Diabetic Vitrectomy
Steven R. Sanislo
Mark S. Blumenkranz
Over 11 million Americans are estimated to have diabetes mellitus. Twenty-five percent of diabetic patients have diabetic retinopathy and 5% have severe nonproliferative diabetic retinopathy (NPDR) or proliferative diabetic retinopathy (PDR). In the United States, diabetic retinopathy is one of the leading causes of new cases of blindness and is the leading cause of blindness in working-aged Americans (25 to 74 years).1 Blindness is 25 times more common in diabetic patients than in those without diabetes.
History
In the last two decades, remarkable advances have occurred in the treatment of diabetic retinopathy. Pan-retinal laser photocoagulation has been shown to be effective in preventing the progression of most PDR and in reducing severe visual loss.2,3 Focal and grid laser photocoagulation also have been proven effective in reducing the risk of visual loss from clinically significant diabetic macular edema.4 Of 3,711 patients with mild to severe NPDR or early PDR enrolled in the Early Treatment Diabetic Retinopathy Study (ETDRS), vitrectomy was performed on 208 patients (5.6%).5 Twenty percent of vitrectomies were performed within 2 years of entering the study and 78% within 5 years. Most patients undergoing vitrectomy in the ETDRS had type I diabetes mellitus. The ETDRS showed that despite appropriate application of laser treatment, some patients, particularly those with type I diabetes mellitus, continue to develop progressive PDR with severe vision-threatening complications. In addition to these patients, others may present initially with proliferative complications for which laser photocoagulation cannot be applied. Vitrectomy is useful in preserving or restoring vision in many of these patients.
Machemer et al. first performed pars plana vitrectomy for the management of complications of diabetic retinopathy in 1970.6,7 Initially, diabetic vitrectomy was performed primarily to remove nonclearing vitreous hemorrhage. In 1975, Machemer described using vitrectomy techniques to remove preretinal proliferative membranes.8 Since then, indications for diabetic vitrectomy have increased to include the following: nonclearing vitreous hemorrhage, tractional retinal detachment, combined tractional and rhegmatogenous retinal detachment, progressive fibrovascular proliferation, and macular edema associated with posterior hyaloidal traction (Table 1). Vitrectomy is sometimes utilized to treat persistent diabetic macular edema in the absence of epiretinal membrane or obvious posterior hyaloidal traction, but this remains controversial. Increased indications for diabetic vitrectomy are primarily the result of significant advances in vitrectomy instrumentation and surgical techniques. Despite advances in our understanding of the pathophysiologic mechanisms of diabetic retinopathy and improvements in instrumentation and surgical techniques, patients with complications of diabetes mellitus remain among the most difficult patients to manage.
TABLE 1. Indications for Diabetic Vitrectomy | |
|---|---|
|
Surgical Principles
The surgical principles of diabetic vitrectomy include (a) removal of media opacities, (b) release of all traction on the retina, (c) application of laser endophotocoagulation when appropriate, and (d) use of retinal tamponade or scleral buckling when necessary. The first step in any diabetic vitrectomy is achieving adequate visualization of the retina by clearing media opacities. This may involve removal of a cataractous lens or removal of vitreous hemorrhage. Next, tractional membranes must be removed. It is desirable to remove all retinal traction, particularly around all retinal breaks, with complete separation of the posterior hyaloid. Pan-retinal photocoagulation should be performed if not already complete, and laser should be applied to surround any retinal breaks. Finally, if appropriate, retinal tamponade, scleral buckling, or both should be performed.
