Diabetic Retinopathy
Brett J. Rosenblatt
William E. Benson
Clinical Findings
Diabetic retinopathy is usually divided into nonproliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR).
Early Nonproliferative Diabetic Retinopathy
Although microaneurysms are the first ophthalmoscopically detectable change in diabetic retinopathy, the earliest abnormalities seen histopathologically are thickening of the capillary basement membrane and pericyte dropout.1,2,3,4 Pericytes are mesothelial cells that surround and support the retinal capillary endothelium. Normally there is one pericyte per endothelial cell. In diabetes, however, the pericytes slowly decrease in number (Fig. 30.1). Their absence weakens the capillaries and permits thin-walled dilatations, called microaneurysms, to develop. Later, endothelial cells proliferate and lay down layers of basement membrane material. Fibrin may accumulate within the microaneurysm along with erythrocytes, and the lumen of the microaneurysm may become occluded (Fig. 30.2). Initially, most microaneurysms are on the venous side of the capillaries, but later they are seen on the arterial side as well. Clinically, they appear as small red dots (Fig. 30.3). Despite the multiple layers of basement membrane, microaneurysms are permeable to water and large molecules, allowing the transudation of fluid and lipid into the retina.
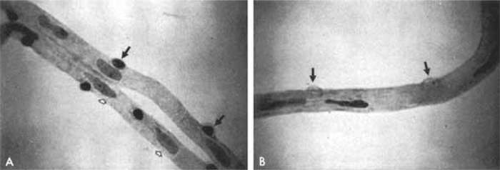 Figure 30.1. A. Trypsin digest preparation of early background retinopathy. Normal retinal capillaries, with one pericyte (closed arrows) per endothelial cell (open arrows). B. Retinal capillary of a patient with diabetes with necrotic pericytes (arrows). (Courtesy of Dr. Myron Yanoff.) |
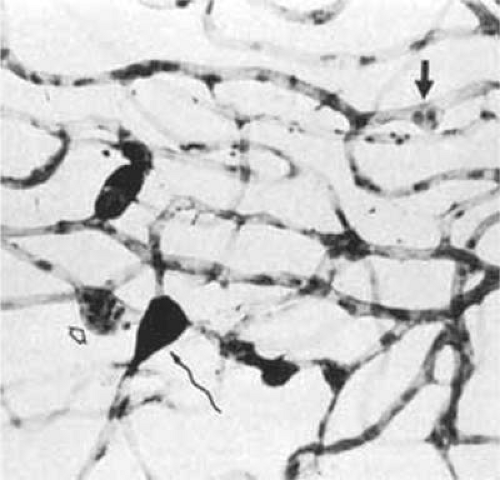 Figure 30.2. Trypsin digest preparation of early background retinopathy. Early microaneurysm (closed arrow), aneurysm with endothelial proliferation (open arrow), and aneurysm occluded with fibrin (curved arrow). (Courtesy of Dr. Myron Yanoff.) |
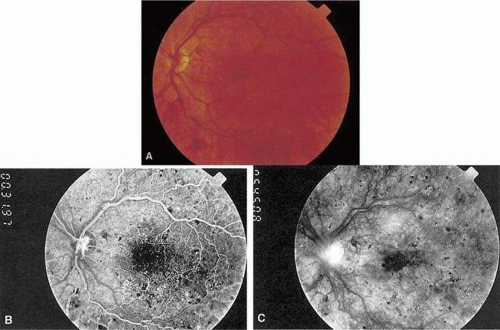 Figure 30.3. A. Diabetic retinopathy with multiple microaneurysms, dot hemorrhages, and early neovascularization of the optic disc (NVD). A small blot hemorrhage is seen inferiorly. B. Midphase of the fluorescein angiogram. Patent microaneurysms are seen as hyperfluorescent dots. Note that most microaneurysms cannot be seen ophthalmoscopically. There is some enlargement of the foveal avascular zone because of occluded capillaries. Temporally there is a larger zone of capillary nonperfusion. The NVD is beginning to leak. C. Late phase of the fluorescein angiogram showing diffuse leakage into the macula. |
It is often difficult to distinguish a small dot hemorrhage from a microaneurysm by ophthalmoscopy alone. On fluorescein angiography, patent microaneurysms will fill with dye quickly and then leak, unlike a small dot hemorrhage that will block fluorescence5 (Fig. 30.3). However, angiography cannot distinguish a hemorrhage from a microaneurysm filled with clotted blood. Because fluorescein passes easily though them, many more microaneurysms are seen on fluorescein angiography than are apparent on examination.6
When the wall of a capillary or microaneurysm is thin, it may rupture and form an intraretinal hemorrhage. If the hemorrhage is deep (i.e., in the inner nuclear layer or outer plexiform layer), it usually has a round or oval shape (“dot or blot”) (Fig. 30.3). Superficial nerve fiber layer hemorrhages are flame- or splinter-shaped, indistinguishable from that seen in hypertensive retinopathy. Although people with diabetes with normal blood pressure may have multiple splinter hemorrhages, they should nevertheless have their blood pressure checked because a frequent complication of diabetes is systemic hypertension.
