55 Deep Neck Space Infection • Retropharynx • Parapharyngeal • Anterior deep neck • Fascial layers: – Superficial: investing – Middle: visceral – Deep: prevertebral, alar • Spaces * All 3 contribute to carotid sheath • 2nd most common neck abscess in children (peritonsillar abscess/quinsy most common) • Retropharyngeal lymph nodes atrophy with age • Aetiology: • Presentation: • Management: • Ludwig angina; floor of mouth cellulitis • Anatomy Fig. 55.1 Retropharyngeal abscess. • Features • Aetiology • Management – Sublingual space only—intra-oral – Submaxillary space—external • Anatomy • Presentation • Aetiology • Treatment
55.1 Sites
55.2 Anatomy
 Fascial compartments are potential spaces between fascial planes
Fascial compartments are potential spaces between fascial planes
 Superficial and deep layers
Superficial and deep layers
 Deep,* divided into:
Deep,* divided into:
 See Table 55.1
See Table 55.1
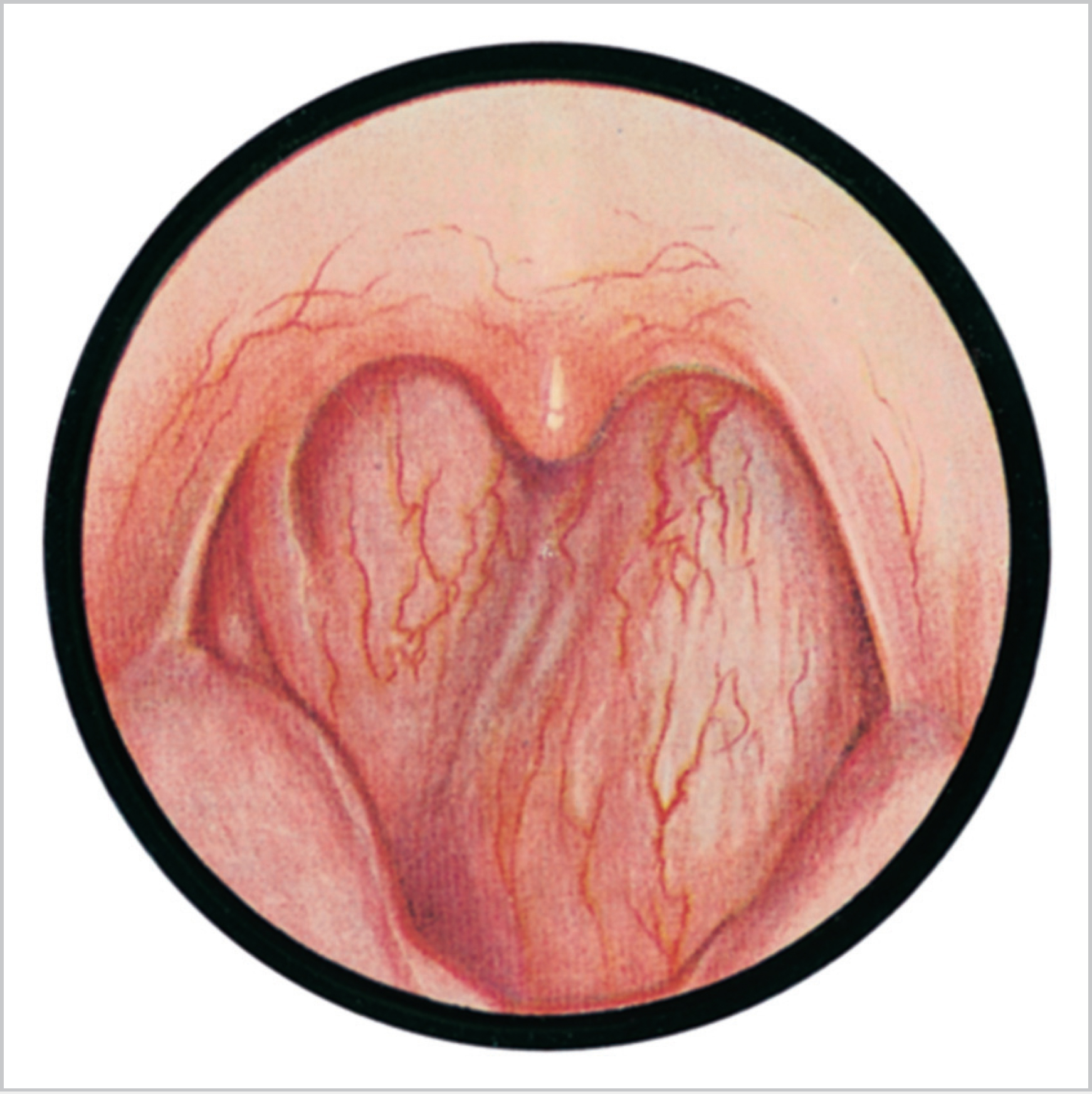
55.3 Retropharyngeal Abscess (Fig. 55.1)
 Suppurative adenoiditis
Suppurative adenoiditis
 Trauma
Trauma
 Vertebral osteomyelitis
Vertebral osteomyelitis
 Pyrexia*
Pyrexia*
 Neck pain*
Neck pain*
 Airway obstruction
Airway obstruction
 Drooling
Drooling
 Torticollis
Torticollis
 Age of presentation is typically 6 months to 6 years (mean 3–5 years)
Age of presentation is typically 6 months to 6 years (mean 3–5 years)
 Airway is the priority
Airway is the priority
 Transoral aspiration/drainage if abscess medial to great vessels unless other neck spaces involved
Transoral aspiration/drainage if abscess medial to great vessels unless other neck spaces involved
 Specimen pus urgent Gram stain and culture and sensitivity and abscess wall
Specimen pus urgent Gram stain and culture and sensitivity and abscess wall
 Intravenous antibiotics (discuss with microbiology common regimes include: clindamycin/piperacillin or penicillin/gentamicin + metronidazole) ± steroids
Intravenous antibiotics (discuss with microbiology common regimes include: clindamycin/piperacillin or penicillin/gentamicin + metronidazole) ± steroids
55.4 Anterior Deep Neck

 Submandibular space extends from hyoid to mandible divided by mylohyoid muscle
Submandibular space extends from hyoid to mandible divided by mylohyoid muscle
 Sublingual space superior to muscle
Sublingual space superior to muscle
 Submaxillary space inferior
Submaxillary space inferior
 Mouth pain
Mouth pain
 Drooling
Drooling
 Dysphagia
Dysphagia
 Neck pain
Neck pain
 Swelling in floor of mouth
