Purpose
To present the surgical technique and the early clinical results of the EndoGlide, a graft insertion device for use during Descemet stripping automated endothelial keratoplasty (DSAEK).
Design
Prospective interventional case series.
Methods
patients: Graft insertion with the EndoGlide was performed in 25 eyes of Asian patients with endothelial dysfunction suitable for DSAEK. Demographic and clinical details, best-corrected visual acuity, postoperative complications, and endothelial cell density (ECD) loss were documented. surgical technique: The prepared graft is transferred onto a preparation base and pulled into the glide capsule with forceps. Drawing the graft into the capsule curls it into a “double-coil” configuration. The assembled EndoGlide is inserted into the eye, and the graft is pulled into the anterior chamber with forceps, where it uncoils in the correct orientation with minimal manipulation.
Results
Average age was 70 years (range 28-91) and the commonest diagnosis was pseudophakic bullous keratopathy (12 eyes). Preoperative donor ECD was 2957 ± 242 cells/mm 2 , median graft diameter was 8.75 mm, and all surgeries were completed successfully by 2 surgeons. There was a short learning curve in loading of the graft into the EndoGlide and in uncoiling the graft in the recipient eye. No patient had graft dislocation or primary iatrogenic graft failure. At 6 months, the mean ECD was 2586 ± 338 cells/mm 2 and mean cell loss was 13.1% in 20 eyes. At 12 months, the mean ECD was 2575 ± 289 cells/mm 2 and mean cell loss was 15.6% in 10 eyes.
Conclusions
Graft insertion with the EndoGlide is safe in DSAEK, with a short learning curve and a low endothelial cell loss at 6 and 12 months.
Descemet stripping automated endothelial keratoplasty (DSAEK) is a form of selective lamellar corneal transplant surgery that allows replacement of diseased endothelium while maintaining the patients’ own corneal stroma. The advantages offered by DSAEK include a small incision, tectonically stronger cornea, and faster visual rehabilitation with minimal astigmatic shift.
However, significant loss in endothelial cell density (ECD) occurs during DSAEK, attributable partly to the surgical trauma sustained by the graft during insertion into the anterior chamber. This may be particularly true if the technique used involves folding of the graft and insertion with forceps, and especially in Asian eyes with shallow anterior chambers and high vitreous pressures. In extreme cases, extensive endothelial cell loss can result in “iatrogenic” primary graft failure (IPGF) or contribute to graft dislocation.
In this report, we describe the use of the EndoGlide (AngioTech, Reading, Pennsylvania, USA/Network Medical Products, North Yorkshire, UK), an insertion device developed specifically to minimize donor endothelial cell injury during DSAEK. The early results of an interventional clinical trial are also presented.
Methods
Patients
The Singapore National Eye Centre (SNEC) DSAEK EndoGlide Clinical Trial is a prospective interventional trial evaluating the safety and efficacy of the EndoGlide in clinical practice. Consecutive patients with visually significant corneal edema from endothelial dysfunction and who were suitable for DSAEK were enrolled into the study with full informed consent. Prospective data were collected before surgery and included demographic details and prior ophthalmic history. Ethnicity was classified into the following 4 categories as defined by the Singapore Department of Statistics ( http://www.singstat.gov.sg/statsres/glossary/population.html#E ): Chinese, Malay, Indian, and Others. Intraoperative and postoperative complications, including IPGF, graft dislocation, and pupil-block glaucoma, were documented.
Outcome measures were best-corrected visual acuity (BCVA), refractive error, and central ECD before surgery and at 1 month, 3 months, 6 months, and 12 months after surgery. Preoperative donor ECD was based on specular microscopy performed by the Singapore Eye Bank with the Konan Keratoanalyzer EKA-98 (Konan Medical Corp, Hyogo, Japan). Postoperative ECD was performed using the Noncon Robo Specular Microscope NSP-9900 (Konan Medical Corp) in the SNEC by independent and experienced ophthalmic technicians. The ECD was considered acceptable if at least 100 endothelial cells were counted and marked on a high-quality image of the central corneal endothelium; otherwise, the ECD was excluded from the results. Postoperative endothelial cell loss was calculated as a percentage of the preoperative donor ECD.
Other measures include preoperative and postoperative anterior segment imaging with the Visante OCT (Carl Zeiss Meditec, Dublin, California, USA), corneal topography with the Pentacam (Oculus, Lynnwood, Washington, USA), and contrast sensitivity with the Functional Acuity Contrast Sensitivity (Stereo Optical Co, Chicago, Illinois, USA).
