Degeneration and Atrophy of the Choroid
Richard G. Weleber
Peter J. Francis
The goal of this chapter is to present an overview of degeneration and atrophy of the choroid. As such, we present a differential diagnosis of the different types of degeneration and atrophy of the choroid and briefly discuss some disorders that will be covered more extensively in other chapters, such as gyrate atrophy, choroideremia, the inherited macular dystrophies, and retinitis pigmentosa. In this chapter, we will focus on the choroidal manifestations of these allied disorders and will leave the reader to refer to other chapters for more complete discussions.
DEFINITION
The term choroidal degeneration refers to a group of disorders that present with acquired, usually progressive cellular or tissue dysfunction resulting eventually in cell death and consequent structural changes involving the choroid. Atrophy of the choroid is a more specific term that applies to the anatomic changes that arise from loss of cells and tissue subsequent to cell death. Atrophy of the choroid can be either congenital or acquired and can occur from any process that involves cell loss. Dystrophy is the term that applies to acquired cell or tissue degeneration with subsequent atrophy that is the result of a genetic defect, such as a deficiency of an enzyme (i.e., ornithine aminotransferase deficiency in gyrate atrophy of the choroid and retina) or a mutated gene product (i.e., atrophy that can be seen with patients who carry mutations of the rhodopsin gene or the peripherin/RDS gene).
One cannot assume that the basic underlying defect in choroidal atrophies and dystrophies resides in the choroid alone. Both gyrate atrophy and choroideremia are the result of defects of gene products that are widespread throughout the body but, for different reasons, produce pathology limited mostly to the eye. The choriocapillaris has an intimate association with the pigmented retinal epithelium, and any disorder, genetic or otherwise, that produces a loss of one will be expected to also eventually result in a loss of the other. The recent discoveries of peripherin/RDS mutations in patients with either diffuse or regional choroidal atrophy indicate that even defects of proteins limited in expression to the photoreceptors can result in pigment epithelial and choroidal atrophic changes.
RELATIONSHIP TO AGING MACULAR DEGENERATION
Degeneration and atrophy of the choroid can occur as part of age-related macular degeneration. Often the end stage of specific disorders, such as Best’s macular dystrophy, Stargardt’s macular dystrophy, pattern dystrophy of the retinal pigment epithelium, Sorsby’s fundus dystrophy, North Carolina macular dystrophy, and juvenile X-linked retinoschisis, will present with an atrophic fundus appearance that is mistaken for that resulting from advanced typical aging macular degeneration. Several investigators have suggested that many common forms of aging macular degeneration are the result of genetic disease.1,2 Stone and Sheffield have proposed that some forms of aging macular degeneration may be mutations allelic to known macular dystrophies but differently expressed with regard to age of onset because the mutations involved affect a different portion of the gene product.3
One of the problems that has impeded searches for genes associated with age-related macular degenerations has been the lack of multigeneration families to study because of the late age of onset. Classical studies of linkage by descent are most productive in large families with three or more generations of individuals available for study. Newer genetic techniques, such as affected pedigree member analysis4 and sib pair analysis and association studies5 represent powerful tools to discover and map new genes that cause macular degeneration.
In general, specificity of any degenerative or dystrophic process is reduced or lost as the disorder progresses. In the end stages, the fundus appearance may resemble that of any of a number of diseases. Seeing the range of various expression and stages of progression in multiple affected family members is very helpful in recognizing and differentiating one form of choroidal atrophy or degeneration from another. Special tests, such as the fluorescein angiogram, optical coherence tomography (OCT), the electrooculogram (EOG), and the electroretinogram (ERG), may give additional information that will help to define a precise diagnosis. For example, an older individual with Best’s vitelliform macular dystrophy can present with an atrophic lesion of the macula involving marked loss of choriocapillaris or choroid. The EOG will disclose the subnormality of the slow oscillation of the resting potential of the eye that is characteristic of this disease.6,7,8 Males with X-linked juvenile retinoschisis may present with only marked macular atrophy as a result of long-standing foveomacular schisis. The ERG for these individuals will show the marked, selective loss of the scotopic b-wave of the ERG (the so-called electronegative ERG configuration) that is typical of this disorder.9,10 However, for most forms of choroidal atrophy or degeneration, accurate diagnosis depends not on electrophysiology alone but on the assimilation of information from history, fundus examination, visual fields, fluorescein angiograms, and other special tests, including plasma amino acids or tests on DNA for specific genetic mutations.
