Skin Resurfacing-Laser or Peel
CHAPTER 30
The demand for facial skin rejuvenation has seen unprecedented growth in recent times. The explosion of interest in facial skin resurfacing by the public has paralleled that on the part of the cosmetic surgeon. As newer technologies have become available, the cosmetic surgeon’s armamentarium for treating aged and actinically damaged facial skin has blossomed. While the media continue to bombard the public with the latest therapies, and as we address better informed, Internet-saavy patients, facial plastic surgeons have a responsibility to be knowledgeable and to understand the advantages and disadvantages of the various types of facial skin resurfacing techniques.
Many options are available to physicians who treat patients interested in facial skin rejuvenation. The latest advances in technology have allowed physicians to treat many facial skin conditions with laser therapy. As laser technology continues to develop, many different types of lasers are becoming available. The recent debate, however, is whether the laser will supplant more traditional chemical peeling procedures. Chemical peeling agents have been used for many centuries. The contemporary use of these agents began during the 1960s, and their use has flourished. Well-documented research has shown the beneficial clinical and histologic changes present after the application of various chemical peeling agents. Similar findings have recently been shown after laser facial skin resurfacing.
Regardless of the modality used, success with these agents is based on many variables. Along with a thorough understanding of the chemical agent or laser, and its proper use by the operator, patient selection remains a crucial factor in determining a successful outcome. No single therapy can be used successfully for all patients or all skin conditions. Currently, we use both modalities in our practice and continue to do so for a variety of different problems to help our patients achieve optimal rejuvenation of their skin.
Background
Chemical peeling of the face has been performed for centuries. The ancient Egyptians used particles of alabaster mixed with milk and honey to abrade the skin in an attempt to tighten the facial skin. Substances including acids, minerals, sulfur, mustard, fire, sandpaperlike products, limestone, and plant substances have been used in an attempt to reduce facial rhytids and to reverse changes associated with photoaging.
During the early twentieth century, interest in skin revitalization again flourished as MacKee, a dermatologist, reported the use of phenol for the treatment of acne scars. Shortly after this discovery, in 1905, surgical planing, today known as dermabrasion, was pioneered by Kromayer. He is reported to have used rotating wheels and rasps for the treatment of keratoses, acne scars, and hyperpigmentation disorders. Kromayer observed that healing after skin resurfacing was related to the depth of injury created by surgical planing. He believed that when injury to the skin was restricted to the upper dermal layer, above the adnexal structures, subsequent healing would occur without scarring.
Interest in surgical planning grew after World War II as many attempts were made to improve traumatic tatoo injuries sustained during the war. Throughout the 1940s and 1950s, the medical literature became replete with descriptions related to the uses of dermabrasion. During this period, chemical peeling did not receive the same attention from the medical community because it was not applicable to the treatment of war-related injuries. However, the lay public was extremely interested in chemical peeling, as the media reported that the “fountain of youth”; had been discovered.
Most operators performing chemical peels were not physicians. It was not until the late 1950s and early 1960s that plastic surgeons and dermatologists undertook scientific investigations of phenol and trichloroacetic (TCA) acids peels for their use in facial skin resurfacing. It was not until 1972, when Baker demonstrated to a group of plastic surgeons the beneficial results he had achieved using phenol, that facial skin resurfacing became widely accepted in the medical community.
Histologic Effects of Photoaging and Skin Resurfacing
Most patients seeking evaluation for skin rejuvenation have a history of significant sun exposure. Clinical signs of actinic damage include the development of coarse rhytids, rougher skin texture, pigmentary mottling, and the development of solar lentigines and actinic keratoses. Histologically, changes in the epidermis and dermis of patients with sun-damaged skin develop as well. Epidermal dysplasia occurs, indicated by thickened epidermis and the appearance of dysplastic cells. Clinically, this finding corresponds to the development of actinic keratoses and may lead to the development of basal or squamous cell carcinomas. In addition, epidermal hyperplasia and epidermal atrophy are observed in combination with irregular pigment distribution and solar lentigines. In the dermis, dermoelastosis, the degeneration of collagen and elastic fibers, is the main diagnostic feature in sun-damaged skin. Intrinsically aged skin shows similar clinical and histologic changes, except that, in actinically damaged skin, these processes are accelerated.