Statistical Analysis
Descriptive statistics for normally distributed variables are reported as mean ± standard deviation; otherwise, median and range are reported. The 95% confidence intervals (95% CI) are reported along with the mean 3-month, 6-month, and 12-month percentage ECD loss. All data analysis was carried out with SPSS Statistics 17.0 (SPSS Inc, Chicago, Illinois, USA).
Surgical Technique
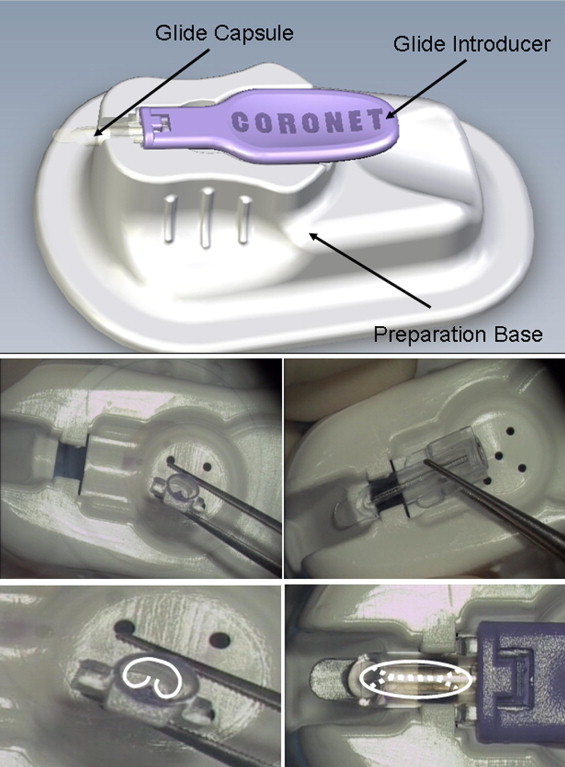
The EndoGlide is an FDA Class 1 medical device approved for use in the United States for DSAEK surgery, and obtained CE mark status in June 2009. The device consists of 3 components: the glide capsule, the glide introducer, and the preparation base ( Figure 1 , Top), on which the glide capsule is preloaded. The glide capsule is a transparent oval plastic chamber with a flat “glide” portion anteriorly to prevent iris prolapse during insertion. An internal central ridge within the capsule ( Figure 1 , Middle left and right) enables automatic coiling of the graft tissue into a “double-coil” configuration when the graft is pulled into the chamber. The double coil allows a much larger graft to be inserted via a cartridge-style system without any overlap of the endothelial surfaces, as opposed to merely rolling the graft along the longitudinal axis. This has since been supported in an experimental DSAEK model using eye bank eyes, where graft insertion with the EndoGlide resulted in ECD loss of 8% (range 5%–13% in 8 eyes) on vital dye staining (unpublished data by Donald T.H. Tan; Clinical Trial Results of New Donor Inserter for DSAEK, presented at the 2010 ASCRS Symposium on Cataract, IOL and Refractive Surgery, Boston, Massachusetts, April 2010). The internal diameter of the capsule is designed to hold a double-coiled graft of up to 10 mm in diameter and 250 μm in thickness without any endothelial-to-endothelial-surface touch. After coiling, the glide introducer is secured onto the posterior end of the glide capsule to form a tight seal, and the assembled EndoGlide is ready for graft insertion into the recipient eye.
Recipient Preparation
A temporal scleral tunnel incision, measuring 4.5 mm wide by 1.5 mm to 2.0 mm deep, is used for graft insertion with the EndoGlide; a similar clear corneal approach is also possible. An anterior chamber (AC) maintainer is preplaced to prevent AC collapse during insertion, and surgeons who are right-handed may find it more convenient to place the AC maintainer 1 clock hour to the left of the main scleral tunnel. The tip of the AC maintainer should not protrude too deeply into the AC, as this may obstruct graft uncoiling; similarly, the bevel of the maintainer is turned towards the limbus, so that the flow of balanced salt solution (BSS) is not directed towards the center of the AC. Descemet membrane is stripped in the usual manner under air or a cohesive viscoelastic (which must then be removed completely). A clear cornea paracentesis is also made at the nasal limbus directly across from the temporal wound; this is for entry of the curved EndoGlide placement forceps (AngioTech/Network Medical Products), which is used to pull the graft from the EndoGlide into the AC. Through a limbal stab incision, an inferior peripheral iridectomy is created to prevent pupil-block glaucoma, as we routinely leave a large air bubble within the AC at the end of all DSAEK surgeries (regardless of insertion technique).