Instrumentation
The first instrument designed specifically for posterior vitrectomy was a single multipurpose instrument, the vitreous infusion suction cutter. Disadvantages of the vitreous infusion suction cutter included poor illumination, creation of large sclerotomies due to the size of the instrument, and difficulty manipulating the globe with a single instrument. In response to these problems, the standard three-port pars plana vitrectomy technique was developed. This technique uses single-purpose instruments: an infusion cannula; an endoillumination probe; and a vitreous cutter, forceps, or pic placed through three small sclerotomies. The main disadvantage of using single-purpose instruments is the necessity of removing and inserting instruments through the sclerotomies several times, which increases the risk of creating peripheral retinal breaks or retinal incarceration. Several cannula systems have been developed to address this problem. Recent trends in vitreous surgery include a return toward the use of multipurpose instruments (such as illuminated forceps, scissors, and pics), the advent of high-speed vitreous cutting instruments, and increasing use of sutureless transconjuctival vitrectomy. Multipurpose instruments may allow better tissue manipulation and help avoid iatrogenic retinal breaks. Many specialized instruments are available, including multifunction tissue manipulators, diamond blade cutting instruments, and membrane peeling cutter scissors. An overwhelming array of retinal forceps and pics are now available to choose from. Secondary illumination systems, such as illuminated infusion cannulas, have become available due to advances in the power of newer light sources. In difficult cases, illuminated infusion cannulas or chandelier illuminators can facilitate bimanual tissue manipulation. Contact and noncontact wide-angle viewing systems have improved visualization during vitrectomy, particularly for patients with small pupils, during pan-retinal photocoagulation and air–fluid exchange. Fiberoptic endolaser probes are used to apply pan-retinal photocoagulation, and indirect laser delivery devices can be used to complete the laser pattern to the ora serrata. Small-gauge transconjunctival sutureless 25- and 23-gauge vitrectomy systems have been developed and are gaining increasing acceptance for many cases of diabetic vitrectomy. Small-gauge vitrectomy can reduce surgical time and reduce surgically induced trauma in selected cases of diabetic vitrectomy. In cases with diabetic tractional retinal detachment, long-acting intraocular gas tamponade is often useful.9 The Silicone Oil Study Group has shown that intraocular gas tamponade with perfluoropropane is more effective than sulfur hexafluoride in treating severe forms of proliferative vitreoretinopathy.10,11 Perfluoropropane also may be preferable to sulfur hexafluoride in diabetic vitrectomy when retinal tamponade is necessary, but this has not been conclusively proven. Silicone oil sometimes is used for tamponade in cases of recurrent retinal detachment (issues regarding the use of silicone oil in diabetic vitrectomy are discussed later in this chapter). Although liquid perfluorocarbon is not used often in diabetic vitrectomy, it may be used to temporarily flatten the retina and delineate areas of persistent retinal traction.12
Standard Surgical Techniques
Anesthesia
Vitrectomy for complications of diabetic retinopathy can be performed with the patient under local or general anesthesia. The choice of anesthesia depends on the surgeon’s and patient’s preferences, the estimated duration of the procedure, and any systemic conditions that might place the patient at increased risk with general anesthesia. Local anesthesia offers the advantage of minimal disruption of the patient’s diabetic management, but may not be appropriate for long procedures or for patients who cannot remain immobile.
Removal of Vitreous Hemorrhage
If the vitreous hemorrhage is dense, preoperative ultrasonography is useful to delineate areas of retinal detachment and to ascertain whether a posterior vitreous detachment is present. After a core vitrectomy is performed, an opening in the posterior hyaloid is made with the vitrectomy probe. Subhyaloid hemorrhage then is aspirated with the probe or with a soft-tipped extrusion needle. Next, the posterior hyaloid and peripheral vitreous is removed. If no posterior vitreous detachment is present, one can be created by engaging the posterior vitreous over the optic disk or in the posterior pole adjacent to an area of proliferation, or the posterior hyaloid can be incised over an area of subhyaloid hemorrhage.
Membrane Dissection
Techniques for removal of epiretinal fibrovascular membranes have evolved over the past 10 years. Three techniques have been classically described: (a) segmentation, (b) delamination, and (c) “en bloc” dissection. Surgeons often use combinations and modifications of these techniques depending on the specifics of individual cases. Recently various adjuvants have been utilized to help identify and delimit the posterior hyaloids and epiretinal membranes.
Segmentation
Segmentation was the earliest method used to release retinal traction caused by preretinal fibrovascular proliferation. A core vitrectomy is first performed (Fig. 1A). Anteroposterior traction then is released by circumferentially cutting the posterior vitreous surface around the area of epiretinal proliferation (see Fig. 1B). After the anteroposterior traction has been released and the formed vitreous has been removed, the posterior vitreous surface is cut between epicenters of fibrovascular adhesion, which leaves islands of fibrovascular tissue. It also may be necessary to excise bridges of fibrovascular tissue connecting epicenters by using the vitrectomy probe or intraocular scissors (see Fig. 1C). Bleeding often is a problem during segmentation because the neovascular tissue is cut far away from its origin within the retina. Intraocular diathermy often is required to control bleeding from stumps of severed fibrovascular membranes. Raising the intraocular pressure also can be used temporarily to control intraoperative hemorrhage. Finally, pan-retinal endophotocoagulation is applied (see Fig. 1D).
