Fig. 15.1
Panoramic radiograph of 10 year old child in mixed dentition stage. The adult maxillary and mandibular incisors and first (6-year) molars are fully erupted in addition to the deciduous canines and molars. The second molars (12 year molars), canines, and premolars have not yet erupted, and can be seen developing behind the first molars and below the deciduous canines and premolars, respectively. Note the incomplete root formation of the molars and premolars at this age. Also note the endodontically treated maxillary right central incisor with radio-opaque material filling the root canal and a restoration of the previously fractured crown
Dental and Oral Injuries
Dentoalveolar injuries are the most frequent facial injury in children. Many of these are treated by the dentist or oral and maxillofacial surgeon in an outpatient office setting. Many traumatic injuries in young athletes involve head trauma so a thorough medical and neurological exam is necessary. Blunt trauma from an object, particularly in sports such as football, baseball, or hockey, is one of the most common mechanisms of injury [1–5].
Diagnosis
A careful oral examination should be performed in all dental and facial trauma cases. As with any trauma evaluation, the clinical history of the accident is very important. The oral injury may be a distracting injury, especially if a tooth is avulsed or displaced and there is a significant amount of hemorrhage from the oral cavity lacerations. It is important that this does not distract from the bigger picture of the trauma evaluation. Particularly in cases of significant force to the head, loss of consciousness and other injuries need to be addressed. Concussions, cervical spine injuries, and head trauma are discussed in separate chapters [1].
For the examination of the oral and maxillofacial region, the examiner should evaluate the soft tissue for any lacerations extraorally as well as intraorally and look for any missing, loose, or chipped teeth. It is also very important to evaluate the occlusion , since a malocclusion, or step-off in the occlusal plane, can reveal a mandible fracture or displaced teeth. All teeth should be accounted for. An attempt should be made at the scene to locate any avulsed teeth and these should be immediately replanted or properly transported in the appropriate storage medium if any attempt at replantation is to be made. Exposure of the root surface and severing of the neurovascular bundle at the tooth root apex leads to tooth necrosis, and prolonged avulsion greatly reduces the chance for a successful rescue. Ideally, if it can be accomplished safely, the avulsed tooth is transported in its original socket. If this cannot be accomplished safely, there are commercially available solutions for storing avulsed teeth, such as Hank’s Balanced Salt Solution (HBSS) . When such media are not available, avulsed teeth may be transported in pasteurized milk. If there is no alternative, teeth may be transported in saliva or saline. Chipped teeth and fractured crowns should prompt the clinician to look for intraoral lacerations since fragments can often become imbedded in soft tissues. In cases of missing teeth or fragments that cannot be accounted for, a chest radiograph is a prudent exam, especially in cases with significant trauma and loss of consciousness. Dental fragments can easily be aspirated and, if revealed on plain films, need to be retrieved. In cases of swallowed fragments, revealed on an abdominal radiograph, these usually do not require any treatment other than surveillance [1].
The radiographic examination is a critical component of the trauma evaluation. The panoramic radiograph is an excellent screening tool that will show the entire upper and lower jaw in one plane, as well as the entire dentition. Many patients already have a CT scan, especially if evaluated for head trauma in the emergency room. However, the mandible and lower teeth are often excluded in the window of the typical brain CT used to screen for intracranial hemorrhage. Even in cases where a face CT is obtained, the panoramic radiograph is still a helpful tool for several reasons. First, it will reveal mandible fractures and relative displacement, as well as all erupted and unerupted teeth, which are present in many adolescent athletes and children. The panoramic radiograph shows the entire dentition together in a single plane making evaluation much easier. It allows for evaluation of root formation and detection of root fractures, which will determine treatment. The radiograph can also determine the presence of foreign bodies and fragments of teeth imbedded in soft tissue [1] (Fig. 15.2).
