitting-up with feeds may be reported in some stridorous neonates. As discussed above, aspiration and cough can occur in infants with vocal cord paralysis, tracheoesophageal fistula, or laryngeal clefts, each of which can interfere with the necessary exclusion of food from the airways. Additionally, tracheal obstruction and esophageal compression can coexist, particularly with intrathoracic vascular anomalies such as the double aortic arch and other compressive rings (Fig. 4a, b).
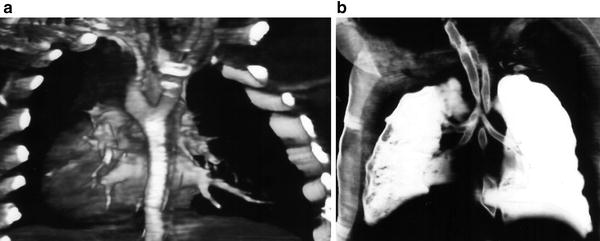
Fig. 4
Enhanced computed tomographic images of (a) double aortic arch surrounding the trachea and the esophagus causing (b) severe narrowing of the distal trachea
Cyanotic Spells
Any stridorous infant who has cyanotic spells, severe respiratory distress with neck or chest retractions, or with a history of a “near-miss” or apparent life-threatening event (ALTE) requires urgent evaluation and management. These infants are usually admitted for cardiorespiratory monitoring and multidisciplinary work-up. Cardiovascular and central nervous system disorders need to be excluded in the infant with cyanotic spells and ALTE, particularly when stridor is intermittent or absent. However, an infant with a confirmed airway lesion can have concomitant cardiovascular, pulmonary, and/or central nervous system disorders. This is often the case in syndromic infants, as well as in neonates who have had prolonged, complicated intensive care unit stays.
Sleep
Stridor may improve or may worsen during sleep. Some neonates with airway obstruction will suffer from obstructive sleep apnea, with relaxation of upper airway musculature causing multi-level airway obstruction. Airway obstruction at the pharyngeal level often worsens during sleep, most classically demonstrated by infants with glossoptosis and the Pierre-Robin triad. Stridor from laryngeal and tracheobronchial obstruction usually is loudest in the awake and agitated infant, with fewer symptoms during sleep.
Physical Examination
The general examination of the neonate with stridor is a key in determining the severity of airway compromise. In addition to routine vital signs, pulse oximetry may be helpful as a screen for severe respiratory difficulties. One should be cautioned that a normal room air arterial oxygen saturation reading by no means excludes severe airway obstruction, as ventilation may be severely compromised before arterial oxygen desaturation occurs. The nature of the stridor can be determined, with relation to the phase of respiration as well as whether it is high or low-pitched, constant or intermittent, or variable with body position.
The presence of tachypnea, severe retractions, lethargy, cyanosis, or seemingly poor airway movement in an infant with stridor suggests the need for near simultaneous airway evaluation and airway support. In some circumstances this requires urgent transport to the operating room for diagnostic airway endoscopy and support with endotracheal intubation, tracheotomy, or other intervention depending on the nature of the airway lesion. The neonate with stridor who is otherwise stable can usually be evaluated in the clinic setting or at the bedside.
The general examination will include inspection of the head and neck, with attention to presence or absence of craniomaxillofacial deformities. Infants with microtia, absence or deformity of one or both auricles, can have associated mandibular hypoplasia and asymmetry, resulting in relative airway obstruction (Fig. 5). More obvious deformities of the external nose, nasal ala, mouth shape and size, jaw size and position, etc. should be documented. Infants with facial hemangiomas, especially those around the lips, mouth, and chin, may have stridor from laryngeal hemangiomas. Inspection of head and neck, the chest wall anatomy and dynamics, as well as the limbs, may suggest a syndromic diagnosis that includes an airway abnormality. For example, an infant with stridor, misshapen helices, and a submucosal cleft palate may have velocardiofacial syndrome, a condition that is associated with glottic webs and vascular rings.

Fig. 5
Infant with severe airway obstruction from mandibular hypoplasia. Note associated ear anomalies
The nose is examined, looking at size, patency of nostrils, abnormal secretions and masses. The choanal openings can be assessed by passing catheters through the nose, but it is a simple task to assess choanal patency during transnasal fiberoptic laryngoscopy. The oral cavity and oropharynx is inspected for masses, abnormal tongue shape and position, overt and occult palate clefts, etc. While obstructive airway lesions may not be seen, the clinician may see features to suggest more diffuse issues with neuromotor tone or even syndromic diagnosis.