Examination of other family members who may be similarly affected is often crucial for recognition of the disorder in its earlier or more specific stage and for appreciation of the range of expression. For those individuals who do not have a family history of others similarly affected, valuable information can be obtained from previous examination records, especially if photographs were taken or other specific tests were performed. Often, examining other family members or obtaining old records is the only way to arrive at the correct diagnosis.
PRIMARY ATROPHIES
In this chapter, we will discuss briefly all primary atrophies or dystrophies that include significant choroidal atrophy in at least one stage of the disease. Primary atrophies that can lead to choroidal atrophy include primary choroidal atrophies, retinal degenerations (retinitis pigmentosa group), end-stage macular dystrophies, mutations of the peripherin/RDS gene, and disorders that cause angioid streaks, such as pseudoxanthoma elasticum.
PRIMARY CHOROIDAL ATROPHIES
Primary choroidal atrophies are those genetically determined degenerations that involve prominent choroidal atrophy at an early stage in the disease. Primary choroidal atrophies can be divided into regional choroidal atrophies and diffuse choroidal atrophies, which, in turn, can be further subdivided into choriocapillaris and total vascular choroidal atrophies, depending on whether the atrophy involves predominantly the choriocapillaris or the entire choroid.11
REGIONAL CHOROIDAL ATROPHIES
Regional Choriocapillaris Atrophies
CENTRAL AREOLAR CHOROIDAL DYSTROPHY (CENTRAL AREOLAR CHOROIDAL SCLEROSIS)
First described by Nettleship12 in 1884, central areolar choroidal dystrophy (CACD) (MIM No. 215500, Phenotype catalog number (MIM) from McKusick VA: Mendelian Inheritance in Man. Catalogs of Human Genes and Genetic Disorders. 12th ed. Baltimore: Johns Hopkins University Press, 1998 [http://www-ncbi-nlm-nih-gov.easyaccess1.lib.cuhk.edu.hk/Omim/]), as it is most appropriately called,13 has been described under many names, including central areolar choroidal sclerosis, central areolar choroidal atrophy, central angiosclerosis, and central senile choroiditis.14,15 The disorder can be autosomal dominant or autosomal recessive, and phenocopies can occur from many other diseases, including mutations of peripherin/RDS16,17,18,19 and advanced stages of macular dystrophies (see later text). A locus for CACD has been identified on chromosome 17p.20 The earliest symptoms result from pericentral scotomas and include difficulty reading, poor dark adaptation, reduced visual acuity, and glare sensitivity. The earliest fundus findings are subtle and include pigment epithelial and choriocapillaris lesions in the macula (Fig. 1A) that enlarge and eventually form the punched-out central atrophic lesions typical of this disease (Fig. 1B). Histopathology shows fibrotic scarring with absence of choriocapillaris, retinal pigment epithelium, and overlying photoreceptors in the affected areas.21 The Ganzfeld electroretinogram is usually normal early in the course but may become mildly to moderately abnormal for cone and rod responses late in the course of disease when extensive atrophy of the choroid and secondarily the pigment epithelium and neurosensory retina occurs. Recent studies using the multifocal ERG have indicated that the abnormality of retinal function extends beyond the borders of the visible atrophy and is consistent with presynaptic photoreceptor dysfunction.22 The EOG can be normal or mildly abnormal depending on the extent of associated retinal pigment epithelial dysfunction.