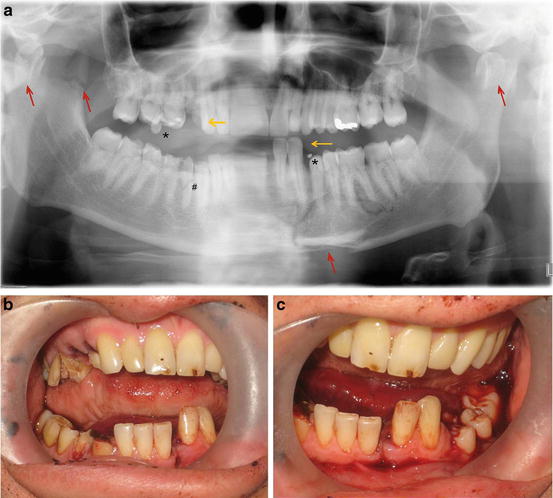
Fig. 15.2
(a) Panoramic radiograph of traumatic injury to the mandible with multiple findings. Vertical arrows point out mandibular fractures in the left parasymphysis region, bilateral condylar fractures, and right coronoid process fracture. The * points out tooth fragments. The # points out a root fracture of the right mandibular premolar. The horizontal arrows point out a stepoff in the occlusal plane corresponding to mandible fracture and displacement of the canine and lateral incisor in the mandible and fractured dental crowns in the maxilla. (b) and (c) show corresponding clinical photos of the stepoff in the occlusal plane in line of fracture and fractured teeth. Due to severity of mandibular injuries, the patient required surgery and open reduction with internal fixation of mandibular body fractures
An initial panoramic radiograph is also very useful since this radiograph is used as a baseline for future panoramic radiographs obtained during follow-up care. Individual radiographs of traumatized teeth should also be taken since they are much more sensitive than the panoramic radiograph in determining root fractures with minimal displacement. The radiographs can be taken at multiple angles to determine position and direction of luxations, as well as the relationship of injured primary teeth to underlying permanent dentition. In fact, with deep lacerations of the lips, it is often wise to take a periapical radiograph of the soft tissue to look for foreign bodies such as tooth fragments. An occlusal radiograph can be a useful supplement to determine the relationships of the anterior dentition to the developing permanent dentition [1, 5–7].
It is worthwhile noting that over the last few years, many dental and surgical offices have been equipped with low-dose conebeam CT scanners, which are increasingly used for evaluations, and provide an excellent 3D image of the dentoalveolar structures as well as a reconstructed panoramic view at a fraction of the exposure of a medical CT. This technology has enhanced the diagnostic capabilities of many local offices and clinics.
Types of Injuries
Injuries to teeth and surrounding structures can be subdivided into injuries affecting the hard tissue of the teeth alone such as chips and fractures of the crown; injuries of the dental pulp, such as crown fractures involving pulpal exposure; injuries to the surrounding periodontal support tissues and supporting bone; and finally injuries to the gingival and soft tissues of the oral cavity. In most instances there is injury involving multiple structures, combining these types of injuries. The treatment of particular injuries to the oral cavity and dentition depends on the type of dental injury and is discussed in the context of each injury [8, 9].
Oral Soft Tissue Injuries
Tongue lacerations are usually a result of bite injuries sustained in a collision or fall with chin trauma, resulting in the tongue being trapped between the teeth. The tongue and oral mucosa heal very quickly, and the resulting minor tongue lacerations often do not require suturing. However, temporary hemorrhage can occur and be significant since the tongue is very vascular, but this is usually self-limiting. When suturing is required, resorbable sutures such as plain or chromic gut are always used. The patient is also often treated with a course of topical antimicrobial chlorhexidine rinse and antibiotics if necessary.
