4

Diagnosis and Management of
Rhinosinusitis
Prior to considering management of rhinosinusitis, the physician must be certain about the diagnosis. Proper diagnosis is achieved only with thorough knowledge about the pathophysiology and etiology of the disease. Accurate diagnosis and subsequent treatment are achieved by complete understanding of the symptoms and signs of the disease, the ability to perform an accurate head and neck examination, and understanding of the subtle significance of findings seen on computed tomography scans and nasal endoscopic examination. Once the disease is certain, treatment options need to be available that include both medical and surgical options.
In the United States, rhinosinusitis is an extremely common disease and is increasing in prevalance. There were over 32 million cases of sinusitis reported and 11.6 million patient visits, mostly to primary care physicians. Since 0.5% to 5% of viral upper respiratory tract infections result in rhinosinusitus, it is estimated that from the 1 billion viral infections there would be about 20 million cases of acute bacterial rhinosinusitis.3,4 Not only is acute sinusitis common, but it is also costly, with approximately $3.5 billion spent each year in the United States.5 The cost of management of sinusitis in 1994 to the U.S. health care system was $2.4 billion, and this does not include diagnostic evaluation, such as adiology, or surgery.
Restricted activity days are the number of days a person is away from customary activities. From 1986 to 1988, there were 50 million such days. From 1990 to 1992, there were 73 million restricted activity days, which is almost a 50% increase in the number of days compared with the period 1986 to 1988. These numbers suggest that sinusitis is increasing in frequency or severity.
Although the majority of those afflicted with rhinosinusitis have self-limited disease or are managed easily by their primary care physicians, there are those with difficult and frustrating problems who eventually make their way to the otolaryngologist. It is then the subspecialist otolaryngologist who must be adequately armed to diagnose and manage the disease so that the patient may reasonably and efficiently return to work, family, school, social encounters, and activities of enjoyment.
Poor air quality in spite of improved automobile, bus, truck, and industrial emissions may be one of the reasons for the increase in the frequency and/or severity of sinusitis (Fig. 4–1). In the Great Lakes area of the United States, for example, there are many manufacturing, steel, and automotive industries. In 1993, the Environmental Protection Agency measured air quality and pollution in the United States. The 8-hour carbon dioxide concentration in the Steubenville-Weirton area (~75 miles southwest of Cleveland, Ohio) was fifth highest. The average particulate count in Cleveland and the cities around Cleveland was fourth highest. Sulfur dioxide content was the highest in the United States in the SteubenvilleWeirton area, seventh highest in Youngstown and Warren, Ohio (smaller communities between Cleveland and Pittsburgh, Pennsylvania), and tenth highest in Cleveland. Many people refer to this part of the United States as the “sinus belt,” and it may very well be so, just because of the air quality and pollution.
Evaluation begins with the patient history. A good history is dependent upon knowledge of the etiology and pathophysiology of the disease. If the etiology is understood, then the treatment is usually easier and more successful. Most physicians agree about the common causes and predisposing factors for sinusitis. These include upper respiratory infections, allergic rhinitis, asthma, day care centers, environment such as cigarette smoke (both active and passive), air pollution, structural abnormalities such as deviated nasal septum, and nasal polyps. Less common predisposing factors are immunodeficiency, swimming, adenoiditis, foreign body, cystic fibrosis, substance abuse, and neoplasm.
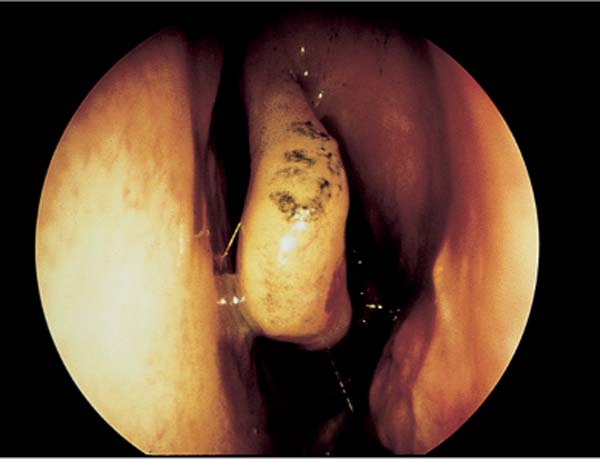
FIGURE 4–1 Air pollution causing particulate matter to lodge on the middle turbinate, creating irritation and edema.
A few general comments are needed about some of these etiologic and predisposing factors.
It may be difficult to differentiate infectious rhinosinusitis from a common self-limited viral upper respiratory infection, allergic rhinitis, or vasomotor rhinitis. The ability to determine this may be clearer with the more recent definitions of rhinosinusitis (see below). If allergic rhinitis is present, then sinusitis is generally preceded by the typical allergic symptoms of itchy eyes, itchy nose, watery eyes, and sneezing fits. Mucus tends to be thin and watery in allergic rhinitis and thick and purulent in infectious rhinosinusitis. Vasomotor rhinitis generally has symptoms of watery nasal drainage and nasal obstruction that alternates from one side of the nose to the other. Some factors that incite vasomotor rhinitis are perfume, cigarette smoke, light, cold, foods (especially beer and wine), pregnancy, certain medications, and stress.