Macular edema is an important manifestation of NPDR because it is the leading cause of legal blindness in patients with diabetes. The macular fluid arises from both leaking microaneurysms and diffuse capillary leakage. It separates retinal cells, causing multiple intraretinal interfaces that scatter light, decreasing the retina’s normal translucency and blurring the normal retinal pigment epithelial and choroidal background pattern (Figs. 30.3, 30.4, and 30.5). Clinically, macular edema is detected by biomicroscopy with a contact or handheld lens. Optical coherence tomography (OCT) is a diagnostic tool that accurately defines macular thickness and detailed surface and cross-sectional anatomy (Fig. 30.5). In severe cases of edema, the pockets of fluid in the outer plexiform layer are large enough to be seen. This is called cystoid macular edema (CME) (Fig. 30.6). Usually CME is seen in eyes with other signs of severe NPDR such as numerous hemorrhages or hard exudates, but in rare cases, generalized diffuse leakage from the entire capillary network can result in CME with few other signs of diabetic retinopathy.7
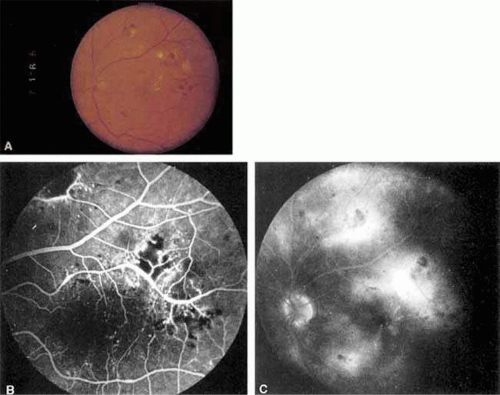 Figure 30.4. A. Exudates surround an area of hypoperfused retina. Note soft exudate superiorly. The macular edema thickens the retina and obscures the normal choroidal appearance. B. In the center of the hard exudates, the fluorescein angiogram shows capillary nonperfusion surrounded by microaneurysms. C. The late phase of the angiogram shows leakage into the retina. |
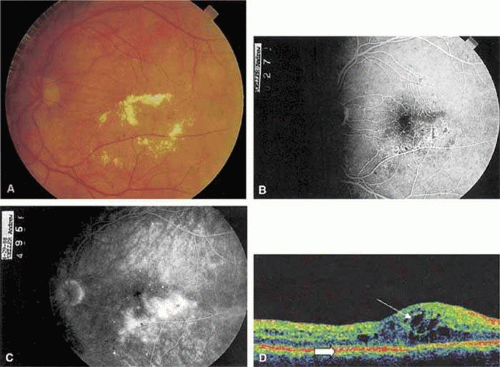 Figure 30.5. A. Circinate retinopathy inferotemporal to the center of the macula. B. The midphase of the fluorescein angiogram shows a cluster of microaneurysms in the center of the circinate ring. C. The late phase of the angiogram shows leakage of fluorescein. D. Optical coherence tomogram centered on the fovea of an eye with diabetic macular edema. The area of marked retina thickening contains numerous hyporeflective cystoid spaces (thin arrow). The outer retina is limited by the hyperreflective pigment epithelial band (thick arrow). |
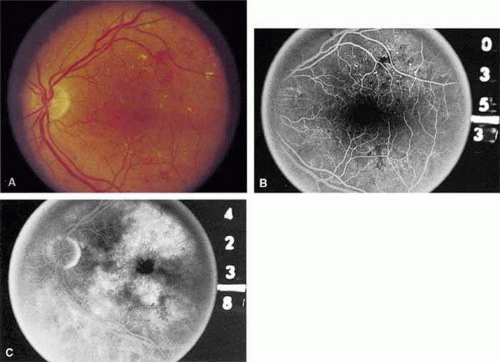 Figure 30.6. A. Background diabetic retinopathy. B. The midphase of the fluorescein angiogram shows multiple microaneurysms. C. Late phase of the angiogram shows cystoid macular edema. |
If the leakage of fluid is severe, lipid may accumulate within the retina (Figs. 30.4 and 30.5). Again, the outer plexiform layer is first to be affected. In some cases, lipid is scattered throughout the macula; in others, it accumulates in a ring around a group of leaking microaneurysms or around areas of capillary nonperfusion (Figs. 30.4 and 30.5). This ring pattern is referred to as circinate retinopathy.
