Purpose
To ascertain in vivo confocal microscopic features of corneal/conjunctival intraepithelial neoplasia (CIN) and correlate these with histology of the same lesions.
Design
Observational case series with evaluation of diagnostic technology.
Methods
Four patients with unilateral CIN (3 men and 1 woman) were examined with the Heidelberg Retina Tomograph II (HRT II) Rostock Cornea Module (RCM) confocal microscope before, during, and after treatment. Corneal epithelial samples were taken by alcohol delamination technique in 2 patients, while impression cytology (IC) samples were obtained in the other 2 patients. Morphometric analysis of confocal and histologic images was carried out and the findings correlated. Four controls (all men, 2 with limbal stem cell deficiency, 1 with a limbal lesion, and 1 with diffuse keratoconjunctival proliferation) were similarly examined. Two of these had biopsy for histologic examination. Main outcome measures comprised the degree of correlation between histology and confocal microscopic features of CIN.
Results
Dysplastic cellular changes were noticed on histopathology and correlated well with confocal microscopy, corresponding to the different corneal epithelial layers. Bright nucleoli within huge nuclei and ill-defined cell borders were a feature of the basal epithelium on histopathology and confocal microscopy. Subbasal corneal nerves were not visualized on confocal microscopy in areas affected by CIN. These features disappeared in response to treatment cycles as the basal epithelium reverted to its normal pattern, as seen by confocal microscopy.
Conclusion
Confocal microscopy findings highly correlate with histologic features in CIN. Confocal microscopic features of CIN as defined in this study will enable a reliable diagnosis in a noninvasive manner. Confocal microscopy will also allow real-time monitoring of the condition during treatment.
The term “CIN” is widely accepted in the literature to indicate conjunctival and/or corneal intraepithelial neoplasia, which includes dysplasia and carcinoma in situ. It is a relatively rare condition that more often affects elderly men. A predominantly corneal type of CIN without conjunctival lesions has been well described and frequently considered as a separate entity by some authors. This, however, almost always occurs in association with corresponding limbal lesions. The term “ocular surface squamous neoplasia” (OSSN) is now used to describe the spectrum of lesions but excludes papillomas, melanomas, and lymphomas.
The clinical symptoms are generally nonspecific, with chronic ocular irritation, redness, and varying degrees of visual involvement determined by the extent of encroachment of the lesion on the visual axis. The signs, too, can vary from a distinct limbal lesion to a gray avascular semitransparent thickened sheet of epithelium with a lusterless surface. For this reason, and because of the noninvasive nature of the condition, the diagnosis is often missed or delayed and patients treated for chronic conjunctivitis. Other conditions for which CIN is commonly mistaken include pterygium, corneal pannus, viral keratitis, corneal dystrophy, and fatty degeneration.
Histologic examination of a tissue sample, preferably taken from the limbus, reveals the correct diagnosis. In recent years in vivo confocal microscopy has proved useful as a noninvasive technique to investigate various ocular surface conditions including CIN. However, the diagnostic features of CIN by in vivo confocal microscopy are not yet fully established in the published literature.
Single case reports were recently published describing confocal microscopic features of CIN, including irregular hyperreflective cells with bright nuclei. Malandrini and associates mentioned these features in the superficial layers only, whereas Wakuta and associates described similar changes in all epithelial layers. In this article we present novel in vivo confocal microscopy findings in CIN with emphasis on their diagnostic potential, showing the basal layer heavily populated by dysplastic cells supported by reliable histopathologic correlation. In vivo confocal microscopy description of subbasal corneal nerves in CIN was not mentioned in earlier studies. We also present in vivo confocal microscopy changes in patients after treatment with topical chemotherapeutic agents.
Patients and Methods
The study was an observational consecutive case series. We examined 4 eyes of 4 patients (3 men and 1 woman, age range 57–73) affected by CIN, referred either to the Queens Medical Centre of Nottingham University Hospitals, Nottingham, UK, or to the Ophthalmology Clinic, University “G d’Annunzio” of Chieti-Pescara, Italy. In addition, control eyes of 4 male patients, 2 with limbal stem cell deficiency (LSCD), 1 with a suspicious limbal lesion, and 1 with diffuse keratoconjunctival proliferation, were also studied.