Auscultation of the lung fields and even over the neck/larynx may amplify features of the stridor, particularly for children with intrathoracic lesions, cardiac disease, or abnormalities of chest wall/lung dynamics. The neck should be examined to look for retractions as well as for masses that may affect airway function.
Symptoms of airway obstruction, including stridor, may vary with position of the infant. The exam can include evaluation while supine, prone, and upright. The infant with laryngomalacia has worsened stridor when supine, improved when upright or prone. Similarly, the micrognathic infant with airway compromise from the Pierre-Robin triad is worse in the supine position, but airway obstruction in this infant worsens when sleeping, unlike infants with laryngomalacia.
When stridor is subtle or not observed in the clinic setting, we ask parents to make audio–video recordings, often using smartphone cameras, to help share concerning observations. Additionally, we will observe for the emergence of stridor in the active/agitated infant, usually during the fiberoptic laryngoscopy described later in this chapter.
Specialized Examinations and Procedures
Fiberoptic Laryngoscopy (FOL)
Fiberoptic laryngoscopy, or flexible laryngoscopy, is the key to our specialized examination to assess both dynamic and fixed lesions of the upper airway, viewing from the nose to the larynx. We routinely perform this in the clinic for the great majority of infants with stridor, once we have ruled out severe airway compromise. While the indication we discuss here is neonatal stridor, fiberoptic laryngoscopy is also used to evaluate stertor, feeding difficulties, cough, or abnormal cry in infants.
Fiberoptic laryngoscopy is most often performed in an awake infant who is held upright on the lap of an assistant (Fig. 6). While topical decongestants such as oxymetazoline can be used to reduce mucosal swelling in the nose, the routine use of topical anesthetics (lidocaine, tetracaine) is avoided in neonates who have respiratory and/or swallowing issues, as impaired pharyngeal sensation may worsen respiratory function. While small caliber scopes (2.7 mm) have been developed for use in neonates, the senior author prefers a 3.5 mm scope for most full-term neonates and young infants, as the larger scope provides better image quality. The small caliber scopes are useful for preterm infants or infants with nasal narrowing such as seen with piriform aperture stenosis. Video recording is routine, and is useful for serial documentation of changing lesions, careful assessment of dynamic issues such as vocal cord motion, and education of parents/caregivers.

Fig. 6
Awake fiberoptic laryngoscopy to evaluate a young infant with stridor
The flexible scope is passed through both sides of the nose and advanced to the nasopharynx, assessing for nasal patency and obstructive masses. Nasal masses such as congenital dacryocystoceles can cause airway distress in neonates, who are obligate nasal breathers, as can choanal stenosis or atresia. Soft palate movement can be assessed, nasopharyngeal narrowing can be viewed, and hypopharyngeal anatomy and dynamics can be observed. A detailed view of the anatomy and movement of the base of tongue, the supraglottic larynx, and the vocal cords with respiration should be obtained, The subglottis can often be seen during full abduction of the vocal cords, but most practitioners will not routinely advance the scope below the vocal cords during the evaluation of an awake stridorous neonate in the clinic setting.
This examination can also be performed rapidly at NICU/nursery bedside or in the clinic setting, and requires no sedation or airway control. It is ideal for assessing dynamics of respiration such as pharyngeal tone, tongue position, supraglottic collapse, and vocal cord motion, all of which can be correlated with observed respiratory sounds. The subglottis and trachea are not visualized, so lesions such as subglottic or tracheal stenosis are best diagnosed with operative laryngoscopy and bronchoscopy. Posterior laryngeal clefts can be missed on fiberoptic laryngoscopy because the redundant tissues around the cleft may obscure the lesion.
Fiberoptic endoscopic evaluation of swallowing (FEES) has been introduced as a method to assess swallowing abnormalities in infants with feeding problems, with or without observed airway obstruction and/or stridor. The FOL examination described above is supplemented with real-time observation of the hypopharynx and larynx during swallows of colored boluses of varying consistencies. The ability to exclude the swallowed material from the laryngeal intraoitus and trachea is assessed, and laryngeal and hypopharyngeal sensation can be tested as well. FEES has been used to look for anatomic correlates of swallow dysfunction as a supplement to video-fluoroscopic assessments (“modified” barium swallow). FEES also can be used as a primary assessment of swallow function in neonates to limit exposure to the ionizing radiation of fluoroscopy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