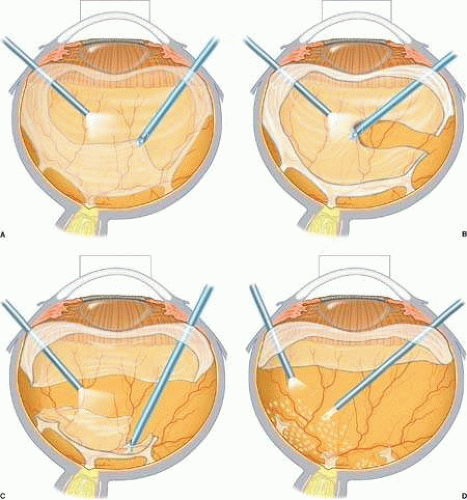 FIGURE 1. A. Core vitrectomy is performed. B. Peripheral vitreous is removed, releasing all anteroposterior traction on the epiretinal membrane. C. The epiretinal membrane is segmented by cutting bridging tissue between foci of fibrovascular adhesion. D. Segmentation has been completed, and pan-retinal endophotocoagulation is applied. |
Delamination
Delamination begins similarly to segmentation with the removal of the partially detached posterior vitreous surface between the vitreous base and the edge of the fibrovascular adhesions. Using bimanual techniques, from anterior to posterior, the edge of the fibrovascular membrane is reflected using either a lighted pick, lighted forceps, the light pipe, or a tissue manipulator (Fig. 2A). This allows the epicenters of adhesion between the retina and the fibrovascular membrane to be visualized. These epicenters then are amputated at the retinal surface using horizontal scissors, membrane peeling cutter scissors, or a diamond blade (see Fig. 2B). This technique is continued until all of the fibrovascular tissue has been removed up to the optic nerve head. The membrane then can be grasped with a forceps and gently avulsed (see Fig. 2C). Unlike segmentation, after the membrane dissection using the delamination technique, minimal or no epiretinal tissue remains on the retinal surface (see Fig. 2D). In cases with broad areas of severe vitreoretinal adhesion, a combination of delamination and segmentation may be necessary.
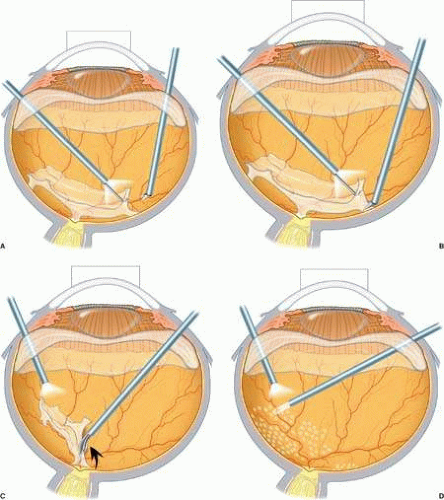 FIGURE 2. A. A lighted pic is used to elevate and reflect the edge of epiretinal tissue so that foci of fibrovascular adhesion can be visualized. B. Horizontal scissors are used to amputate the fibrovascular adhesion at the retinal surface. C. After the epiretinal membrane has been dissected up to the optic nerve, forceps are used to grasp the membrane and gently avulse it from the optic nerve head. D. The epiretinal membrane has been completely removed, and pan-retinal endophotocoagulation is applied. |
“En Bloc” Vitrectomy and Membrane Excision
The en bloc technique uses the anteroposterior traction of the vitreous to elevate the edge of the fibrovascular membrane, thus serving as a “third hand.” Removal of the formed vitreous is delayed until the end of the membrane removal. Initially, the vitrectomy cutter is used to create a tunnel through the formed vitreous from the sclerotomy site to an area of vitreoretinal separation (Fig. 3A). Any subhyaloid blood then is removed through this opening. The remaining posterior vitreous surface is left attached and assists in visualizing epicenters of adhesion between fibrovascular tissue and the retina (see Fig. 3B). An illuminated pick may be used to further elevate the fibrovascular tissue, and horizontal scissors are used to amputate epicenters of fibrovascular vitreoretinal adhesion (see Fig. 3C). Hemorrhage may occur when these epicenters are cut, but because the vessels are cut close to their origin, the bleeding usually is minimal and stops spontaneously. After the posterior vitreous surface and the entire fibrovascular membrane are freed from the retina, they are removed using the vitrectomy probe (see Fig. 3D). The main disadvantage of this technique is an increased risk of iatrogenic peripheral retinal breaks caused by traction at the vitreous base, which may occur in up to 35% of cases.13 If peripheral retinal breaks occur, they are treated with laser photocoagulation and a long-acting intraocular gas tamponade, with or without scleral buckling, depending on break location and surgeon preference.
