Deep Neck Infections
Behrad B. Aynehchi
Gady Har-El
Deep neck space infections (DNSIs) are a relatively infrequent entity in the postpenicillin era. Their occurrence, however, poses considerable challenges in diagnosis and treatment and they may result in potentially serious or even fatal complications in the absence of timely recognition. The advent of antibiotics has led to a continuing evolution in etiology, presentation, clinical course, and antimicrobial resistance patterns. These trends combined with the complex anatomy of the head and neck underscore the importance of clinical suspicion and thorough diagnostic evaluation. Proper management of a recognized DNSI begins with securing the airway. Despite recent advances in imaging and conservative medical management, surgical drainage remains a mainstay in the treatment in many cases.
ETIOLOGY
Knowledge of the portal of entry enables the surgeon to anticipate the pathway of extension within the neck, potential complications, and sites for drainage. In the preantibiotic era, the majority of deep neck infections in adults and children originated from the tonsils and pharynx, most commonly leading to parapharyngeal space infections (1). Acute rhinosinusitis in children may also cause retropharyngeal lymphadenitis. Suppuration of these inflamed nodes can eventually culminate in abscess formation. Early administration of antimicrobials in adult patients has led to a decreased incidence of upper respiratory tract infections and consequently significantly fewer DNSIs originating from this site. This trend has given way to infections of odontogenic sources becoming the primary source of deep neck infection in adults, recognizing a strong association with poor oral hygiene and lower socioeconomic status (2). Additional but less common origins of deep neck infections include salivary gland infections, penetrating trauma, surgical instrument trauma, spread from superficial infections, necrotic malignant nodes, mastoiditis with resultant Bezold’s abscess, and unknown causes (3,4,5). In inner cities, where intravenous drug abuse (IVDA) is more common, there is a higher prevalence of infections of the jugular vein and carotid sheath from contaminated needles (6,7,8). The emerging practice of “shotgunning” crack cocaine has been associated with retropharyngeal abscesses as well (9). These purulent collections from direct inoculation, however, seem to have a more benign clinical course compared to those spreading from inflamed tissue (10). Congenital anomalies including thyroglossal duct cysts and branchial cleft anomalies must also be considered, particularly in cases where no apparent source can be readily identified. Regardless of the etiology, infection and inflammation can spread throughout the various regions via arteries, veins, lymphatics, or direct extension along fascial planes. When confined to a certain area or space, this inflammatory process will eventually form a phlegmon or abscess.
FASCIAL ORGANIZATION OF THE DEEP NECK
An understanding of the applied anatomy of the neck includes a consideration of the layers of the deep cervical fascia and the compartments or spaces formed by the arrangement and attachments of these layers. This knowledge is crucial for planning treatment strategies and anticipating potential complications. The cervical fascia is divided into the superficial and deep fascia. The deep fascia is further subdivided into three layers or components: the superficial, middle, and deep. A summary of the organization of the cervical fascia is presented in Table 55.1. Figure 55.1 features a midsagittal visualization of the fascia and deep neck spaces.
TABLE 55.1 CLASSIFICATION OF FASCIA IN THE NECK | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
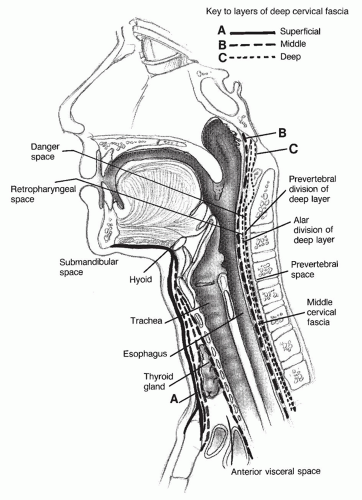 Figure 55.1 Midsagittal section of the neck shows the fascia and spaces of the neck. |
Superficial Cervical Fascia
The superficial cervical fascia lies beneath the skin of the head and neck, extending from the top of the head down to the shoulders, axilla, and thorax. This layer covers adipose tissue, sensory nerves, superficial vessels, lymphatics, the platysma muscle, and the muscles of facial expression. The platysma is absent in the midline. In contrast to the deep cervical fascia, which is composed of mainly fibrous connective tissue, the superficial cervical fascia is a layer of fibrofatty tissue connecting the overlying skin to the deeper fascial layers. Infections of this superficial space should be managed with appropriate antibiotic therapy in the case of cellulitis or extended to incision and drainage in the presence of an abscess (11).