Donor Cornea Preparation and Placement
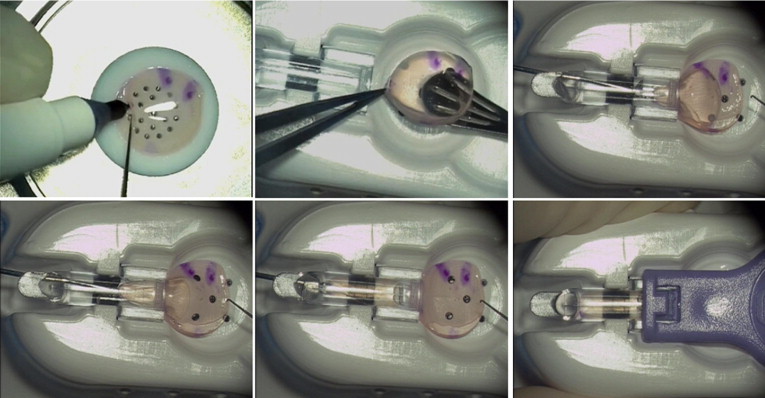
Lamellar dissection of the donor cornea is first performed with an automated lamellar therapeutic keratoplasty (ALTK) system (Moria, Antony, France), and trephined to the desired diameter, which usually ranges from 8.0 to 9.5 mm. The leading edge of the posterior lenticule may be inked on the stromal side for easy visualization ( Figure 2 , Top left), but this step is only necessary in the most advanced forms of corneal decompensation where the AC view is very poor; as gentian violet may adversely affect endothelial cells, other nontoxic dyes may be considered. The edges of the anterior cap and posterior donor lenticule are first separated by gentle irrigation of BSS with a cannula. They are then transferred together onto the donor well of the preparation base, with endothelial surface facing up ( Figure 2 , Top center).
Graft Coiling Procedure
Under the operating microscope, the internal lumen of the glide capsule is lubricated with BSS. A very small ribbon of dispersive viscoelastic is placed on the endothelial surface of the posterior donor lenticule; we prefer Viscoat (Alcon, Fort Worth, Texas, USA), although other viscoelastics such as Ocucoat (Bausch & Lomb, Rochester, New York, USA) may also be used if there are concerns about inadvertent coating of the stromal surface. The straight EndoGlide loading forceps (AngioTech/Network Medical Products) is then introduced through the anterior opening of the glide capsule and used to grasp the leading stromal edge of the posterior donor lenticule ( Figure 2 , Top right). As the graft is slowly drawn into the glide capsule, the sides will begin to coil upwards to adopt a double-coil configuration when the edges of the graft encounter the central internal ridge ( Figure 2 , Bottom left). The double coiling can be facilitated by gentle upward strokes of the edges with a BSS cannula or Sinskey hook. The graft should be drawn forward, fully coiled, until the leading edge just reaches the anterior opening of the glide capsule ( Figure 2 , Bottom center).
Placement of the Glide Introducer
The glide introducer is now inserted into the posterior opening of the glide capsule and locked into place to seal the glide capsule from behind ( Figure 2 , Bottom right). This posterior seal prevents egress of BSS or aqueous from the EndoGlide during graft insertion, which enables a deep AC while minimizing aqueous flow and turbulence even when the AC maintainer is open. The entire EndoGlide complex is removed from the preparation base and is inverted right side up for insertion into the eye.
EndoGlide Insertion
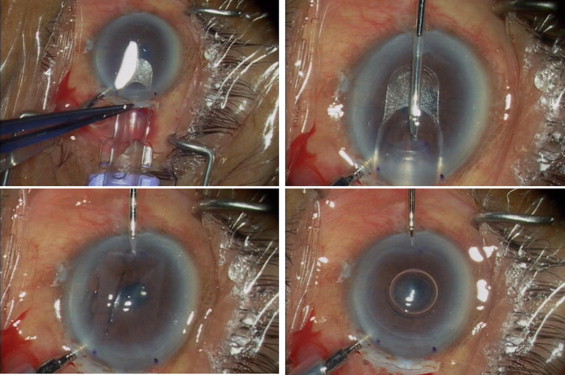
The introducer of the EndoGlide is grasped with thumb and forefinger, in a manner similar to inserting a thumbdrive into the USB port of a computer. The anterior glide surface of the EndoGlide is smoothly inserted into the temporal wound until the anterior opening is seen through the cornea to be fully within the AC ( Figure 3 , Top left). Holding the anterior lip of the wound will help prevent in-folding of the anterior lip during insertion of the EndoGlide. Moderate flow from the AC maintainer and the tight wound seal around the EndoGlide during the insertion process helps maintain the AC depth.