Dental injuries are often accompanied by abrasions and lacerations of the surrounding gingiva. In the anterior maxilla and mandible, the vestibular frenum attachment in the midline is often torn and injured since it is easily mobile and friable. These wounds often require a few resorbable sutures. Gingival lacerations should be treated, especially if the gingiva is detached or stripped off the alveolar bone. The treatment usually involves interdental sutures to reapproximate the gingiva. This will allow for proper healing preserving soft tissue aesthetics. Gingival lacerations and injuries tend to heal very quickly, since oral mucosa has a very high turnover rate.
Lip lacerations often occur when the lip becomes trapped between the upper and lower teeth. These can be through-and-through lacerations with the teeth biting through the lip. Lip lacerations often require repair, especially in cases where the laceration crosses the vermillion border. Any lacerations should be carefully examined for the presence of tooth fragments or foreign bodies since these can become a nidus of infection. This is where a soft tissue radiograph can be useful to look for foreign objects. Thorough debridement and copious irrigation is necessary. The antibiotics of choice in oral injuries are typically penicillins, which have excellent oral microbial coverage . In cases of penicillin allergy, clindamycin is typically the preferred option (Fig. 15.3).

Fig. 15.3
(a) Example of a 9-year-old patient in a bicycle accident with soft tissue injuries and dental fragments within deep lip laceration. Patient suffered multiple abrasions, with a through and through upper lip laceration. (b) Multiple dental fragments from the fractured teeth are noted embedded in the soft tissue. (c) The wound was carefully debrided and irrigated prior to layered closure. The loose dental fragments were removed
Hard Tissue Injuries
Our discussion here will involve the various types of dental injuries, the treatment, and future sequela. All of these aspects are important principles for primary clinicians involved in the management of athletes, from the youth to professional levels, as well as for parents and for the athletes themselves. The treatment of these hard tissue dental injuries is based on the anatomy of the teeth and surrounding tissues, ranging from limited to severe injury of the crown and root to the displacement of teeth and injury of the periodontium and supporting bone. Treatment is guided by the severity of the anatomical components injured. The World Health Organization (WHO) has presented a widely accepted injury classification system that is based on anatomic considerations and accepted therapies of dental injuries and surrounding structures. The system, known as the Applications of International Classification of Diseases to Dentistry and Stomatology (ICD-DA), was initially published in 1973 with the third edition published in 1994. It has been modified by Anderson and colleagues and is still widely used [8, 9].
Dental Inj uries
Injuries of teeth can be described based on the component of the injured tooth. A fracture of a tooth can involve multiple layers of the crown of the tooth including the enamel and dentin, can extend into the pulp, and can involve the root. An uncomplicated crown fracture involves the enamel and dentin only and does not expose the pulp. This may be a simple chip of the enamel involving only the incisal edge of an incisor or a more substantial fracture involving both enamel and dentin. In the case of a fracture extending to the dentin, the tooth may exhibit increased sensitivity. Ellis classified these fractures as Type I (involving enamel only) and Type II (involving enamel and dentin) [9]. Treatment of an uncomplicated fracture typically involves composite bonding to restore form and aesthetics. If a large fragment is fractured, it should be saved and brought to the dentist since in certain cases it may be used and bonded to the remaining tooth. The definitive treatment and material will be determined by the restoring dentist based on the amount of missing tooth structure [1, 4, 5, 8, 9] (Figs. 15.4 and 15.5).