If asthma is present and out of control, sinusitis may be the cause, and evaluation is needed. There may be associated aspirin or nonsteroidal anti-inflammatory drug sensitivity. This is often called triad asthma, Samter’s triad, or Fernand Widal triad and is an abnormality in the arachidonic acid metabolic cycle. It most commonly affects young adults ages 20 to 40. Triad asthma is often a frustrating management problem for the patient, primary care physician, and otolaryngologist because of repeated rhinosinusitis, sinus and nasal polyps, and asthma out of control. These patients require ongoing medical management for their pulmonary problems, infectious rhinosinusitis, and nasal polyps, and often frequent surgery to remove polyps and relieve obstruction.
Day care centers commonly have been places where young children go while parents are at work. They also can be places where respiratory disease is transmitted because of close and direct contact. However, day care centers are no longer limited to just children. In addition to the pediatric day care centers, there is an increasing number of adult day care centers because of the growing aging population in the United States. Anytime there are centers where people come together of any age, there is a greater chance that they will contract an upper respiratory tract infection and develop sinusitis.
Although immunodeficiency syndromes are uncommon, they must be looked for when there are recurrent episodes of respiratory tract infection and the traditional management has failed. Whether it is an adult or a child, immunodeficiency should be considered if a patient is experiencing frequent upper respiratory tract infections, sinusitis, otitis media, pneumonia, or bronchitis. If the patient has frequent, severe, or resistant disease, the immune system should be evaluated.
It is not clear whether swimming causes or worsens rhinosinusitis. Although there is no scientific evidence, some physicians feel that there are increased symptoms of sinusitis if there is frequent swimming in polluted water or when diving water is forced into the nasal and sinus cavity and becomes trapped.
In children, adenoiditis must be considered as an etiology for rhinosinusitis. Tonsillitis is frequently considered as part of the cause of upper respiratory tract disease, but adenoiditis is infrequently considered. In the pediatric patients adenoiditis may cause sinusitis, or sinusitis may cause adenoiditis. This is not clear. Enlarged adenoids may become infected and seed the sinuses or may merely obstruct the flow of secretions from the nasal and sinus cavities into the throat, causing stasis of secretions and subsequent infection. In a child who has repeated and medically unresponsive sinusitis and adenoid hypertrophy, an adenoidectomy is often performed before surgical intervention for sinus disease and is successful. It is less invasive, more conservative, and often can rid the sinus disease by managing the infectious source, the adenoids.
A foreign body within the nose should be considered, especially in the pediatric patient, as well as a patient who may have an emotional or mental disorder or who is institutionalized. A foreign body may obstruct the flow of secretions from the sinuses and create infection.
Substance abuse, especially of cocaine and marijuana, can alter the ciliary function of the nose and predispose to sinusitis. General active and passive cigarette smoke is part of exposure to substance abuse. Smoke is particulate matter inhaled and is an irritant to the respiratory tract, specifically the nasal and sinus ciliary function.
When there is unilateral sinus disease, it is important to have follow-up for the patient with repeated examinations and/or imaging to be sure that a neoplastic process is not the etiology. When unilateral sinus disease does not resolve, consider neoplasm and obtain proper imaging, nasal endoscopic examination, and biopsy as needed.
Although sinusitis is one of the most common disease entities, it has been poorly defined. The American Academy of Otolaryngology Head and Neck Surgery Paranasal Sinus Committee has attempted to define sinusitis.6 This committee agreed that as part of the description and definition of the disease, the term rhinosinusitis should now be used. In general, sinusitis does not occur without rhinitis, and rhinitis does not occur without sinusitis. This is similar to what occurs in the ear. Otologists understand that patients with acute otitis media will often have roentgenographic appearance of mastoiditis without a clinical mastoid infection. This is because of the communication between the middle ear and the mastoid air cells. The same is true in the nose and sinus with the interconnection between the spaces of the nasal sinus cavities. For this reason, rhinitis and sinusitis most often exist together, and therefore the term rhinosinusitis is appropriate.
Major and minor symptoms and signs of rhinosinusitis were defined by the committee and used as criteria to determine the diagnosis of rhinosinusitis. These criteria are symptoms and signs and are used to define five different types of rhinosinusitis: acute, recurrent acute, subacute, chronic, and acute exacerbation of chronic. From these criteria and definitions, a clinician should be able to diagnosis most cases of rhinosinusitis by history.
Major criteria associated with rhinosinusitis are facial pain and pressure, facial congestion and fullness, nasal obstruction, nasal discharge that is a purulent post-nasal drip, change in sense of smell, and purulence on nasal endoscopic examination. Minor criteria are headache, fever, halitosis, fatigue, dental pain, cough, ear pain, pressure, and fullness.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