In addition to the retinal vascular abnormalities, the choriocapillaris may be involved in NPDR. Initially there is a thickening of the basement membrane.8. Later, a periodic acid–Schiff (PAS)–positive material accumulates, which impinges on and may occlude the lumen of the choroidal capillaries in the posterior pole.4
Advanced Nonproliferative Diabetic Retinopathy
In advanced NPDR, signs of increasing retinal hypoxia appear, including multiple retinal hemorrhages, cotton-wool spots, venous beading and loops, intraretinal microvascular abnormalities (IRMA), and large areas of capillary nonperfusion (Figs. 30.7 and 30.8). Cotton-wool spots, previously called “soft exudates,” are nerve fiber layer infarctions. They are white, fluffy-appearing lesions of the nerve fiber layer that result from occlusion of precapillary arterioles. Fluorescein angiography confirms the lack of capillary perfusion. Microaneurysms frequently surround older cotton-wool spots as well as larger areas of capillary nonperfusion.
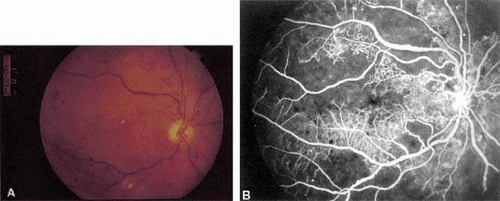 Figure 30.7. A. Severe nonproliferative retinopathy with venous dilatation and beading, cotton-wool spots, and intraretinal microvascular abnormalities. B. The midphase of the angiogram shows the intraretinal microvascular abnormalities (IRMA) and severe capillary nonperfusion. |
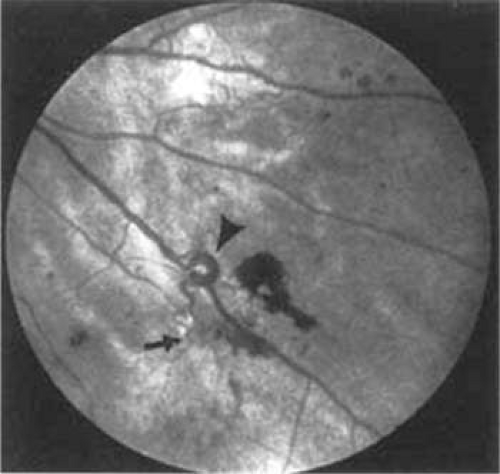 Figure 30.8. Venous loop (large arrow) and intraretinal microvascular abnormalities (IRMA; small arrow). |
Venous beading (Fig. 30.7) and venous loops (Fig. 30.8) indicate sluggish retinal circulation and are nearly always adjacent to extensive areas of capillary nonperfusion. Focal vitreous traction is thought to contribute to their formation.9 Dilated capillaries next to areas of nonperfusion that function as collaterals are referred to as IRMA. They may be difficult to differentiate from surface retinal neovascularization. Fluorescein, however, does not leak from IRMA but leaks profusely from neovascularization (Fig. 30.7). The Early Treatment Diabetic Retinopathy Study (ETDRS) found that IRMA, multiple retinal hemorrhages, venous beading and loops, widespread capillary nonperfusion, and widespread leakage on fluorescein angiography are all significant risk factors for progression to proliferative retinopathy (10). Interestingly, cotton-wool spots, in the absence of the other findings, are not. Approximately 50% of patients with severe NPDR progress to proliferative retinopathy with high-risk characteristics within 1 year.11
Proliferative Diabetic Retinopathy
Proliferative vessels usually arise from veins and often begin as a collection of fine vessels. When they arise on or within one disc diameter of the optic nerve they are referred to as neovascularization of the disc (NVD) (Fig. 30.9). When they arise further than one disc diameter away, they are called neovascularization elsewhere (NVE) (Fig. 30.10). NVE usually grows toward and into zones of retinal capillary nonperfusion, but capillary nonperfusion is nearly always more widespread in eyes with NVD than it is in NVE.12 Interestingly, it is seen more often in patients younger than forty years compared to older patients with diabetes.13