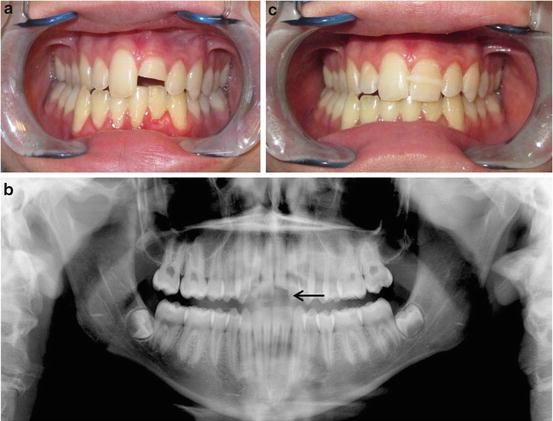
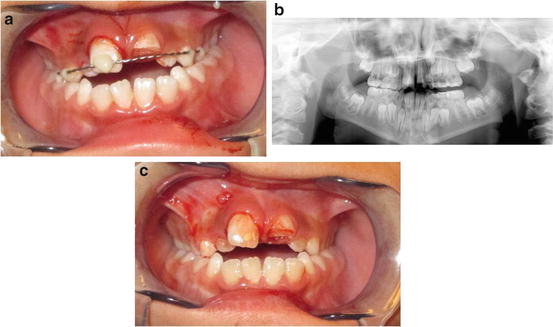
Fig. 15.4
(a) Sixteen-year-old patient with a crown fracture involving enamel and dentin of the maxillary left central incisor, sustained in an ice-skating accident. The patient saved the crown fragment. (b) Panoramic radiograph showing fracture. (c) It was provisionally bonded to the tooth in the emergency room reducing sensitivity and restoring esthetics. He later followed up with his dentist for definitive treatment
Fig. 15.5
(a) A 10-year-old boy involved in an ice-skating accident. Clinical presentation involving luxation and enamel and dentin fracture of the right central incisors and a complicated fracture of the left central incisors involving the dentin and pulp exposure of the left central incisor. (b) The panoramic radiograph shows the fractures and no other injuries. (c) Treatment involved splinting the slightly mobile right central incisor. The left central incisor will require additional treatment and restoration
A complicated crown fracture involves exposure of the dental pulp. This type of fracture involving enamel, dentin, and pulp exposure was classified by Ellis as Type III [9]. This type of injury should be evaluated as soon as possible by a dentist since prognosis depends on factors such as age of the patient and stage of dental development, time of exposure, and amount of pulpal exposure. All exposed pulpal tissue will require treatment. In cases of small pulpal exposures in young patients that have incompletely formed root apices, the prognosis of pulpal survival is much better than in adults where the tooth root is completely formed and the apex (where the neurovascular bundle enters the tooth) is closed. Significant pulpal exposure in older patients will likely require endodontic therapy , with long-term prognosis to be determined by close follow-up on clinical and radiographic exams by the patient’s dentist [7, 9].
The dental hard tissue injury can also extend into the root of the tooth. The crown-root fracture can extend into the cementum, or root structure, again with pulpal exposure (complicated) or without pulpal exposure (uncomplicated). An injury involving the root was classified as a Type IV fracture in the Ellis classification [9]. Fractures that extend past the gingival margin into root structure cause significant damage and may have a poor prognosis depending on the level of root fracture. If there is no pulpal exposure in certain cases, the mobile crown segment can be removed and the tooth restored. In cases of pulpal exposure in young patients with incomplete root formation, the dentist may be able to preserve pulpal vitality. In older patients, once root formation is complete, and there is a complicated (pulpal exposure) crown-root fracture, the tooth will require root canal therapy if it is restorable. These cases often require complicated restorative procedures, including full coverage crowns to fully restore function and aesthetics. In the extreme crown-root fracture, where the tooth is fractured along its vertical axis, the tooth is non-restorable and requires extraction. Often, complicated crown-root fractures also result in non-restorable situations or very difficult restorative situations where it may be more beneficial to extract and replace the tooth based on cost, prognosis, and risk and benefit discussion with the patient. Treatment planning of complicated fractures often requires endodontic treatment as well as involvement of the orthodontist to extrude the tooth to allow exposure of enough tooth structure for the dentist to restore the tooth. These decisions are based on the individual patient and involve multiple specialists and are beyond the scope of this discussion [4–23] (Fig. 15.6).
