Dermatology
Alex V. Levin
Thomas W. Wilson
David Rootman
Elise Héon
Dermatologic diseases will often have an associated ophthalmic manifestation because of the common embryologic origin of the ocular structures and the skin. The skin and ocular surface are both of ectodermal origin. The skin covering the eyelids, the lashes, all eyelid glands, the lacrimal gland, the conjunctival epithelium, and the corneal epithelium are all derived from surface ectoderm. The lens of the eye is also a surface ectoderm derivative. Dermatologic disease involving the periorbital skin area can cause secondary abnormalities of the ocular surface. Skin diseases affecting the mucous membranes such as Stevens-Johnson syndrome will often have ocular manifestations as conjunctiva is a mucous membrane. The ectodermal dysplasias are a group of rare genetic diseases with a wide clinical spectrum involving skin, eyes, teeth, hair, nails, and sweat glands. Ocular manifestations may include corneal surface disease, conjunctival disorders, lid abnormalities, or cataract.
Skin pigment is derived from melanosomes, which originate as neural crest cells. Likewise, the melanocytes of the uveal tract are also neural crest descendants. Melanosomes are also found in the retinal pigment epithelium, a neuroectodermal derivative, where pigmentation is required for normal development of the overlying retina. Oculocutaneous albinism refers to those disorders in which deficiency of melanin or melanosomes manifests in both skin and eye. Ocular albinism refers to an isolated ocular hypopigmentation disorder.
Dermatologic treatments can also cause ocular side effects. Steroid creams can cause an increase in intraocular pressure and lead to glaucoma cataracts. Systemic tetracycline used to treat acne can cause pseudotumor cerebri. The retinoids are natural and synthetic compounds that produce similar effects to vitamin A and can also cause pseudotumor cerebri.
There are numerous other examples of combined dermatologic and cutaneous manifestations, many of which are covered elsewhere, such as the phakomatoses (Chapter 23), rheumatologic disorders such as lupus (Chapter 27), and skeletal disorders such as pseudoxanthoma elasticum (Chapter 28). This chapter will focus on disorders that are primarily dermatologic and that have associated involvement of the oculofacial regions.
 Figure 15.1 Ectrodactyly–Ectodermal Dysplasia (EEC Syndrome) The predominant features of this autosomal dominant syndrome are ectrodactyly (shown here), ectodermal dysplasia, and cleft lip/palate. When associated with urinary tract abnormalities, the syndrome is named EEC-UT. Other manifestations include oral and facial abnormalities, dry eye, and hypohidrosis. Patients have absence of eyelashes, thin hair and eyebrows, and decreased skin pigmentation. Meibomian glands are decreased or absent, leading to corneal vascularization and scarring. The lacrimal punctum may be small or absent. Aggressive tear replacement therapy is necessary to maintain normal ocular surface and reduce photophobia. Retinal detachment may also occur. One variant is the rare autosomal recessive association of ectodermal dysplasia and macular dystrophy: Ectrodactyly–ectodermal dysplasia–macular dystrophy (EEM) syndrome. |
 Figure 15.2 Incontinentia Pigmenti (Bloch-Sulzberger Disease) Incontinentia pigmenti is an X-linked dominant disorder that is almost always lethal in males. It is caused by mutations in the NEMO gene at Xq28 with another locus postulated for the disorder at Xp11. The cutaneous lesions, which are distributed along the lines of Blaschko, evolve from an early bullous phase with erythematous papulosquamous lesions (left image) to a hyperkeratotic verrucous stage, followed by swirling and patchy hyperpigmentation (right image) with or without hypopigmentation, atrophy, and scarring in its later stages. Neurologic features include seizures and mental retardation. (The authors are grateful for the contributions of Dr. Christopher Cessna to this legend.) |
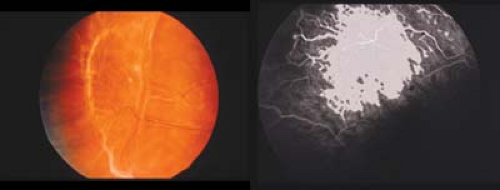 Figure 15.3 Incontinentia Pigmenti (Bloch-Sulzberger Disease) Ocular manifestations are often asymmetric and include peripheral retinal avascularity similar to that seen in retinopathy of prematurity (Chapter 8: Retina and Vitreous, Figs. 8.6, 8.7, 8.8, 8.9, 8.10, 8.11, 8.12, 8.13, 8.14, 8.15, 8.16, 8.17, 8.18, 8.19, 8.20, 8.21, 8.22 and 8.23) with retinal ischemia inducing neovascularization and bleeding/exudation. The findings are usually worse temporally. Milder cases may only show straightening of the far temporal peripheral retinal vessels. Temporal dragging of the macular vessels is an ominous sign. If a child is fully vascularized without leakage or traction on first examination, then he or she will not develop retinopathy. |
 Figure 15.4 Incontinentia Pigmenti (Bloch-Sulzberger Disease) In cases of retinopathy, progression to traction retinal detachment can be rapid. Careful periodic follow-up is essential. Other reported signs include optic atrophy, foveal hypoplasia, microphthalmos, cataracts, conjunctival pigmentation, iris hypoplasia, uveitis, nystagmus, strabismus, and whorllike epithelial keratitis. Dental abnormalities are seen in greater than 80% of cases and include absent teeth and conical teeth with supplemental cups. |
 Figure 15.5 Hypomelanosis of Ito Patients with hypomelanosis of Ito present with cutaneous abnormalities consisting of hypopigmented patches and streaks. (right image) Brain migration disorders are common and result in brachycephaly and micropolygyria. Ophthalmic manifestations include coloboma, iris heterochromia, microphthalmia, and choroidal atrophy. (left image) Biopsy of affected skin may show mosaicism for one of the many reported associated chromosomal aberrations. This girl had congenital glaucoma, developmental delay, and a mosaic isochromosome 8.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|