Patients With Corneal/Conjunctival Intraepithelial Neoplasia
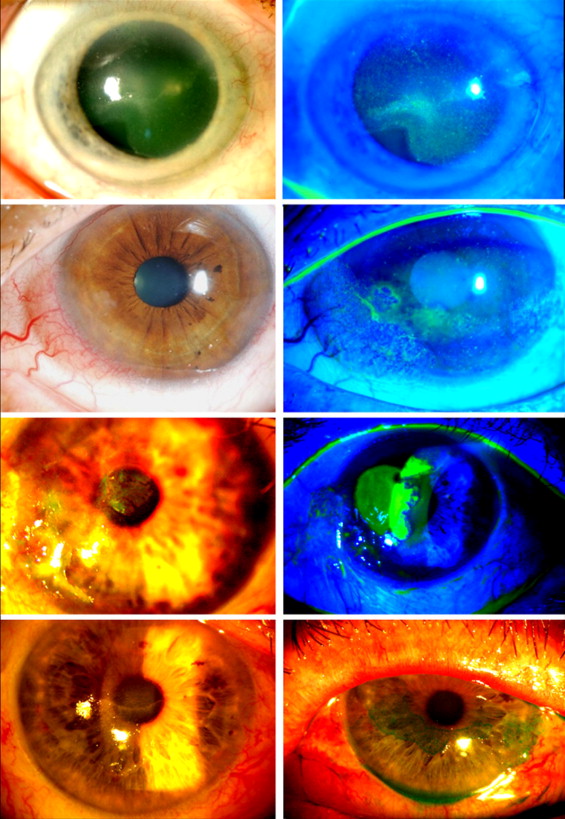
All patients with CIN had superficial corneal opacification confined to the epithelium. Adjacent conjunctival involvement was also observed in all patients. Slit-lamp examination revealed a continuous nonvascularized, semitransparent, relatively thick sheet of abnormal epithelium growing over the corneal surface. This abnormal layer showed a rough, lusterless surface with superficial punctate staining with fluorescein and lissamine green. Patient demographics and clinical findings are given in the Table . Representative biomicroscopic findings of the patients at presentation are illustrated in Figure 1 .
| Patient | Sex | Age | Symptoms | Slit-Lamp Findings | Diagnostic and Therapeutic Intervention | Outcome |
|---|---|---|---|---|---|---|
| CIN | ||||||
| 1 | M | 69 | Ocular irritation, visual impairment | Abnormal corneal epithelium | Alcohol delamination + MMC 0.04% | Complete healing |
| 2 | M | 57 | Ocular irritation, visual impairment | Abnormal corneal and conjunctival epithelium | Alcohol delamination + MMC 0.04% | Partial healing/recurrence/complete healing |
| 3 | F | 70 | Photophobia, foreign body sensation | Abnormal corneal and conjunctival epithelium | Excisional biopsy + MMC 0.04% | Complete healing/recurrence |
| 4 | M | 73 | Ocular irritation, visual impairment | Abnormal corneal epithelium | MMC 0.04% | Complete healing |
| Controls | ||||||
| 5 | M | 22 |
| Superior and inferior fibrovascular pannus on cornea. Clear visual axis. Temporal corneal scar. | Topical steroids and lubricants. No surgical intervention. | Gradually progressing. |
| 6 | M | 74 | Ocular discomfort and visual impairment. Clinical diagnosis: LSCD | Peripheral superficial vascularization and abnormal corneal epithelium | Alcohol delamination | Clearing of visual axis with improvement in vision |
| 7 | M | 63 | Asymptomatic | Localized fleshy limbal lesion 4 × 2 mm | Surgical excision | Settled with no recurrence |
| 8 | M | 66 | Ocular discomfort, dry eyes. Clinical diagnosis: DKP | Circumferential encroachment of fibrovascular tissue (conjunctiva-like) on cornea. Visual axis clear. | Topical lubricants | Stable, no signs of progression |
Previous treatment received included scraping of abnormal epithelium (1 case) and topical steroids and lubricants (2 cases). Corneal epithelial samples were taken (impression cytology and biopsy using alcohol delamination ) from each patient for histopathology. After histologic diagnosis of CIN, patients were treated with topical mitomycin C (MMC) 0.04% 4 times a day for a week, followed by 1 week off. The number of such cycles required for complete resolution was 2 to 9. One patient required additional application of 0.04% MMC-soaked sponges for 5 minutes, 1 application per week for a total of 5 applications, to achieve complete response.
Alcohol delamination of the corneal epithelium was performed to obtain tissue for histology. Twenty percent ethanol was applied to the central 6 mm of the dysplastic corneal epithelium for 40 seconds using an optical zone marker (Bausch & Lomb, Kingston-upon-Thames, Surrey, UK). The alcohol was then drained from the well with a surgical sponge (K-sponge; Katena Products, Denville, New Jersey, USA) and the surface washed with saline solution before peeling off the loosened epithelium. Biopsy specimens were floated on a few drops of saline placed on nonabsorbent paper and unfolded with fine forceps by gentle stroking. The saline was absorbed with a K-sponge such that the epithelial sheet lay flat on the paper. The sheet was then covered with a few drops of 10% formalin and kept covered for 15 to 20 minutes before transferring to a formalin pot for transfer to the laboratory. Specimens were paraffin embedded and 5- to 7-μm sections were stained with hematoxylin-eosin. Slides were reviewed with the help of the Nanozoomer Digital Pathology scanner (NDP C9600 series; Hamamatsu Photonics K.K., Hamamatsu City, Japan), using the software for high-magnification views and cell morphometry.