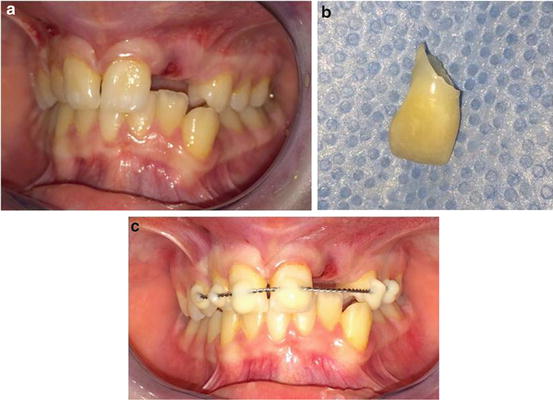
Fig. 15.6
(a) Complicated crown injury involving crown and root of the left maxillary lateral incisor, extending below the gingiva. (b) The fractured segment is nonrestorable due to root fracture being in the coronal segment and the oblique angle. (c) The adjacent subluxed teeth were splinted for 2 weeks. The remaining root will require extraction and eventually an implant will be placed
Although rare, accounting for about 7.7 % of injuries to the permanent dentition, a dental injury can involve an isolated root fracture. The most commonly affected teeth are the maxillary incisors since they are most exposed and most easily injured. These fractures are often detected on radiographic exam. The involved tooth may also be slightly extruded from the socket and luxated. The prognosis depends on the level of the horizontal root fracture. The best prognosis occurs in root fractures involving the apical (deepest) third of the root and the worst in cases near the coronal third. Fractures involving the most apical third of the tooth are typically stabilized with a flexible splint for 4 weeks. More coronal root fractures may involve longer splinting periods. These teeth need to be carefully monitored for pulpal necrosis and need for endodontic therapy by the patient’s dentist [4, 5, 7, 20].
Primary teeth can sustain similar injuries to the permanent dentition. However, the age of the patient and time to planned exfoliation of the tooth also need to be considered prior to treatment. The priority is placed on preservation of the erupting or developing permanent dentition. Therefore, primary teeth are never replanted, and severely luxated primary teeth are often extracted [6] (Fig. 15.7).
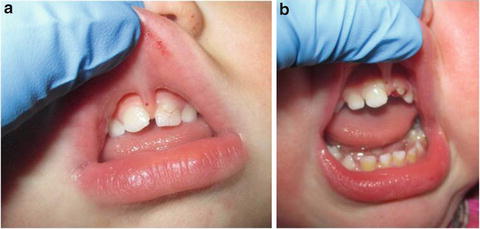
Fig. 15.7
(a) A 19-month-old with trauma to the left maxillary central incisor. The crown was fractured below the gingival margin with pulpal exposure and the tooth was nonrestorable. (b) The tooth was extracted due to significant fracture
It is important that parents understand that early extraction of primary teeth can sometimes alter the eruption of the adult teeth and can cause crowding in the permanent dentition, so long-term follow-up is important. A soft diet is recommended for at least a week as part of the treatment of all concussion, subluxation, and luxation injuries for symptom relief and to allow healing of the surrounding structures.
Injuries to Surrounding Structures
Concussion and subluxation are injuries to the periodontium, the supporting structure of the tooth. A concussion is typically sustained in mild trauma and is manifested by sensitivity and tenderness to percussion or biting, without displacement or loosening of the tooth. Concussion injuries typically improve with soft diet and do not require any splinting or stabilization. There are usually no radiographic abnormalities on exam. The injury should be followed for symptom resolution and vitality testing by the patient’s dentist [15, 16].
Subluxation injury typically requires more force and involves loosening of the traumatized tooth without displacement. The tooth will be tender to touch and percussion. There will likely be no radiographic abnormalities since there is no displacement. If there is mobility of the tooth, it may need to be splinted with a flexible composite bonded splint for 2 weeks. The patient should be placed on a soft diet for a week. This injury should also be followed for symptom resolution and vitality testing [11, 15, 16].