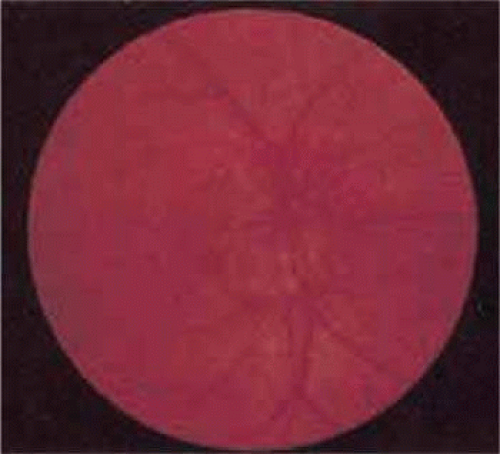 Figure 30.9. Advanced neovascularization of the disc. |
 Figure 30.10. Neovascularization elsewhere (NVE). |
Once the stimulus for growth of new vessels is present, the vessels grow along a path of least resistance. The absence of the internal limiting membrane over the optic disc could explain the proclivity of new vessel growth at that location. Neovascularization grows readily along connective tissue scaffolding such as the posterior hyaloidal face (Fig. 30.11).
 Figure 30.11. Autopsy eye. Neovascular stalk adherent to and growing on the posterior cortical vitreous, which has partially detached. (Courtesy of Dr. Myron Yanoff.) |
As PDR progresses, the new vessels become increasingly associated with fibrotic tissue. Fibrosis can become predominate or the neovascularization can remain primarily vascular. The vascular variety is usually found in association with vessels extending into the vitreous cavity or with abnormal new vessels on the surface of the retina. The avascular, fibrotic variety usually results from organization or thickening of the posterior hyaloid face.
Posterior vitreous detachment in diabetics is characterized by a slow, overall shrinkage of the entire formed vitreous rather than by the formation of cavities caused by vitreous syneresis.14 The contracting vitreous has a significant role in the production of vitreous hemorrhage, retinal breaks, and retinal detachment.15 Neovascular vessels do not “grow” forward into the vitreous cavity; they are pulled into it by the contracting vitreous to which they are adherent (Fig. 30.11). Vitrectomized eyes rarely develop new areas of neovascularization, and existent neovascularization tends to regress. In severe cases, posterior vitreous separation may result in retinoschisis, retinal detachment, and retinal break formation. In eyes fortunate enough not to develop these complications, the neovascularization may burn out, leading to atrophy of the new vessels.
An additional complication of contracting vitreous is traction involving the optic nerve that causes stria of the macula or even macular heterotopia12; both may cause decreased visual acuity.16
Although the macular edema, exudates, and capillary occlusions seen in NPDR often cause legal blindness, affected patients usually maintain at least ambulatory vision. PDR, on the other hand, often results in severe vitreous hemorrhage or retinal detachment with hand-movements vision or worse. It has long been assumed that sudden vitreous contractions tear the fragile new vessels, causing vitreous hemorrhage. Approximately three quarters of diabetic vitreous hemorrhages occur during sleep, possibly because of an increase in blood pressure secondary to early morning hypoglycemia or to rapid eye movement (REM) sleep.17,20 Because so few hemorrhages occur during exercise, it may not be necessary to restrict the activity of patients with proliferative retinopathy. The location of the hemorrhage is important in predicting whether it will clear on its own. If blood is behind the posterior vitreous face, it is likely to settle to the bottom of the eye and be absorbed. However, when hemorrhage breaks into formed vitreous it is less likely to clear spontaneously.