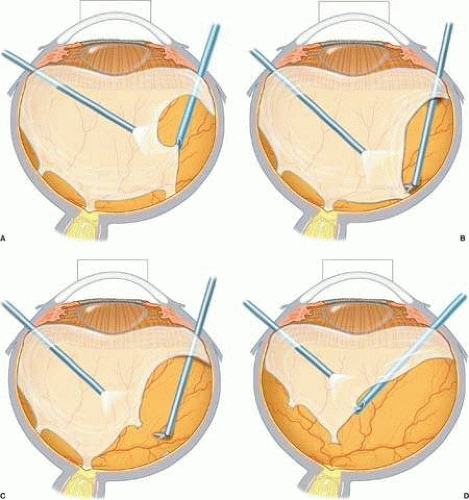 FIGURE 3. A. The vitrectomy cutter is used to create a tunnel through the formed vitreous to an area of vitreoretinal separation. B. The remaining posterior vitreous exerts traction on the epiretinal membrane, assisting in visualization of epicenters of adhesion. C. Horizontal scissors are used to amputate the fibrovascular adhesion at the retinal surface. D. The posterior vitreous surface and the entire fibrovascular membrane have been freed from the retina and are removed using the vitrectomy probe. |
Membrane Avulsion from the Optic Nerve
Using the delamination or en bloc technique, the fibrovascular membrane can be dissected from the retina up to the optic nerve head. At this point, the membrane can be avulsed from the optic nerve. Alternatively, the membrane can be trimmed close to the nerve and the remaining stump of tissue treated with diathermy. Avulsing the tissue assures that no traction persists. Bleeding often occurs when the tissue is avulsed, but usually it is limited and ceases spontaneously.14 Disadvantages of leaving tissue attached to the optic nerve include the possibility of persistent or recurrent retinal traction or inadvertent trauma to the optic nerve from diathermy.
Modified Delamination
As mentioned previously, the development of high-speed cutters has improved safety by reducing traction exerted by the cutting instrument on the retina when cutting close to the retinal surface. This allows the surgeon to perform vitreous “shaving” to remove residual anterior vitreous near the vitreous base and to more easily remove epiretinal fibrovascular tissue from the retinal surface. Previously cutting speeds typically used were in the range of 400 to 600 cuts per minute, whereas current technology allows cutting speeds of 1,200 to 2,400 cuts per minute. High-speed cutters have made possible a modification of delamination where nearly complete removal of all fibrovascular tissue is possible without the use of scissors or blades. In this technique, fibrovascular membranes are first segmented with the vitrectomy cutter between epicenters of epiretinal proliferation (Figure 4A). Next the remaining proliferative tissue is removed up to the epicenter. Finally, the high-speed vitreous cutter is used to shave the remaining tissue from the retinal surface (Figure 4B). Diathermy is often needed to coagulate the epicenters that have been shaved. Using this technique a nearly complete removal of proliferative membranes can be achieved without the risk of inadvertent retinal damage from sharp blades or scissors.