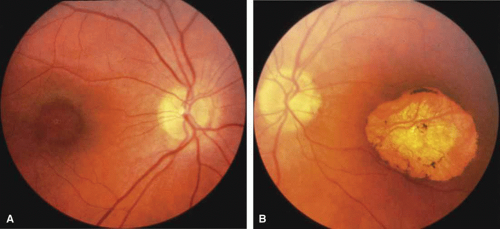 Fig. 1 A. Right eye of a 22-year-old woman with central areolar choroidal dystrophy in early stage showing discrete, oval macular lesion. Visual acuity was 20/100. B. Left eye of a 57-year-old woman (mother of patient shown in A) with typical large depigmented atrophic macular lesion. Visual acuity was 20/300. (From Carr RE: Central areolar choroidal dystrophy. Arch Ophthalmol 73:32, 1965) |
Other forms of central choroidal dystrophy exist that do not show the discrete oval lesions of typical central areolar choroidal sclerosis. These forms of central choroidal choriocapillaris atrophy often present with progressive pigment epithelial mottling and patchy choriocapillaris atrophy initially limited to the macula (Figs. 2A and 2B). With time, the atrophy enlarges and eventually encompasses the entire posterior pole (Fig. 2C). For this form of central choroidal atrophy, a gradual transition usually occurs from atrophic central pigment epithelium and choriocapillaris to essentially normal retina and choroid in the peripheral fundus.
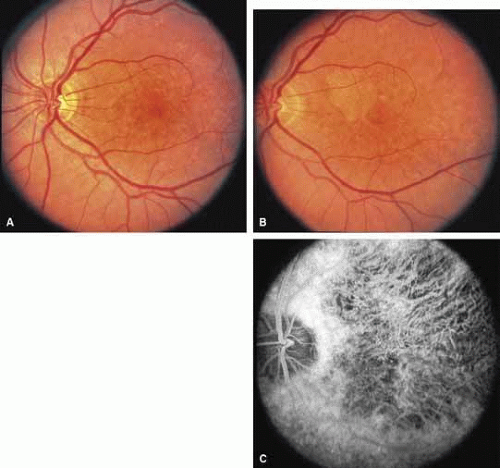 Fig. 2 Central choroidal dystrophy of a less discrete form than central areolar choroidal dystrophy, showing in early stages the focal pigment epithelial and choriocapillaris defects in a male at 30 years of age (A) and the subsequent progression evident at 45 years of age (B). C. Late stage of central choroidal dystrophy showing atrophic macular choroid in a 54-year-old woman (mother of patient shown in A and B). The father of the patient shown in C was similarly affected, suggesting autosomal dominant inheritance. |
BIETTI’S CRYSTALLINE DYSTROPHY
Bietti’s crystalline dystrophy (MIM No. 210370) of the cornea and retina is an autosomal recessive disorder that is characterized by the presence of crystals of unknown composition in the stroma of the peripheral cornea and at several layers of the retina (Figs. 3A and 3B).23 The disease can be subdivided into regional and diffuse forms, and the lack of any reports of the two patterns in the same family suggests genetic heterogeneity and not just variable expressivity.24,25 The regional form begins in midlife as pericentral scotomas that cause difficulty reading and reduced central visual acuity. Peripheral retinal function is retained and the electroretinogram and electrooculogram are normal or near normal even in moderately advanced disease. The fundus appearance and fluorescein angiogram reveal regional loss of pigment epithelium and choriocapillaris limited to the posterior pole (Figs. 3C and 3D). The finding of abnormal crystals in leukocytes indicates that this is a systemic metabolic disorder.24
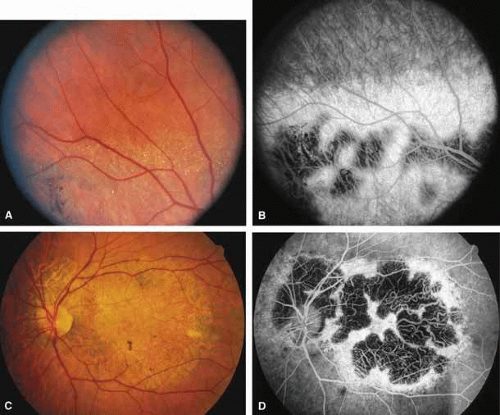 Fig. 3 Right fundus (A) and fluorescein angiogram (B) of 52-year-old man with regional form of Bietti’s crystalline corneal retinal dystrophy. Note retinal crystals adjacent to areas of dystrophy. Left fundus (C) and fluorescein angiogram (D) of 61-year-old brother of patient shown in A, showing marked regional atrophy of choroid and retina limited to the posterior pole and peripapillary regions. (A and B from Wilson DJ, Weleber RG, Klein ML, et al: Bietti’s crystalline dystrophy: A clinicopathologic correlative study. Arch Ophthalmol 107:213–221, 1989; Copyright 1989, American Medical Association) |
The diffuse form presents with loss of peripheral visual field, symptoms of poor night vision as well as reduced visual acuity, and diffuse loss of pigment epithelium and choriocapillaris on funduscopy (Fig. 4) and on fluorescein angiogram. The ERG is profoundly abnormal early in the course of the disease, and visual impairment eventually becomes much more severe in the diffuse than in the regional form of the disease.