A large superficial hemorrhage may separate the internal limiting membrane from the rest of the retina. Such hemorrhages usually are round or oval but may also be boat shaped (Fig. 30.12). The blood may remain confined between the internal limiting membrane and the underlying retina for weeks or months before breaking into the vitreous. Subinternal limiting membrane hemorrhages were formerly thought to lie between the internal limiting membrane and the cortical vitreous and were called subhyaloid or preretinal hemorrhages. It is now felt that true subhyaloid hemorrhages are probably quite rare. Tight subinternal limiting membrane hemorrhages are dangerous because they may progress to traction retinal detachment.18,1918,19
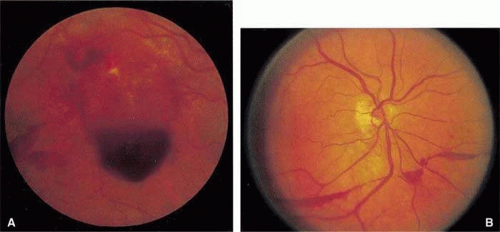 Figure 30.12. Subinternal limiting membrane hemorrhages. |
Two types of diabetic retinal detachments occur, those that are caused by traction alone (Fig. 30.13), and those caused by traction and secondary retinal breaks (Figs. 30.14 and 30.15). Characteristics of nonrhegmatogenous traction detachments in PDR include the following: (a) The detached retina is usually confined to the posterior fundus and infrequently extends more than two thirds of the distance to the equator, (b) it has a taut and shiny surface, (c) it is concave toward the pupil, and (d) there is no movement of subretinal fluid.
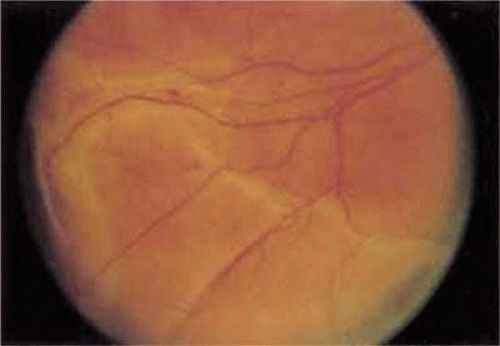 Figure 30.13. Traction retinal detachment. The detached retina has a smooth noncorrugated appearance and is convex toward the pupil. |
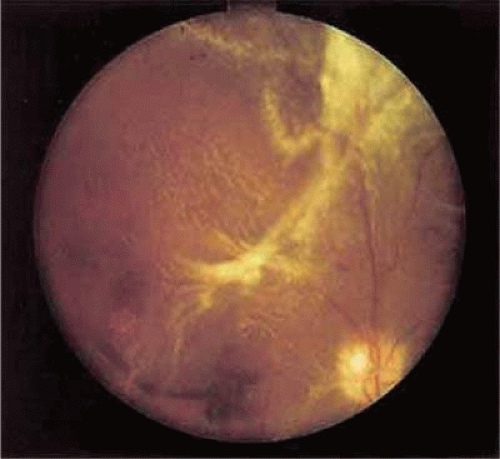 Figure 30.14. Combined traction/rhegmatogenous retinal detachment. The detached retina has a corrugated appearance and is concave toward the pupil. |
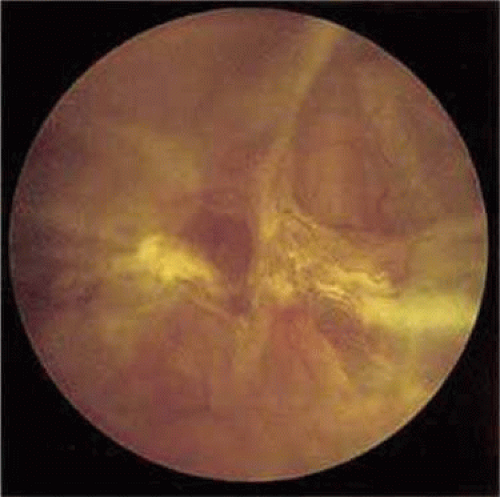 Figure 30.15. Round hole near fibrous proliferation. |
Vitreous traction may also cause focal areas of retinoschisis that may be difficult to distinguish from full-thickness traction retinal detachment. In retinoschisis, the elevated layer is thinner and more translucent (Fig. 30.16). In combined traction/rhegmatogenous detachment, the borders of the elevated retina usually extend to the ora serrata; the retinal surface is dull and grayish and undulates because of mobile subretinal fluid. The causative retinal breaks are usually found in the posterior pole near areas of fibrovascular proliferation. The breaks are oval and appear to be the result of tangential traction from the proliferative tissue as well as vitreous traction. Determining the location of retinal holes may be complicated by many factors, particularly poor dilation of the pupil, lens opacity, increased vitreous turbidity, vitreous hemorrhage, intraretinal hemorrhage, and obscuration of the breaks by overlying proliferative tissue. Often they are located only during surgery.