For impression cytology, under topical anesthesia a cellulose acetate filter paper disc (Millipore. 0.45 μm; Millipore Corp, Bedford, Massachusetts, USA), marked for orientation, was applied to the surface of the dysplastic epithelium and firm pressure applied to the paper with a Goldmann tonometer headpiece. The paper was allowed to remain in contact with the eye for approximately 5 to 10 seconds, then peeled off with a forceps and placed in fixative solution before transfer to the laboratory. Cells were stained with hematoxylin-eosin.
Each patient was examined with a digital laser-scanning confocal microscope (LSCM) (HRT II Rostock Cornea Module; Heidelberg Engineering GmbH, Heidelberg, Germany). The software driver (Eye Explorer) of this confocal microscope allows for an automated z-scan with determination of focal depth within corneal layers in high-contrast digitized images of 400 × 400 μm each. The corneal surface was evaluated in all patients with emphasis on visualizing epithelial cell morphology at the site of CIN and its borders. In vivo confocal microscopy examinations were performed in the active stage, after treatment, and in the event of recurrence for all patients who signed a written consent form for this examination.
In vivo confocal microscopy was carried out under topical anesthesia with Minims Oxybuprocaine Hydrochloride 0.4% (Chauvin Pharmaceuticals Ltd, Surrey, UK). A digital camera mounted on a side arm furnished a lateral view of the eye and objective lens to monitor the position of the objective lens on the surface of the eye. A drop of 0.2% polyacrylic gel (Viscotears liquid gel; Novartis Pharmaceuticals UK Ltd, Surrey, UK) served as coupling medium between the polymethyl methacrylate contact cap and objective of the LSCM. Sequential images derived from automatic scans and manual frame acquisition throughout the corneal lesions were obtained from each examined eye. Epithelial cell density (cells/mm 2 ) was calculated using the analysis software of the instrument.
Controls
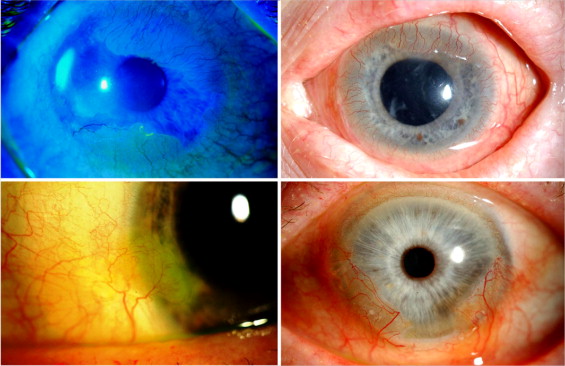
Patient demographics and clinical findings are given in the Table and in Figure 2 . One patient had LSCD secondary to unilateral alkali burn. Abnormal conjunctivalized epithelium covering a fibrovascular pannus had encroached on the cornea superiorly and inferiorly. Another patient with LSCD had central corneal involvement with a thin opaque layer of “conjunctivalized” epithelium. This was removed by alcohol delamination. One male patient had a suspicious fleshy lesion at the limbus encroaching on the cornea. An excisional biopsy was performed. One male patient had diffuse keratoconjunctival proliferation, affecting the peripheral cornea from the 3-o’clock to 10-o’clock position, with a small, relatively unaffected area of 1 clock hour at the 6-o’clock position. The visual axis was clear. He was managed conservatively.
Results
Corneal/Conjunctival Intraepithelial Neoplasia
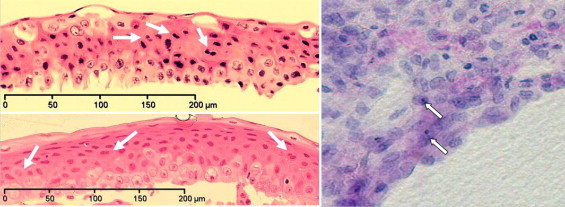
In histology a multilayered epithelium with cellular and nuclear pleomorphism in the basal layer and reversal of the nuclear cytoplasm ratio were observed. Some cells had multiple nuclei and most of the basal cells had prominent nucleoli ( Figure 3 ). Such dysplastic cells were also noted in the suprabasal layers in some sections. Representative images from 2 patients are shown in Figure 3 (Left top and bottom). The nucleoli of the basal cells measured using the morphometry software of the Nanozoomer ranged from 2.60 to 3.98 μm (mean ± SD = 2.84 ± 0.60 μm) ( Figure 4 , Top right and left). (Basal nuclear size in nonmetaplastic corneal epithelial cells measured with the Nanozoomer is 7.84 ± 0.40 μm [mean ± SD] [personal observation].) The basal cell nuclei ranged from 8.2 to 16.6 μm (mean ± SD = 11.9 ± 3.765 μm) while the middle layer nuclei were 6.61 to 11.1 μm (mean ± SD = 8.98 ± 1.52 μm) ( Figure 4 , Bottom).