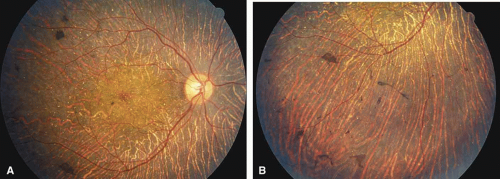 Fig. 4 Posterior pole (A) and inferior retina (B) of right eye of a 45-year-old woman with diffuse form of Bietti’s crystalline corneal retinal dystrophy, showing widespread atrophy (same patient as in reference 24). |
REGIONAL TOTAL VASCULAR CHOROIDAL ATROPHIES
Helicoidal peripapillary chorioretinal degeneration (also called atrophia areata and peripapillary chorioretinal degeneration, Iceland type). First described in Iceland by Sveinsson26 in 1939 as choroiditis areata and renamed as helicoidal peripapillary chorioretinal degeneration (MIM No. 108985),27,28 this autosomal dominant disorder is characterized by peripapillary tongue-shaped patches of total vascular choroidal atrophy that extend radially away from the disc. Signs of edema or inflammation have not been described, distinguishing this disorder from serpiginous choroidopathy. Brazitikos and Safran29 believe that the peculiar fundus lesions are the result of tearing and retraction of the retinal pigment epithelium, and possibly Bruch’s membrane, followed by atrophy of the choroid and retina. The areas of atrophy bear no relation to the pattern of the retinal vessels. The ERG suggests focal rather than diffuse retinal dysfunction initially at the level of the RPE and later affecting the sensory retina.30 Magnússon,31 who used the term atrophia areata, studied a large pedigree of 26 affected individuals in whom the disorder was inherited as an autosomal dominant trait (Fig. 5). Myopia and astigmatism were usually present, and the visual acuity was extremely poor in later years. Occasionally, the disorder has been called central gyrate atrophy, but this name should be discouraged because of the confusion with gyrate atrophy of the choroid and retina with hyperornithinemia. Serum amino acid levels are normal in helicoidal peripapillary chorioretinal degeneration.31
 Fig. 5 Fundi of a 24-year-old woman with helicoidal peripapillary chorioretinal degeneration. Ten years later, central vision was lost in the right eye. (From Magnússon L: Atrophia areata: A variant of peripapillary chorioretinal degeneration. Acta Ophthalmol 59:659, 1981) |
This clearly dominantly inherited disorder should not be confused with the nonfamilial condition called serpiginous choroidopathy, which has unfortunately been reported in the past (and in some reviews is still classified) under the name geographic helicoid peripapillary choroidopathy.32
PROGRESSIVE BIFOCAL CHORIORETINAL ATROPHY
Progressive bifocal chorioretinal atrophy is a rare autosomal dominant disorder mapped to chromosome 6q33,34 that was first described by Douglas, Waheed, and Wyse35 in a large Scottish family in 1968. Thirty-three of 91 family members were affected. The authors classified the disease into three stages (Fig. 6). Stage 1, which lasts from birth to age 14 years, involves a temporal focus of atrophy of retinal and choroidal tissue in the macula that continues to slowly enlarge with time. The upper, nasal, and lower edges of the temporal lesion are well defined, whereas the temporal edge is serrated and indistinct. Stage 2, which lasts from age 15 years to age 45 years, is associated with a second focus of atrophy nasal to the disc, hence the term bifocal in the name. At the end of this stage, the nasal focus is about three disc diameters in size. Stage 3, which occurs after 45 years of age, is associated with further expansion of the temporal and, especially, the nasal focus, leaving only a vertically oriented one- to two-disc-diameter swath or band of intact retina and choroid extending from the disc to each equator superiorly and inferiorly. Visual acuity was markedly subnormal compared with early years, but no patients lost all vision. All patients had coarse nystagmoid eye movements that precluded measurement of visual fields. Most patients were myopic. The ERG b-wave amplitude was subnormal but not unrecordable by a non-Ganzfeld single-flash technique.