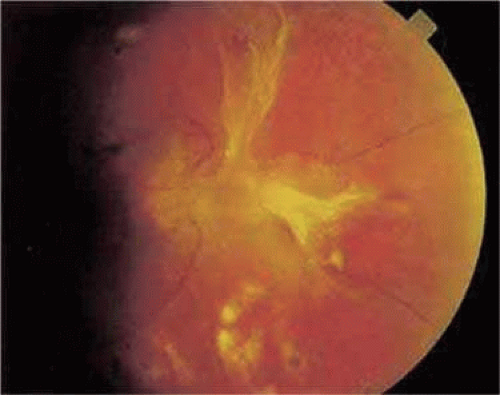 Figure 30.16. Traction retinoschisis nasal to the disc (Stereo). There is a small inner wall hole along the vessel that leaves the disc at the 2 o’clock position. |
Risk Factors of Diabetic Retinopathy
Duration of Diabetes
The best predictor of diabetic retinopathy is the duration of the disease.21,22,23,24 Patients who have had type 1 or insulin-dependent diabetes mellitus (IDDM) for 5 years or less rarely show any evidence of diabetic retinopathy.24,25 However, 27% of those who have had diabetes for 5 to 10 years and 71% to 90% of those who have had diabetes for longer than 10 years have diabetic retinopathy.30 After 20 to 30 years, the incidence rises to 95% and approximately one third to one half of these patients have PDR.25
Determining the role of duration of diabetes as a predictor of retinopathy in type 2 or insulin-resistant diabetes mellitus is more difficult because of the uncertainty of the onset in many patients. In some, the diagnosis of diabetes is made only after retinopathy is discovered. Yanko et al.26 found that the prevalence of nonproliferative retinopathy 11 to 13 years after the onset of type 2 diabetes was 23%. After 16 or more years, it was 60%. Eleven or more years after the onset, 3% of the patients had proliferative retinopathy. Klein24 found that 10 years after the diagnosis of type 2 diabetes, 67% of patients had retinopathy and 10% had PDR. The risk was lowest in patients who did not require insulin.