Luxation indicates a movement from the normal position. Luxation injury can be extrusive, lateral, or intrusive in nature. This typically occurs with significant force and is often associated with fracture of a tooth as well as the alveolar bone supporting the tooth. Splinting is typically required with a flexible splint for a period of 2 weeks. Extrusive luxation is displacement of the tooth outward or incisally out of the socket. Lateral luxation involves any lateral movement out of the occlusal arch, other than in an apical or coronal direction [16–18] (Fig. 15.8).
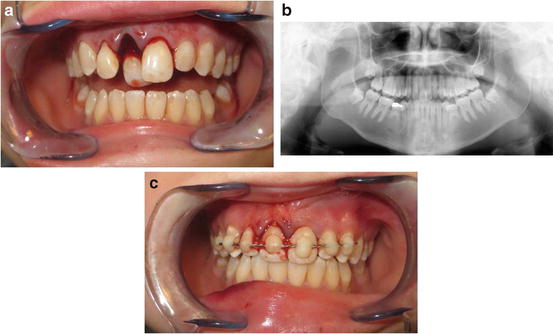
Fig. 15.8
Extrusive and palatal luxation of the maxillary right central incisor in a football injury without use of a mouthguard. (a) Initial presentation. (b) Panoramic radiograph shows no other bony or dental injuries, with the tooth displaced and out of the correct occlusal plane. (c) Since there was no alveolar bone fracture, the tooth was repositioned after administration of local anesthesia and splinted with a flexible composite-bonded splint
This type of injury often involves a fracture of the thin overlying alveolar bone cortex. Intrusive luxation defines apical displacement into the alveolar bone. Teeth that are extruded or laterally luxated are usually repositioned in the office under local anesthesia. In the case of intrusion, the tooth is pushed into the socket and can either be allowed to re-erupt or can be repositioned based on the patient’s age. On occasion, significant intrusion may require orthodontic forces to reposition the tooth gradually. In teeth of older patients with complete root formation, intrusion injuries often lead to pulp necrosis and will frequently require endodontic treatment . Intrusion injuries in particular may have significant sequela in the future. In cases of primary dentition, depending on the child’s age, luxation of a deciduous tooth may not require much force, since the roots of deciduous teeth are gradually resorbed by the erupting permanent teeth. In these cases the primary teeth are often extracted [4, 6, 22] (Figs. 15.9 and 15.10).
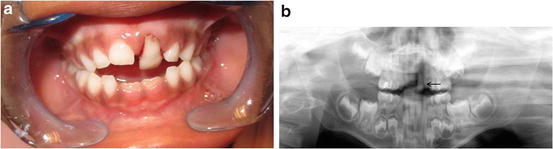

Fig. 15.9
(a) An example of a primary maxillary left central incisor luxated in a 5-year-old girl. (b) Panoramic radiograph shows degree of luxation and proximity of adult teeth, and short root. The tooth was extracted during the visit
Fig. 15.10
(a) Extrusive luxation of primary central incisors in a 6-year-old. (b) Panoramic radiograph showing degree of displacement. Note the short roots of the primary incisors as a result of root resorption by the erupting permanent incisors. (c) The teeth were extracted. After extraction, a follow-up periapical radiograph in clinic shows a small residual root tip. This will resorb as the adult teeth erupt over the next year
After an intrusion injury, teeth have a higher risk of ankylosis or root resorption even years after the injury, so long-term surveillance by the patient’s dentist will be required to monitor for such signs. In the case of a young patient where the adjacent dentition is still erupting, ankylosis may lead to dental crowding or malocclusion as the surrounding dentition develops and adjacent teeth erupt, while the ankylosed tooth can no longer move [4, 5].
In the case of the deciduous dentition, intrusion injuries may also damage the crowns of the developing adult teeth below the roots of the primary tooth. In certain scenarios, and depending on the degree of intrusion of the primary dentition, the injured primary teeth may require extraction. It is important to stress the long-term surveillance and follow-up of these injuries by the patient’s dentist to monitor for these sequelae [18–20].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