Deep Cervical Fascia
As noted earlier, the deep cervical fascia is a fibrous connective tissue layer that is, for surgical purposes, subdivided into the superficial, middle, and deep components. The appropriate designation for each layer is as follows: the superficial layer of the deep cervical fascia, the middle layer of the deep cervical fascia, and the deep layer of the deep cervical fascia. A practical observation is that layers overlying nonexpansile components such as the sternocleidomastoid muscle (SCM) are well-developed membranes that can be sutured. On the other hand, fascia surrounding expansile visceral organs such as the pharynx and cheeks is a loose areolar tissue, not amenable to suture retention. Additionally, muscles and organs within these layers are generally free to glide upon contraction and relaxation.
The superficial layer of the deep cervical fascia, also referred to as the investing layer, completely surrounds the neck. The superior nuchal line, ligamentum nuchae of the cervical vertebrae, and the mastoid process are the posterior attachments. The fascia splits to envelope the sternocleidomastoid and trapezius muscles as it courses anteriorly. In the anterosuperior direction, an attachment is made to the inferior zygomatic arch. Moving inferiorly, the parotid gland is enveloped superficially, while the deep extent involves the carotid canal of the temporal bone. The stylomandibular ligament, which separates the parotid and submandibular glands, is formed as this investing fascia tracks anteriorly to cover the submandibular gland and muscles of mastication. The inferior extent includes attachments to the hyoid, acromion, clavicle, and scapular spine. The suprasternal space of Burns is formed as the fascia surrounds the intermediate tendon of the omohyoid muscle. This space may contain a lymph node along with a vessel bridging the two anterior jugular veins (12). A useful tool in understanding the contents of this plane is the “rule of two’s,” referring to the two muscles above the hyoid bone (masseter and anterior belly of the digastrics), two muscles that cross the neck (trapezius and SCM), two salivary glands (parotid and submandibular), and two fascial compartments (parotid and masticator spaces) (11).
The middle layer of the deep cervical fascia, also called the visceral fascia, is divided into a muscular and visceral division. The muscular division of the middle layer of the deep cervical fascia surrounds the sternohyoid, sternothyroid, thyrohyoid, and omohyoid strap muscles. Contents of the visceral division include the parathyroid glands, thyroid gland, esophagus, trachea, larynx, pharyngeal constrictor muscles, and buccinator muscle. This visceral division further contributes to two additional planes: the pretracheal fascia and buccopharyngeal fascia. The pretracheal fascia overlies the trachea. The buccopharyngeal fascia lies posterior to and separates the esophagus from the deep layer of the deep cervical fascia. This plane also marks the anterior border of the retropharyngeal space. The buccinators, pharyngeal constrictor muscles, and esophagus lie between the pharyngobasilar fascia anteriorly and the buccopharyngeal fascia posteriorly (12). The two raphes formed by the buccopharyngeal fascia include the posterior midline raphe, which attaches to the alar layer of the deep layer of the deep cervical fascia, and the pterygomandibular raphe within the lateral pharynx (11). Portions of the middle layer of the deep cervical fascia that surround the trachea and esophagus merge with the fibrous pericardium in the superior mediastinum, representing a possible portal of spread of infection.
The deep layer of the deep cervical fascia, also known as the prevertebral fascia, is composed of two divisions as well: the prevertebral and alar divisions. The prevertebral division contains the cervical vertebra, phrenic nerve, and paraspinous muscles. This fascia runs from the skull base to the coccyx, forming the anterior wall of the prevertebral space, with lateral and posterior attachments to the transverse spinous processes, respectively. The clinical significance of this boundary is the confinement of primary vertebral infections to the prevertebral space with very limited spread to the danger space. The alar division is situated between the prevertebral division posteriorly and the buccopharyngeal fascia of the visceral division of the middle layer of the deep cervical fascia anteriorly, separating the retropharyngeal and danger spaces. This layer extends from the skull base to the second thoracic vertebra. The notable structure within this plane is the cervical sympathetic trunk. In reviewing the deep fascial and special relationships within the neck, the following structures are encountered as one goes from anterior to posterior: the pharyngobasilar fascia, the esophageal or constrictor musculature, the buccopharyngeal fascia of the visceral division of the middle layer of the deep cervical fascia, the retropharyngeal space, the alar division of the deep layer of the deep cervical fascia, the danger space, the prevertebral division of the deep layer of the deep cervical fascia, the prevertebral space, and finally the vertebral body (12).
The carotid sheath is formed by contributions of all three layers of the deep cervical fascia, extending from the skull base to the thorax. Contents of this sheath include the common carotid artery, internal jugular vein (IJV), vagus nerve, and ansa cervicalis (11).