Age of the Patient
Although the duration of diabetes is the most important determinant of retinopathy, the years that a patient has diabetes before the onset of puberty do not count against him or her. In other words, the risk of retinopathy is roughly the same in two 25-year-old patients, one of whom developed type 1 at the age of 6 years and the other of whom developed it at age 12 years.21
Systemic Factors
Control of Blood Glucose
The decades-old controversy regarding whether or not intensive metabolic control prevents the development or progression of retinopathy was finally laid to rest by the Diabetes Control and Complications Trial (DCCT) and the United Kingdom Prospective Diabetes Study (UKPDS).27,28,29,30,31 In the DCCT, patients who closely monitored their blood glucose and who were treated with insulin at least three times per day by injection or by insulin pump were compared to patients treated with conventional therapy. The intensive-treatment group had a 76% reduction in the rate of development of any retinopathy and an 80% reduction in progression of established retinopathy. Ophthalmologists must be aware that after institution of strict control, there is often an initial worsening of preproliferative retinopathy.32,33,34 Fortunately, after two years of control, the strict-control groups had the same or less retinopathy than groups treated conventionally.35 The UKPDS was a randomized, controlled clinical trial involving newly diagnosed type 2 diabetes. Patients were randomly assigned to intensive glycemic control with sulfonylurea agents or insulin or to conventional control with diet. After 12 years of follow-up, progression of retinopathy in the intensive-control group was reduced by 21%.30
The benefits of rigorous control of blood glucose do not extend to all eyes with advanced retinopathy. Even patients who are made normoglycemic by pancreatic transplantation continue to show progression.36
Renal Disease
Most patients with renal disease, as evidenced by proteinuria, elevated blood urea nitrogen (BUN), and elevated blood creatinine, also have retinopathy.37,38,39,40,41,42 Even patients with microalbuminuria are at high risk of having retinopathy.38,39,40,41,42 On the other hand, only 35% of patients with symptomatic retinopathy have proteinuria, elevated BUN, or elevated creatinine.43
Systemic Hypertension
The Hypertension in Diabetes Study (HDS), part of the UKPDS, evaluated the effect of blood pressure control on the progression of diabetic retinopathy. Patients who were kept under strict control of blood pressure (<150/85 mm Hg) had a 34% risk reduction in microvascular changes compared to the conventional blood pressure control group (<180/105).44 For every 10-mm Hg reduction in systolic blood pressure, there was an associated 13% reduction of microvascular end points. It did not matter whether the blood pressure was controlled using a beta-blocker or angiotensin-converting enzyme inhibitor (ACEi).45 Lisinopril, an ACEi, has been shown in another study to decrease by 50% the progression of NPDR in normotensive type 1 diabetics; suggesting a benefit for some antihypertensives independent of the blood pressure lowering effect.46
Pregnancy
Women with diabetes who begin a pregnancy with no retinopathy have a 10% to 26% risk of developing some NPDR.47,48 Those who have NPDR at the onset of pregnancy and those who are anemic or hypertensive tend to show accelerated progression, with increased hemorrhages, cotton-wool spots, and macular edema.48,49,50 Fortunately, there is usually some regression of NPDR after delivery.51,52,53 Women who begin pregnancy with NPDR have a 22% to 40% incidence of progression to PDR.48,51,54 Those with untreated PDR at the onset frequently do poorly unless they are treated with aggressive panretinal photocoagulation (PRP), but those with previously treated PDR usually do well.55,56 Women who maintain good metabolic control during pregnancy have fewer spontaneous abortions and fewer children with birth defects.57 Therefore, obstetricians strive for optimal control. However, women who begin pregnancy with poorly controlled diabetes who are suddenly brought under strict control frequently have severe deterioration of their retinopathy and do not always recover after delivery.47,49,52,58 It may be best to gradually bring the blood glucose under control.
Race
Retinopathy is more likely to be present in blacks than in whites.59 Moreover, blacks have a higher rate of severe macular edema and of blindness, possibly because of a higher incidence of systemic hypertension.60 Contrary to these findings, the study by Arfkin et al61 suggested that blacks had a slightly slower rate of progression than whites.
Cigarette Smoking
Cigarette smoking, because it increases blood carbon monoxide, platelet aggregation, and causes vasoconstriction, might be expected to accelerate diabetic retinopathy. However, a clear association of diabetic retinopathy severity or progression has not been clearly established in peer-reviewed literature.62,63
Serum Lipids
Elevated serum cholesterol is a strong predictor for the rate of visual loss. Patients with both elevated cholesterol and low-density lipoprotein (LDL) cholesterol are much more likely to have vision loss associated with hard exudates in the macula.64
Pathogenesis
The cause of diabetic retinopathy is clearly multifactorial; thus far no single pathologic mechanism has been identified. A clearer picture with important treatment implications is emerging.