Chemical peeling and laser resurfacing techniques reverse the damage created in the skin as a result of photoaging. The obliteration of many of the clinical and histologic changes varies depending on the depth of the wounding agent. Knowledge of histologic changes and the histologic effects of various peeling agents must be understood in order to obtain optimal results and prevent complications.
Patient Selection
INDICATIONS
As in all facial aesthetic procedures, proper patient selection with individualization of treatment is key to a successful outcome. Technical skill must be combined with proper selection of the right patient, to avoid devastating results. Chemical peeling and laser resurfacing have well-defined indications. These treatment modalities are not appropriate for all patients or all skin conditions. In general, patients with facial wrinkles and blotchy pigmentation are candidates for either type of procedure. Patients with actinic keratoses also benefit from resurfacing techniques, as the epidermal and dermal damage is reversed. It is our experience that patients with traumatic or acne scars are more likely to respond to CO2 laser resurfacing than to treatment with chemical peeling agents. Deeper scars may respond poorly to either of these skin resurfacing techniques.
Most patients seeking consultation for facial aging mistakenly believe that a facelift will repair their sun-damaged skin. When gravitational forces are part of the problem, surgical procedures are recommended. However, patients should understand that superficial or deep facial rhytids, pigmentary changes, and acne scarring are better treated with skin resurfacing. It is important to explore the patient’s goals and expectations regarding the procedures desired.
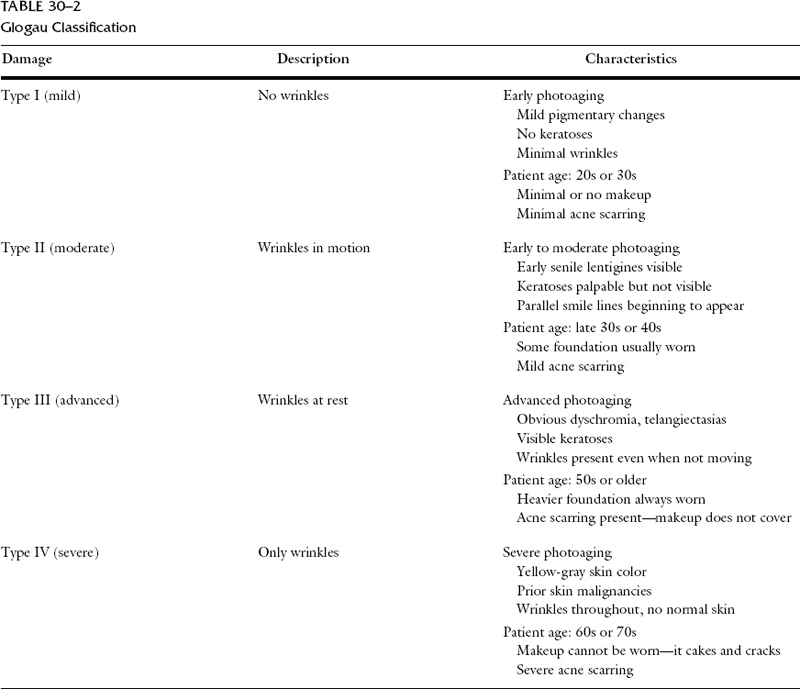
Patient assessment begins with the evaluation of skin type and complexion, skin texture and thickness, the degree of photoaging and severity of facial rhytids, and age-related gravitational changes. Skin type and complexion are the primary factors that help determine whether laser or chemical peeling agents should be considered to yield the best outcome. Other considerations include patient lifestyle and patient expectations. The morbidity associated with early sun exposure must be weighed against the desires and goals of the patient. We use the Fitzpatrick classification as a guide for evaluating skin types (Table 307-1). Skin types under this classification scheme correlate with the patient’s skin color and reaction to sun exposure. White skin that always burns is classified as Fitzpatrick type I, whereas black skin that never burns is classified as Fitzpatrick type VI. Another classification system, developed by Glogau, is more objective, but it is also very useful to help classify photoaged skin (Table 307-2).