Graft Pull-through and Positioning
While holding the EndoGlide in position, the contralateral hand inserts the placement forceps through the nasal paracentesis into the AC and over the glide surface of the EndoGlide. The leading stromal edge of the graft is grasped and pulled out of the glide capsule and into the AC ( Figure 3 , Top right), where it will automatically begin to uncoil in the correct anatomic position, that is, endothelial surface down ( Figure 2 , Bottom left). Full uncoiling may be achieved by gentle sideways or to-and-fro movements of the graft with the placement forceps, or by increasing the flow of the AC maintainer to further deepen the AC. While still holding onto the graft with the forceps, the EndoGlide is removed, and a small air bubble (eg, 2–3 mm in size) is initially injected beneath the graft in order to float it against the recipient stromal surface; this has been our standard practice for DSAEK since adopting it for our Sheets glide insertion technique. The graft may now be released by the forceps, as the air bubble prevents descent of the graft ( Figure 2 , Bottom right). The surgery is then completed by suturing the main scleral wound and AC maintainer paracentesis site, centering the graft, and injecting more air for a full air tamponade of at least 6 minutes to facilitate graft adhesion to the posterior corneal surface. At the conclusion of surgery, a smaller air bubble, measuring slightly less than the graft diameter, is left in place.
Results
We operated on 25 eyes of 25 Asian patients between January 1, 2009 and February 1, 2010. Demographic and preoperative data are summarized in Table 1 . There were 14 female patients, the mean age was 70 years, and patients were predominantly Chinese (n = 15). The commonest indication for DSAEK was pseudophakic bullous keratopathy (PBK) (12 eyes), followed by Fuchs endothelial dystrophy (9 eyes).
| Gender | |
| Male | 11 |
| Female | 14 |
| Age | |
| Mean | 70.0 years |
| Range | 28-91 years |
| Ethnicity | |
| Chinese | 15 |
| Malay | 2 |
| Indian | 1 |
| Others | 7 |
| Indication for surgery | |
| Pseudophakic bullous keratopathy | 12 |
| Fuchs endothelial dystrophy | 9 |
| Post-laser iridotomy-associated bullous keratopathy | 2 |
| Posterior polymorphous corneal dystrophy | 1 |
| Failed DSAEK | 1 |
| Surgery performed | |
| DSAEK | 11 |
| DSAEK + phacoemulsification/IOL | 11 |
| DSAEK/IOL exchange | 2 |
| DSAEK/anterior chamber IOL | 1 |
Preoperative donor ECD averaged 2957 ± 242 cells/mm 2 , median graft diameter was 8.75 mm (range 8.25–9.5 mm), and average graft thickness was 187 ± 32 μm. All surgeries were carried out by 2 surgeons (D.T.H.T. and J.S.M.) under general or retrobulbar anesthesia. All phakic patients had some degree of cataract and had combined phacoemulsification and intraocular lens implantation performed prior to graft insertion (phaco-DSAEK).