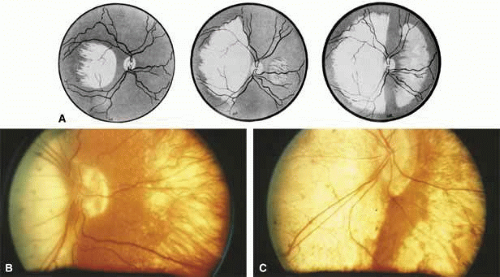 Fig. 6 A. Artist’s drawing of the three stages of progressive bifocal chorioretinal atrophy: Stage 1 (left), Stage 2 (center), and Stage 3 (right). B. Right eye of 17-year-old patient with late Stage 2, early Stage 3 disease. Visual acuity was 20/200. C. Right eye of older patient with Stage 3 disease. (From Douglas AA, Waheed I, Wyse CT: Progressive bifocal chorio-retinal atrophy: A rare familial disease of the eyes. Br J Ophthalmol 52:742, 1968) |
SORSBY’S FUNDUS DYSTROPHY
Sorsby’s fundus dystrophy (MIM No. 136900), previously called Sorsby’s pseudoinflammatory macular dystrophy, is a highly penetrant, autosomal dominantly inherited disorder characterized by a tritan color vision defect, drusen-like subretinal deposits, and pigment epithelial atrophy in younger individuals followed by choroidal neovascularization, hemorrhage, subretinal fibrosis, and choroidal atrophy in later years (Fig. 7).14,36,37,38 Loss of vision usually commences after the age of 50 years. The disease in late stages progresses to involve the peripheral retina. More recent studies of members of Sorsby’s original family demonstrated angioid streaks and yellow plaque-like subretinal deposits, features distinguishing this disorder from dominant drusen.39,40 Visual prognosis is poor because of the tendency of the disease process to involve the macula. The ERG is generally normal except in the most advanced stages when extensive areas of the retina are involved.41 Linkage studies assigned the gene for Sorsby’s dystrophy to 22q13-qter.42 Weber et al.43 found mutations in the gene for the tissue inhibitor of metalloproteinase-3 (TIMP3), which is located on the long arm of chromosome 22, in patients with Sorsby’s fundus dystrophy. This finding suggests that a defect in maintenance and renewal of Bruch’s membrane by the altered gene product is an important underlying pathologic event in Sorsby’s fundus dystrophy.