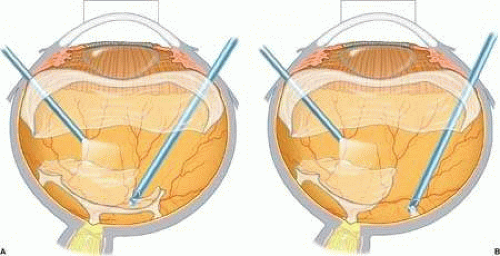 FIGURE 4. A. The vitrectomy cutter is used to segment islands of fibrovascular epiretinal membranes. B. The remaining stump of tissue is trimmed flush to the retinal surface using the high-speed cutter. |
Transconjunctival Sutureless Vitrectomy
The development of smaller instruments and specialized cannula systems has made possible sutureless transconjunctival pars plana vitrectomy. The most common systems use 25-gauge cannulas placed directly through the conjunctiva and sclera utilizing sharp trochars that are removed after placement of the cannulas. Larger 23-gauge transconjunctival vitrectomy systems have also been developed. Specially designed instruments that fit through these small cannulas include illumination and endolaser probes, microforceps and scissors, retinal pics, soft-tipped cannulas, and infusion cannulas. The main advantages of transconjunctival sutureless vitrectomy are the time savings during the surgery and reduced postoperative recovery time. Disadvantages include difficulty in manipulating the eye due to the small size and flexibility of the instruments and a limited choice of instruments that will fit through the cannulas. Initially a lack of instruments small enough to fit through 25-gauge cannulas severely limited the use of this technology in diabetic vitrectomies. Now, however, most instruments commonly used in diabetic vitrectomy are available in 25 gauge. This has led to a rapid increase in the use of small-gauge instrumentation. Other potential disadvantages of sutureless vitrectomy might include an increased risk of iatrogenic retinal tears associated with vitreous incarceration in the sclerotomies due to incomplete anterior vitreous removal and a possible increased risk of postoperative endophthalmitis due to sclerotomy wound leaks. In general, 25-gauge vitrectomy is most applicable for less complicated diabetic vitrectomies, whereas traditional 20-gauge vitrectomy techniques are generally recommended for more complicated cases such as those involving extensive epiretinal proliferation, combined traction/rhegmatogenous detachment, or combined PDR/proliferative vitreoretinopathy.
Primary Indications for Vitreoretinal Surgery
Indications for vitreoretinal surgery for complications of diabetic retinopathy have evolved over the last 20 years. The proportion of patients with nonclearing vitreous hemorrhage as the primary indication has decreased as more surgery is performed for other indications (see Table 1).
Nonclearing Vitreous Hemorrhage
Nonclearing vitreous hemorrhage is the earliest indication for vitrectomy in diabetic patients and generally is the least complex. Although its prevalence has decreased with extensive use of pan-retinal photocoagulation, it remains a common indication for diabetic vitrectomy.15 In the Diabetic Retinopathy Vitrectomy Study, eyes with severe, nonclearing vitreous hemorrhage of 1 to 6 months’ duration were randomized to immediate vitrectomy versus deferral of vitrectomy for 1 year.16 The percentage of patients with visual acuity of 10/20 or better was higher in the early vitrectomy group than in the deferral group throughout the 4-year follow-up period. However, until the 18-month follow-up visit, the early vitrectomy group had a higher percentage of eyes with loss of light perception. This was undoubtedly related in part to the unavailability of argon laser endophotocoagulation. An increased chance of obtaining good vision was clearly observed for early vitrectomy in patients with type I diabetes. However, this finding was not seen in patients with type II diabetes. The main advantages of early vitrectomy include a higher likelihood of recovering useful vision and earlier recovery of vision in successful cases. For individual patients, the exact timing of vitrectomy for nonclearing vitreous hemorrhage must take into account not only the duration of hemorrhage, but also the type and duration of diabetes, the severity of retinopathy (if known), and the status of the fellow eye.
Thompson et al. evaluated the results of 353 vitrectomies for nonclearing diabetic vitreous hemorrhage.17 Eighty-one percent of eyes had improved visual acuity on final examination. The percentage of eyes with a final visual acuity of 20/100 or better was 48%, and the percentage with a final visual acuity of 5/200 or better was 81%. Preoperative factors associated with a favorable visual prognosis included the following: preoperative visual acuity of 5/200 or better, absence of iris neovascularization or neovascular glaucoma, minimal cataract, and pan-retinal photocoagulation of at least one fourth of the fundus.