The Fitzpatrick skin classification system is a simple guide that helps dictate which patients require pretreatment. Both patient and physician must realize that pretreatment with the use of a -hydroxy acids, retinoic acid, topical steroids, sun-screens, and bleaching agents may be a part of the pretreatment regimen. The patient’s skin thickness and texture also must be factored into the plan. As opposed to patients with thin, dry, atrophic skin, those with thicker, oily, sebaceous skin may require a more aggressive pretreatment regimen, including Retin-A and glycolic acids. These patients may also require multiple applications with the peeling agent, or multiple passes with the CO2 laser, to achieve a satisfactory result. Finally, the degree of pathology and the desire for improvement must be assessed. Superficial lentigines and fine rhytids may be treated satisfactorily with either medium-depth chemical peels or conservative CO2 or erbium laser resurfacing. Deeper, coarse, facial rhytids require phenol chemical peeling to achieve the optimal result.
| Type | Skin Color | Skin Characteristics |
| I | White | Always burns, never tans |
| II | White | Usually burns, tans less than average |
| III | White | Sometimes mild burn, tans about average |
| IV | White | Rarely burns, tans more than average |
| V | Brown | Rarely burns, tans profusely |
| VI | Black | Never burns, deeply pigmented |
Chemical Peels
Chemical peeling involves the application of chemical agents that act to accelerate the normal process of exfoliation. A variety of chemical agents are used to produce varying effects to the skin. Sloughing of the stratum corneum, produced by superficial chemical peeling, improves skin texture by stimulating the growth of a thicker epidermal layer. These peels are also effective for the treatment of superficial skin lesions. Medium-depth peeling agents produce injury to the papillary and upper reticular dermal layers by their chemical cauterant effect. This helps reverse the effects of photoaging, including the treatment of mild to moderate facial rhytids and pigmentary dyschromias. They are also performed for the removal of actinic keratoses. Deeper escharotic peeling agents act by destroying specific layers of skin, creating necrosis and inflammation in the epidermis, papillary dermis, and reticular dermis. The deeper peeling agents are indicated for the treatment of patients with significantly photoaged skin. Some chemicals may be used as superficial, medium, or deep peeling agents. A number of factors, including the concentration, the number of layers applied to the skin, and the duration of contact of the peeling agent with the skin, may affect the depth of the peel. Understanding the properties of these chemical agents is key to their successful use (Table 30-1).
| Depth | Agent |
| Superficial | Glycolicacid 50 to 70% applied for 5 to 15 min Jessner’s solution applied in 5 to 10 coats Resorcinol 50% applied for 30 to 60 min TCA 10 to 35% |
| Medium depth | Glycolic acid 70% applied 5 to 30 min TCA 35 to 50% applied alone or augmented with glycolic acid or Jessner’s solution |
| Deep | Phenol 88% Baker–Gordon phenol formula |
TRICHLOROACETIC ACID PEELS
TCA is perhaps the best single agent for skin resurfacing. It exhibits unique properties that afford the cosmetic surgeon tremendous flexibility and versatility in treating a variety of clinical conditions. When properly used, TCA has an overall decreased morbidity as compared with other agents. It allows patients to achieve a predictable result with the benefit of disrupting their lives to a lesser degree.
Indications
Although TCA is the most popular and most widely used chemical peeling agent, proper usage is imperative to a successful outcome. Ideal candidates for TCA peeling include patients with pigmentation disorders and those who exhibit early facial rhytids. Patients with severe actinic damage and those with coarse facial rhytids are better served by other methods.