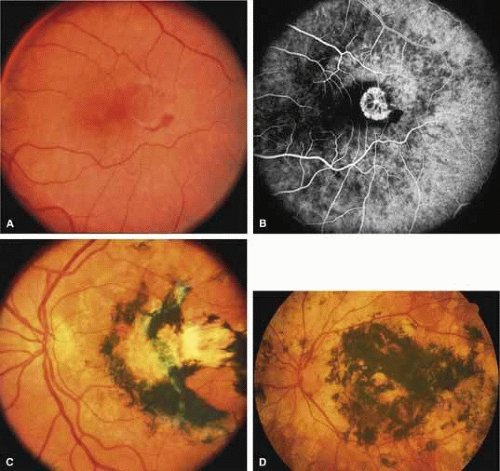 Fig. 7 Left fundus of a woman from a multigeneration family with Sorsby’s fundus dystrophy at 36 years of age (A, B) and at 40 years of age (C) demonstrating scarring from recurrent neovascularization and hemorrhage after laser photocoagulation. D. Untreated left eye of the 67-year-old mother of the patient in A through C. Visual acuity was counting fingers at 2 feet. (Illustrations courtesy of Michael L. Klein, M.D., Portland, OR) |
SERPIGINOUS CHOROIDOPATHY
Serpiginous choroidopathy, also called serpiginous choroiditis, is a recurrent, progressive, destructive chronic degeneration of the choroid and retinal pigment epithelium that begins around the optic nerve and extends through the posterior pole.44 Unfortunately, some cases of this disorder have been reported under the name geographic helicoid peripapillary choroidopathy, and this has led to confusion with the clearly dominantly inherited genetic disorder first described in Iceland by Sveinsson26 in 1939 as choroiditis areata and subsequently renamed helicoidal peripapillary chorioretinal degeneration.27,28 The etiology of serpiginous choroidopathy is unknown, but the disease is not thought to be genetic. The disease starts as a gray, cream, or greenish discoloration and edema of the retinal pigment epithelium, followed by extension of the lesion, usually away from the disc, in a stepwise fashion (Figs. 8A and 8B). Vitritis is present in one-third of cases. Periods of quiescence or activity can be separated by months to years. Subretinal fibrous scarring, atrophy of the choroid, and hyperpigmentation in adjacent tissues can be prominent features (Figs. 8C and 8D). The prognosis for retention of central vision is poor because the disease process will often involve the macula. Systemic immunosuppression may be effective in prolonging remission and improving the visual outcome.45
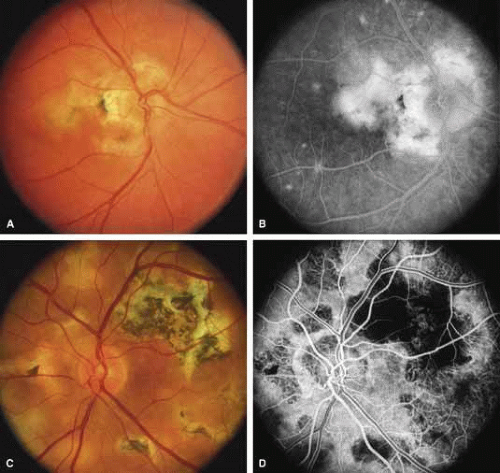 Fig. 8 Right fundus (A) and late-phase fluorescein angiogram (B) of a 35-year-old woman with serpiginous choroidopathy. The visual acuity was 20/200. Left fundus (C) and fluorescein angiogram (D) of a 47-year-old man with advanced serpiginous choroidopathy, demonstrating several stages of lesions and subretinal gliosis. Visual acuity was 14/400. (A and B courtesy of Michael L. Klein, M.D., Portland, OR) |
Although originally described as separate disorders, serpiginous choroidopathy and geographic choroidopathy are believed by most authors to be variations of a single disease process.32,46,47,48 Thus, there appear to be two distinct conditions only—serpiginous choroidopathy, which is an acquired nongenetic disorder, and helicoidal peripapillary chorioretinal degeneration (MIM No. 108985), which is a dominantly inherited disorder.
CENTRAL GYRATE ATROPHY
Some clinicians have used the term central gyrate atrophy as a label for the fundus appearance of marked total vascular choroidal atrophy in the posterior pole. Central gyrate atrophy appears to not be a distinct entity but probably represents the atrophic changes that can occur in the posterior pole in advanced malignant myopic degeneration, the end stage of serpiginous choroidopathy, or the end stage of helicoidal peripapillary chorioretinal degeneration. Use of the term central gyrate atrophy for such fundus appearances should be avoided because it leads to confusion with the metabolic disorder gyrate atrophy with hyperornithinemia.