Visual Acuity and Endothelial Cell Loss
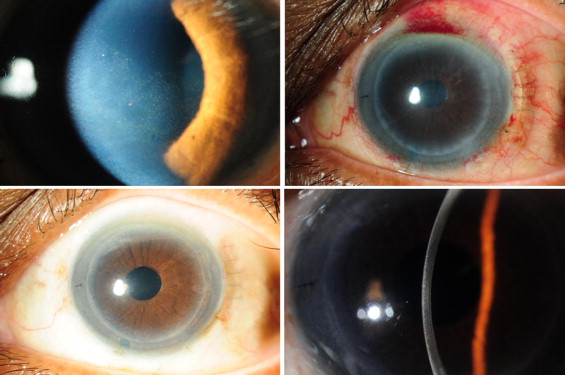
Figure 4 illustrates the results of a typical patient. All eyes completed a minimum of 3 months of follow-up, and in the 18 eyes with acceptable ECD data at 3 months, the mean ECD was 2684 ± 363 cells/mm 2 and mean ECD loss was 9.6% (95% CI, 3.3%-15.8%). Twenty-one eyes attained 6 months of follow-up; best-corrected visual acuity ranged from 20/25 to 20/150, with 12 eyes achieving 20/40 vision or better and no eye losing any lines of vision. In the remaining 9 eyes with sub-20/40 vision, visual recovery was limited in 3 eyes with preexisting glaucoma, 3 eyes with stromal scarring from longstanding bullous keratopathy, 2 eyes with retinal pathology, and 1 eye with congenital nystagmus. The 6-month ECD data from 20 eyes were included; mean ECD was 2586 ± 338 cells/mm 2 , with a mean endothelial cell loss of 13.1% (95% CI, 8.4%–17.8%). Eleven eyes have also completed 12 months of follow-up, and in the 10 eyes with acceptable ECD data, the mean ECD was 2575 ± 289 cells/mm 2 and the mean cell loss was 15.6% (95% CI, 7.0%–24.2%).
Complications
Although all cases were completed successfully, graft insertion was slightly complicated in 3 eyes. The first case was a combined phaco-DSAEK in which vitreous was noted in the AC during graft insertion and required sponge vitrectomy; BCVA was 20/30 and ECD loss was 22.1% at 12 months. The second case required graft manipulation in the AC as part of the graft had folded over on itself when the AC partially collapsed upon removal of the EndoGlide; BCVA was 20/30 and ECD loss was 21.1% at 12 months. In the third case, there was some difficulty controlling the movements of the thin 110-μm graft in the AC, and manipulation of the graft resulted in graft-iris touch; BCVA was 20/25 and ECD loss was 7.2% at 6 months.
Two other eyes also had intraoperative complications of note. In 1 case, there was an uneven lamellar cut with the ALTK during donor cornea preparation, and manual dissection was required to achieve a uniform thickness of 200 μm; subsequent vision was limited by complications of a nonhealing epithelial defect and stromal scarring (see below). A second case had uncomplicated graft insertion but experienced inadvertent chamber collapse and graft-iris touch when forceps were used to remove lint from the AC; BCVA was 20/30 and ECD loss was 19.6% at 12 months.
In the immediate postoperative period, no patient had graft dislocation or IPGF. Postoperative complications have been few thus far, and include 2 patients with presumed steroid-response ocular hypertension requiring only topical glaucoma medications and 1 patient with a nonhealing epithelial defect (as mentioned above) that developed band keratopathy. This last patient required a superficial keratectomy and temporary tarsorrhaphy to facilitate full epithelial healing and best-corrected vision was limited to 20/70 at 6 months because of stromal scarring. To date, none of the eyes has experienced graft rejection or late endothelial failure.
Surgical Experience With the EndoGlide
We found that there is a short learning curve at 2 stages: 1) during double coiling of the graft within the glide capsule, and 2) during uncoiling of the graft in the AC.
On some occasions during the loading of the glide capsule, the donor lenticule may bunch up or adopt a “W”-shaped fold as it is pulled into the glide capsule. This occurs when the sides of the graft do not adequately curl upwards along the inner walls of the capsule, as can happen if the graft is pulled inward too rapidly, if the capsule is not adequately lubricated with BSS, or in very thin grafts. To reduce this occurrence, the use of a BSS cannula or Sinskey hook is recommended in all cases to facilitate the coiling; gentle upward strokes of the stromal sides of the graft will encourage the upward coiling motion along the inner walls of the capsule. In the related situation where the posterior end of the graft folds inwards, forming a “W” configuration, this posterior edge may be grasped at the stromal edge with microforceps to stretch out the graft and prevent the fold. This 2-handed technique is also useful for reversing the pull-through (ie, a graft that initially does not coil appropriately may be gently pulled out slowly, and reinserted).
With regard to graft uncoiling in the AC, this will always occur when the graft is freed of the constraints of the EndoGlide, but full uncoiling may not be complete or instantaneous. If there is obstruction by the underlying iris, then increasing the flow of BSS from the AC maintainer (while still holding onto the graft) often results in complete uncoiling. It should be noted that placement of the AC maintainer should be made such that the infusion is directed away from the center of the AC, as direct infusion against the coiled graft will actually impede uncoiling. Other useful techniques to complete uncoiling include moving the graft to and fro with the placement forceps, or gentle stroking of the graft through the recipient corneal surface.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