Pretreatment
To achieve the most consistent and reliable results, pretreatment of facial skin is mandatory. This improves the ability of TCA to penetrate beyond the stratum corneum and deep to the epidermal-dermal junction in a more predictable manner. We feel that almost all patients should undergo prepeel treatment with a combination of 8% hydroquinone, 1% hydrocortisone, and 0.05% retinoic acid. This bleaching formula is prepared for us by a pharmacist. Hydroquinone affects melanocytic metabolism by increasing the degradation of melanin, while decreasing melanin formation. It acts specifically by inhibition of tyrosinase, a hormone responsible for increasing the proliferation of melanocytes. Retin-A acts synergistically by increasing the penetration of hydro-quinone. An absolute indication for pretreatment is any patient with Fitzpatrick type III skin or greater. After this pretreatment regimen, TCA peeling is more predictable. This combination helps ensure a peel of consistent penetration with a lower risk of postinflammatory hyperpigmentation. Our patients use these products once daily for at least 4 weeks before undergoing their peel. Other cosmetic surgeons recommend treatment for a 6-week period. Alternative pretreatment regimens include the use of glycolic acid products ranging within 10 to 14% concentration. Glycolic acid acts to thin the stratum corneum and enhance TCA penetration. When glycolic acids are used for pretreating the skin, they are frequently used in combination with hydroquinones.
Technique
As with all chemical peeling, the skin should be degreased with an acetone-soaked sponge. The mechanical abrasion helps remove the stratum corneum, helping produce uniform penetration of the peeling agent. TCA may be applied as a 10 to 50% concentration, depending on the desired depth of penetration. We strongly discourage the use of TCA in concentrations higher than 35% because of a significantly higher risk of undesirable side effects such as scarring and hypopigmentation. We routinely use a 35% TCA concentration after the application of Jessner’s solution. Jessner’s solution is a keratolytic agent that acts by removing the stratum corneum to permit deeper penetration of the TCA. Unlike other peeling agents, the penetration of the TCA peel is affected by the number of layers applied. The goal is to achieve uniform frosting of the treated skin. Generally, the whiter the frost, the deeper the TCA has penetrated. It is important to note that a change in the color of the frost, from white to gray, represents penetration deep into the reticular layer and may result in hypertrophic scarring. Jessner’s solution and 30% TCA can be used to treat actinic damage in the neck area.
Postpeel Care
Postpeel care may vary depending on the depth of the TCA peel. Patients undergoing superficial TCA peels are treated with occlusive agents such as bacitracin ointment, Eucerin cream, or Elta. These are applied 4 to 5 times per day by the patient for 3 to 5 days until reepithelialization has occurred. At this point, the patient may resume wearing makeup and is instructed to use a skin moisturizer. Patients undergoing deeper TCA peels are instructed to follow the same directions but should expect reepithelialization to occur several days later, usually between 5 and 7 days. It is imperative that patients be instructed to avoid sun exposure for 6 weeks after their peel.
Complications
Hyperpigmentation The most common complication of TCA peeling is postinflammatory hyperpigmentation, which is generally the result of early sun exposure. It must be stressed that during the early stages of healing, sun exposure is prohibited. In most patients in whom this complication develops, failure to comply with this instruction is the most common cause. Patients may also exhibit this complication if pretreatment was inadequate. Birth control pill intake should also cease during this peripeel period, as their use can produce pigmentary changes.
Hyperpigmentation is usually easy to treat and will respond to 0.05% Retin-A cream in combination with 8% hydroquinone. We prefer to use our bleaching formula as described previously. This is usually applied once or twice daily for about 3 weeks, but it may be used longer if necessary. Some patients may experience moderate erythema secondary to Retin-A use. This problem is less common in those who were treated with Retin-A during the prepeel period. However, should this be of concern, topical hydrocortisone may be used for several weeks as required. These patients are also instructed to use a sunscreen with a sun protection factor (SPF) of 20 or greater.
Hypertrophic Scarring
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