Macular Traction Retinal Detachment
The pathogenesis of diabetic traction retinal detachment involves interaction between the posterior hyaloid surface, preretinal fibrovascular proliferation, and the retina. Epiretinal fibrovascular tissue grows along the posterior surface of the vitreous gel. As the fibrovascular tissue contracts, the posterior hyaloid becomes taut and partially separates from the retina. Anteroposterior traction on the remaining areas of vitreoretinal attachment causes tractional retinal detachment (Fig. 5). Traction retinal detachments are separated into those where the macula is detached and those where the traction detachment does not involve the macula. Charles and Flinn studied the natural history of diabetic extramacular traction retinal detachment.18
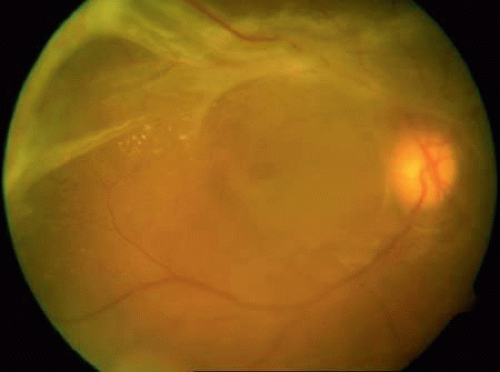 FIGURE 5. An example of an eye with PDR and traction retinal detachment involving the macula. |
They found a progression to macular detachment in only 13.8% of eyes at 1-year follow-up. Because most patients with extramacular traction retinal detachments do not progress to involve the macula vitrectomy is indicated only if there is macular heterotopia or vitreous hemorrhage precluding adequate pan-retinal laser photocoagulation (Fig. 6). In patients with traction macular detachment, surgery should not be deferred for an extended period of time, because retinal vascular changes may cause irreversible macular damage and reduce the potential for visual recovery.19 The results of vitrectomy for 360 eyes with diabetic traction retinal detachment of the macula were evaluated.20 Fifty-nine percent of eyes had improved visual acuity on final examination. The percentage of eyes with final visual acuity of 20/100 or better was 36%, and the percentage with a final visual acuity 5/200 or better was 72%. Preoperative factors associated with a favorable visual prognosis included the following: visual acuity of 5/200 or better, absence of iris neovascularization, minimal cataract, mild or no vitreous hemorrhage, pan-retinal photocoagulation of at least one fourth of the retina, and absence of severe retinal neovascular proliferation. Intraoperative factors associated with a worse visual prognosis included lensectomy, iatrogenic retinal breaks, and use of intraocular gas tamponade.
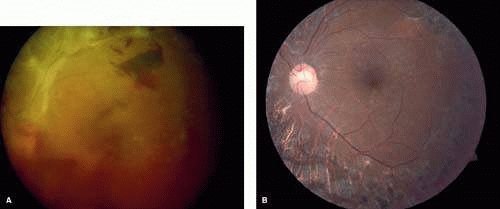 FIGURE 6. A. Preoperative fundus photograph of an eye with fibrovascular epiretinal membrane, traction retinal detachment, and nonclearing vitreous hemorrhage from severe PDR. B. Postoperative fundus photograph of the same eye after vitrectomy, membrane dissection (using delamination technique), and endolaser photocoagulation. |
Combined Traction-Rhegmatogenous Retinal Detachment
Vitreous traction and contraction of proliferative tissue can produce retinal tears that lead to combined traction-rhegmatogenous detachments. Unlike purely tractional detachments, extramacular rhegmatogenous detachments frequently progress to involve the macula, which leads to rapid and severe visual loss. Thus, surgical repair is indicated in combined detachments, whether or not the macula is involved. Often, the retinal breaks are located posterior to the equator, adjacent to areas of fibrovascular proliferation that are under severe vitreoretinal traction. Therefore, this condition is difficult to treat by conventional scleral buckling methods, whereas vitrectomy (with or without scleral buckling) is effective in treating this condition. Intraocular long-acting gas tamponade is required to treat these detachments. Combined traction-rhegmatogenous detachments have a lower success rate than pure tractional detachments or nonclearing vitreous hemorrhage. In an analysis of 172 eyes that underwent vitrectomy for combined traction-rhegmatogenous diabetic retinal detachment, 48% had an improved visual acuity upon final examination.21 A final visual acuity of 20/100 or better was achieved in only 25% of eyes, and a final visual acuity of 5/200 was achieved in 56%. Visual loss progressed to no light perception in 23% (compared with 19% for macular traction detachment and 6% for nonclearing vitreous hemorrhage). Preoperative factors associated with a favorable visual prognosis included visual acuity of 5/200 or better, absence of iris neovascularization, and absence of retinal detachment involving the macula. The only intraoperative factor found to be associated with a favorable visual prognosis was the absence of iatrogenic retinal breaks.