DIFFUSE CHOROIDAL ATROPHIES
Diffuse choriocapillaris atrophies
DIFFUSE CHORIOCAPILLARIS ATROPHY
Diffuse choriocapillaris atrophy, also called diffuse choroidal sclerosis and diffuse choroidal angiosclerosis, can be inherited either as an autosomal dominant or, less commonly, as a recessive trait. Certain mutations of the peripherin/RDS gene have also been associated with diffuse choriocapillaris atrophy.18 The disorder is characterized by progressive thinning and loss of choriocapillaris beginning in midlife and resulting in severe loss of vision by later years (Fig. 9). Although the disease in most families is quite consistent among affected individuals, both diffuse and regional central choriocapillaris atrophy have been reported in the same family, suggesting that these two disorders are interrelated.11 Symptoms may include night blindness, loss of central vision, and loss of peripheral vision—the latter feature distinguishing this disorder from the regional form of central choriocapillaris atrophy. Fluorescein angiograms show thinned or absent choriocapillaris with prominent medium and large choroidal vessels throughout the retina. Eventually, mild pigment dispersion and clumping occur in the peripheral retina as the retinal pigment epithelium and overlying retina become affected, but the picture is still dominated by the atrophy of the choroid. The electroretinogram, except in the earliest stages, is usually severely abnormal and eventually becomes unrecordable. The EOG is abnormal early in the disease.
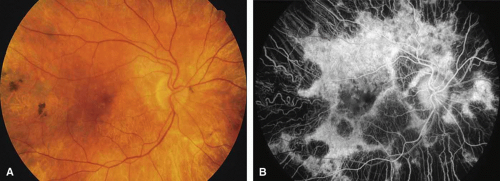 Fig. 9 Right fundus (A) and fluorescein angiogram (B) of a 65-year-old woman with diffuse choriocapillaris atrophy, showing widespread thinning of retinal pigment epithelium and loss of choriocapillaris. |
DIFFUSE TOTAL VASCULAR CHOROIDAL ATROPHIES
Gyrate atrophy of the choroid and retina with hyperornithinemia from ornithine aminotransferase deficiency. Gyrate atrophy of the choroid and retina (MIM No. 258870) is an autosomal recessive disease that is associated with a 10- to 20-fold elevation of plasma and tissue levels of ornithine.49,50,51,52 Vitamin B6 responsive and nonresponsive forms exist. Although the disease is found worldwide, the greatest number of patients, nearly 50% of those reported (all B6 nonresponsive), are of Finnish descent.52 In the first or second decade of life, patients experience night blindness and begin to develop irregular round areas of total vascular choroidal atrophy (Fig. 10A).50 These lesions enlarge and coalesce with time, forming extensive atrophy in the periphery that is associated with constriction of the peripheral visual field (Figs. 10B and 10C). The classic appearance of the fundus is that of a sharp transition from more normal retina to nearly complete atrophy of the choroid and retina (Figs. 11A and 11B).50,53 Central vision may be lost from cystoid macular edema, epiretinal proliferation, or macular involvement in the atrophic process (Figs. 11C and 11D).50 Many patients will develop clinically significant posterior subcapsular cataracts. The ERG and EOG are markedly abnormal from early in the course of the disease.54
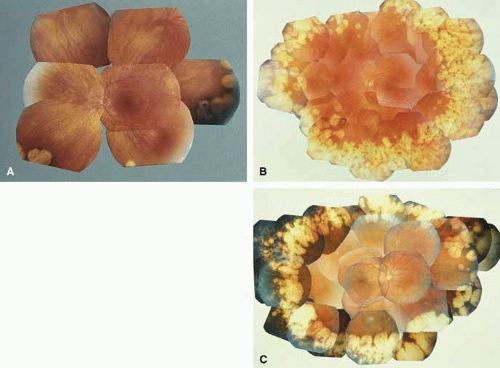 Fig. 10 A. Left eye of a 12-year-old girl with B6-nonresponsive gyrate atrophy of the choroid and retina. One allele of the ornithine aminotransferase gene was inactivated by a (TAC)Tyr299-TAG stop mutation in exon 8, whereas the other allele was inactivated by an Arg180Thr (AGG→ACG) mutation in exon 6 (patient 4 in reference 61). B. Left eye of a 30-year-old woman with B6-responsive gyrate atrophy. One allele of the ornithine aminotransferase gene was the Glu318Lys mutation (GAG → AAG mutation at codon 318 in exon 9), whereas the other allele was inactivated by a splice site mutation of intron 4.62 C. Right eye of a 40-year-old man with B6-nonresponsive gyrate atrophy, showing accumulation of dense, black pigment in the temporal periphery in region of choroidal atrophy. One allele was inactivated by a deletion within exon 6, whereas the other was inactivated by formation of a stop codon in exon 6 (TAT)Tyr209TAA.61 (A, B, and C from Weleber RG, Kennaway NG: Gyrate atrophy of the choroid and retina. In Heckenlively JR [ed]: Retinitis Pigmentosa. Philadelphia: JB Lippincott, 1988:198–220) |