Swelling in floor of mouth
 Superior tongue displacement
Superior tongue displacement
 80% dental—typically lower 3rd molar
80% dental—typically lower 3rd molar
 20% soft tissue/tonsil infection
20% soft tissue/tonsil infection
 Airway is priority consider HDU for observation
Airway is priority consider HDU for observation
 Timely surgical intervention with appropriate IV ABx
Timely surgical intervention with appropriate IV ABx
 Surgical drainage
Surgical drainage
55.5 Parapharyngeal Abscess
 Parapharyngeal space 2 compartments: pre- (anterior) and post-styloid
Parapharyngeal space 2 compartments: pre- (anterior) and post-styloid
 Communicates anterior with submaxillary space via buccopharyngeal gap created by styloglossus
Communicates anterior with submaxillary space via buccopharyngeal gap created by styloglossus
 Communicates posteriorly with the retropharyngeal and danger spaces
Communicates posteriorly with the retropharyngeal and danger spaces
 Airway obstruction—stridor/stertor
Airway obstruction—stridor/stertor
 Pain
Pain
 Dysphagia/dysphonia
Dysphagia/dysphonia
 Trismus (20%)
Trismus (20%)
 Snoring/OSA
Snoring/OSA
 Neck swelling/fullness/increasing erythema
Neck swelling/fullness/increasing erythema
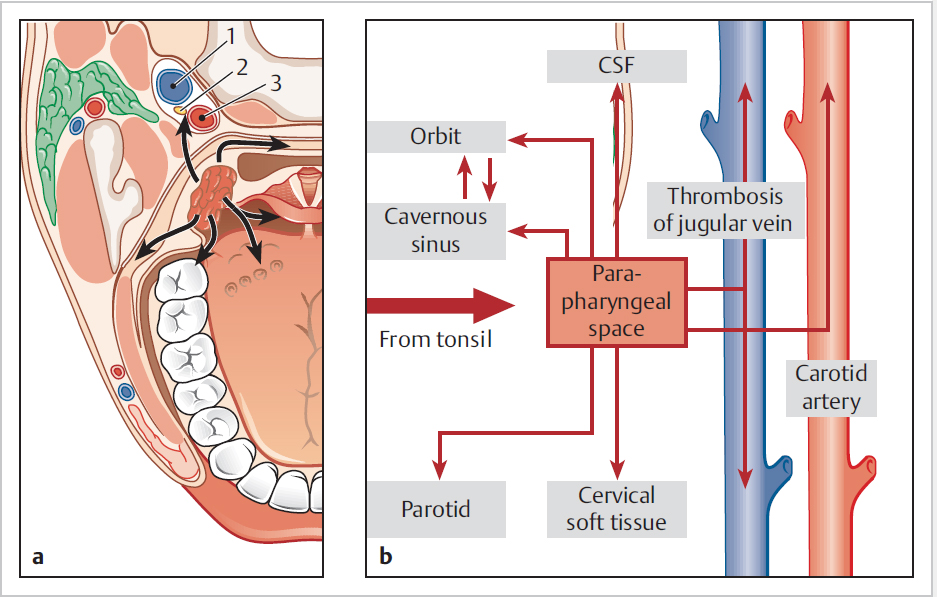
 Tonsillitis (particularly immunocompromised) (Fig. 55.2)
Tonsillitis (particularly immunocompromised) (Fig. 55.2)
 Dental
Dental
 IV drug abusers
IV drug abusers
 Epiglottitis
Epiglottitis
 Parotitis
Parotitis
 Foreign body
Foreign body
 Branchial cleft cysts (if recur)
Branchial cleft cysts (if recur)
 Extension from petrous apex/mastoid tip (Citelli abscess)
Extension from petrous apex/mastoid tip (Citelli abscess)
 Ensure airway stable, may need tracheostomy
Ensure airway stable, may need tracheostomy
 May require ICU admission
May require ICU admission
 Preop CT scan for surgical planning (if airway stable), and cardiothoracic referral if mediastinum involved
Preop CT scan for surgical planning (if airway stable), and cardiothoracic referral if mediastinum involved
 Incision guided by imaging and clinical examination
Incision guided by imaging and clinical examination
 Urgent microbiology inc. Gram stain and culture
Urgent microbiology inc. Gram stain and culture
 Multiple neck spaces may need opening, finger dissection useful at breaking down loculations and entering planes
Multiple neck spaces may need opening, finger dissection useful at breaking down loculations and entering planes
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