Progressive Active Fibrovascular Proliferation
In most patients with PDR, pan-retinal photocoagulation induces regression of retinal and optic disc neovascularization. In some patients, however, fibrovascular proliferation progresses despite full pan-retinal photocoagulation treatment. The importance of vitreoretinal contact in the development of neovascular proliferation has been recognized since 1965.22 When the vitreous gel is removed, the proliferative process tends to stabilize. It is rare for neovascularization of the disc or posterior fundus to occur in eyes that have undergone complete vitrectomy. Because the natural history for eyes with severe fibrovascular proliferation is poor, the Diabetic Retinopathy Vitrectomy Study evaluated the role of vitrectomy in eyes with extensive, active neovascular or fibrovascular proliferation, and useful vision (better than 10/200).23 Forty-four percent of eyes in the early vitrectomy group achieved a visual acuity of 10/20 or better as compared with 28% for the conventional management group. The greatest benefit was observed for eyes with severe fibrous proliferation and moderately severe neovascularization. Thus, for eyes with active, progressive, fibrovascular proliferation despite maximal pan-retinal photocoagulation, vitrectomy should be considered. However, vitrectomy does not take the place of pan-retinal photocoagulation and should be reserved only for eyes where laser cannot be applied or where laser has failed to stabilize the neovascular proliferation.
Macular Edema Associated with Posterior Hyaloidal Traction
Although the ETDRS showed that focal macular photocoagulation is beneficial in the treatment of clinically significant diabetic macular edema, it has been observed that some patients with diabetic macular edema and a taut, thickened posterior hyaloid do not respond to macular photocoagulation. It has been hypothesized that vitreous traction may cause or exacerbate macular edema in these patients. Lewis et al. report the results of pars plana vitrectomy with separation of the posterior hyaloid in 10 eyes with diabetic macular edema and traction associated with a thickened and taut premacular posterior hyaloid.24 Preoperative fluorescein angiography showed a deep, diffuse pattern of leakage in the macula (Fig. 7). Nine of 10 eyes had previous macular photocoagulation, and only one of these eyes responded with a temporary decrease in macular edema. Postoperatively, vision improved in nine eyes, and macular edema resolved in eight eyes. Postoperative complications included vitreous hemorrhage, rhegmatogenous retinal detachment, cataract formation, and mild epimacular membrane (each occurring in one eye). Other studies also report visual improvement after vitrectomy and posterior hyaloid separation in such patients.25 Tachi and Ogino reported the results of pars plana vitrectomy with separation of the posterior hyaloid in 58 eyes with diffuse diabetic macular edema without posterior vitreous detachment.26 These patients differed from those in prior reports in that they did not manifest a taut, thickened posterior hyaloid; therefore, it is not clear whether the posterior hyaloid was responsible for the macular edema. Although these patients showed an improvement in macular edema and visual acuity, this study was not controlled and was of limited follow-up. Thus, it is reasonable to consider vitrectomy and posterior hyaloid separation in patients with diffuse diabetic macular edema associated with a taut and thickened posterior hyaloid, whereas the long-term efficacy of such surgery in patients with diabetic macular edema without vitreoretinal interface abnormalities has not been conclusively proven. More recently some surgeons have proposed the use of vitrectomy with internal limiting membrane (ILM) peeling for patients with recalcitrant diabetic macular edema. At this time, studies of ILM peeling for diabetic macular edema remain somewhat limited and the benefit of such procedures remains controversial. Multiple authors have reported small series of patients with diffuse diabetic macular edema treated by vitrectomy with and without ILM peeling.27,28,29 Some have randomized to vitrectomy versus laser treatment.30,31 Although many of these studies have shown a reduction in macular thickness and macular volume after vitrectomy, most have found no significant difference in visual acuity outcome. Thus, at this time, more studies of vitrectomy for diabetic macular edema are needed to determine what role vitrectomy should play in patients with diffuse diabetic macular edema without a thickened posterior hyaloids or significant epiretinal membrane.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