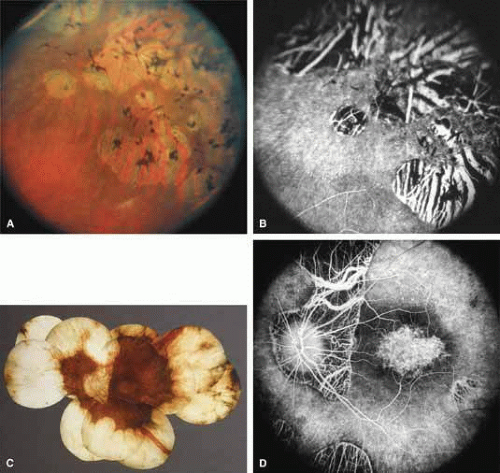 Fig. 11 A. Transition zone between atrophic and more intact midperipheral retina in 37-year-old patient with B6-responsive gyrate atrophy. One allele is the Glu318Lys mutation of the ornithine aminotransferase gene, but the mutation affecting the other allele has yet to be defined (Inana G, Weleber RG, personal communication). B. Fluorescein angiogram of same region, showing pigment epithelial window defects and loss of choriocapillaris. C. Left fundus (C) and fluorescein angiogram (D) of advanced gyrate atrophy associated with macular atrophy in a 64-year-old woman homozygous for the most common Finnish mutation, the Leu402Pro mutation of exon 11 of the ornithine aminotransferase gene (Inana G, Weleber RG, unpublished finding). (B from Weleber RG, Kennaway NG: Gyrate atrophy of the choroid and retina. In Heckenlively JR [ed]: Retinitis Pigmentosa. Philadelphia: JB Lippincott, 1988:198–220. Images C and D courtesy of Robert Kalina, M.D., Seattle, WA) |
The underlying defect of gyrate atrophy involves ornithine aminotransferase (OAT), which is a mitochondrial matrix enzyme that is pyridoxal phosphate dependent. The OAT gene is located at chromosome 10q26. Although the majority of patients have the form of gyrate atrophy that does not respond to vitamin B6 or pyridoxine, some individuals (less than 5%) show partial vitamin B6 responsiveness. This is shown in vitro by an increase in enzyme activity when assayed with additional pyridoxine and in vivo with a 50% reduction of plasma ornithine levels with oral vitamin B6 supplementation.55,56 Histologic abnormalities occur also in muscle (subsarcolemmal deposits in type II muscle fibers) and other tissues (abnormal-appearing mitochondria in liver and iris).57,58,59 However, the predominant pathology and clinical symptoms occur in the choroid and retina (see elsewhere in these volumes).50,52 The exact mechanism of pathology for the ocular lesions in gyrate atrophy is unknown, but the three major theories are that, secondary to the OAT deficiency: (1) intracellular proline in the retina may be deficient; (2) creatine phosphate stores in the retina and choroid may be deficient, leading to cell dysfunction and cell death; and/or (3) elevated levels of ornithine may be toxic to the retinal pigment epithelium.60 The abnormal muscle inclusions appear to be the result of deficiency of creatine phosphate, but the role of creatine phosphate as an energy store in the eye is currently undefined.
The molecular basis of ornithine aminotransferase deficiency has been defined for many patients with gyrate atrophy.61,62,63,64,65,66,67,68 Two mutations of the OAT gene (Leu402-Pro and Arg180Thr) account for nearly all of the Finnish patients with nonpyridoxine-responsive gyrate atrophy.66 Loss of gene function occurs from deletions, insertions, splice site base-pair changes, and missense mutations. The rare pyridoxine-responsive patients with gyrate atrophy are homozygous for the Glu318SLys mutation or heterozygous for either the Val332Met mutation or the Glu318Lys mutation of the OAT gene, with the other allele inactivated by another mutation that may or may not be pyridoxine responsive.62,63,69
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