Aldose Reductase
Aldose reductase is an enzyme that converts sugars, when present in high concentration, into alcohols. For example, glucose is converted to sorbitol and galactose is converted to dulcitol. Because sorbitol and dulcitol cannot easily diffuse out of cells, their intracellular concentration increases. Osmotic forces draw water into the cells resulting in electrolyte imbalance. The resultant damage to lens epithelial cells, which have a high concentration of aldose reductase, is responsible for the cataracts seen in children with galactosemia and in animals with experimental diabetes mellitus. Because aldose reductase is also found in high concentration in retinal pericytes and Schwann cells, some investigators suggest that diabetic retinopathy may be caused by aldose reductase–mediated damage.65,66 Strong support for this theory is that aldose reductase inhibitors reduce cataract formation,67 permeability of small vessels,68 and pericyte loss.69 Furthermore, they improve nerve conduction velocity,70,71 decrease pain from peripheral neuropathy,72 decrease proteinuria,73 and decrease vascular permeability.68,74
Protein Kinase C
Protein kinase C (PKC) is a group of enzymes that seem to play a role in diabetic microvascular complications. The PKC-beta isoform is activated by hyperglycemia, its activation has been shown experimentally to be associated with the breakdown of the blood-retinal barrier by activating vascular growth factors.79,80 Blocking PKC-beta has been shown to prevent intraocular neovascularization. There is enthusiasm that PKC-beta blockade will become an effective treatment for diabetic retinopathy. Ruboxistaurin, an orally administered PCK inhibitor, has been extensively studied. Although it showed a tendency to reduce vision loss and the need for laser, it has not been shown effective in treating macular edema.81,82
Vasoproliferative Factors
In 1954, Michaelson83 first proposed that hypoxic retina produces a “vasoproliferative factor” that diffuses to nearby blood vessels inducing neovascularization. There has long been evidence for this substance: First, neoplasms produce a diffusible substance, tumor angiogenic factor, that causes blood vessels from adjacent normal tissues to grow toward and into the tumor, thereby providing the tumor with oxygen and other nutrients. Second, in many conditions (e.g., branch retinal vein occlusion, sickle cell disease, Eales disease, and retinopathy of prematurity), ischemic areas of retina are adjacent to or near to areas of neovascularization, which tends to grow into the hypoxic area.84,85,86 Third, the development of neovascularization of the optic disc and iris, both of which can be reversed by PRP, argues for a diffusible factor. Vascular endothelial growth factor (VEGF) is clearly one of the more important of these diffusible substances that are implicated in the pathogenesis of microvasculopathies such as diabetic retinopathy. VEGF is found in the vitreous of patients with diabetic retinopathy and decreases after PRP.87,88,89 Furthermore, experimental intravitreal injections of VEGF produce retinal ischemia and microangiopathy in primates.90 Compounds that inhibit the action of VEGF block and reverse the formation of new blood vessels and decrease the permeability of capillary endothelium.
Growth Hormone
After Poulsen91 noted reversal of florid diabetic retinopathy in a woman who had postpartum hemorrhagic necrosis of the pituitary gland (Simmonds syndrome), growth hormone was suspected to play a causative or at least an important supportive role in the development and progression of diabetic vascular complications. In the 1950s and 1960s surgical pituitary ablation was considered by some to be an effective treatment for diabetic retinopathy. More recently, growth hormone deficiency was found to be somewhat protective against retinopathy.92
Platelets and Blood Viscosity
Several lines of evidence strongly suggest that platelet abnormalities in diabetics may contribute to retinopathy.93 There are three steps in platelet coagulation: initial adhesion, secretion, and further aggregation. Adhesion refers to the propensity of platelets, aided by von Willebrand factor (factor VIII) to stick to basement membrane, damaged endothelial cells, and collagen.94 It has been shown that the platelets in diabetic patients are “stickier” than platelets of patients without diabetes.95
Once platelets adhere to the basement membrane or to damaged cell walls, they secrete prostaglandins that cause other platelets to adhere to them (aggregation) (Fig. 30.17). This initiates the production of thromboxane A2 and ADP, which promote increased platelet aggregation. Diabetic platelets are especially sensitive to thromboxane and to other aggregating agents.95,96 It has been postulated that abnormal platelet adhesion and aggregation causes focal capillary occlusion and focal areas of ischemia in the retina, which in turn contribute to the development of diabetic retinopathy.93 However, it should be mentioned that PDR has been reported in patients with severe platelet dysfunction.97
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