DEEP NECK SPACE ANATOMY
The above-mentioned planes of the deep cervical fascia form various real and potential spaces within the neck. These spaces though are not completely impermeable often communicate with each other in generally predictable routes. Strong fascial connections to the hyoid bone anteriorly that may function as a barrier to the inferior spread of infection have led to the classification of these spaces based on their relationship to this landmark. The spaces will be described as those involving the entire neck (retropharyngeal space, danger space, prevertebral space, and carotid space), those that lie above the hyoid bone (parapharyngeal space,
submandibular space, sublingual space, parotid space, masticator space, peritonsillar space, and temporal space), and those that lie below the hyoid bone (anterior visceral space and suprasternal space). Table 55.2 outlines the classification of the aforementioned spaces.
submandibular space, sublingual space, parotid space, masticator space, peritonsillar space, and temporal space), and those that lie below the hyoid bone (anterior visceral space and suprasternal space). Table 55.2 outlines the classification of the aforementioned spaces.
TABLE 55.2 DEEP NECK SPACES | |||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||
Spaces Involving the Entire Neck
Retropharyngeal Space
The retropharyngeal space extends from the skull base to the tracheal bifurcation in the superior mediastinum (Figs. 55.2, 55.3, 55.4). The space is medial to the carotid sheath, anterior to the danger space, and posterior to the buccopharyngeal fascia of the visceral division of the middle layer of the deep cervical fascia. The nodes of Rouviere reside within this space and may cause abscess formation upon drainage from the paranasal sinuses or nasopharynx, especially in children. A midline raphe connecting the alar division of the deep layer of the deep cervical fascia to the buccopharyngeal fascia accounts the off-midline presentation of infections within this space, facilitating distinction from disease processes originating within the danger and prevertebral spaces, which generally lie in the midline. Routes of direct spread are mainly from the parapharyngeal space (12).
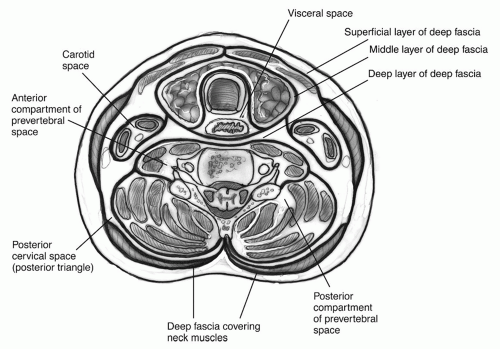 Figure 55.2 Cross section of the neck at the thyroid level. |
Danger Space
The danger space is flanked by the prevertebral and retropharyngeal spaces, extending from the skull base to the level of the diaphragm with minimal resistance (hence the name). It is bordered laterally by the transverse processes of the vertebrae (Fig. 55.4). The most noteworthy structure within this space is the cervical sympathetic trunk. Common sources of infectious spread are from the retropharyngeal, parapharyngeal, and prevertebral spaces (12).
Prevertebral Space
This space runs from the skull base to down to the coccyx, bordered by the vertebral bodies posteriorly, danger space anteriorly, and transverse processes laterally (Fig. 55.4). The dense areolar tissue within this space is in contrast to the loose counterpart found within the danger space. The main neurovascular constituents include the vertebral
vessels, phrenic nerve, and brachial plexus. The paraspinous, prevertebral, and scalene muscles are located within this space as well. Direct extensions of infection are from the vertebrae (e.g., Pott’s abscess) or penetrating injuries (12).
vessels, phrenic nerve, and brachial plexus. The paraspinous, prevertebral, and scalene muscles are located within this space as well. Direct extensions of infection are from the vertebrae (e.g., Pott’s abscess) or penetrating injuries (12).
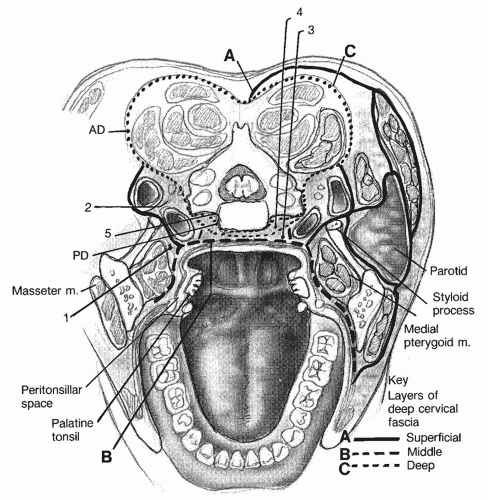 Figure 55.3 Cross section of the neck at the level of the oropharynx shows the anatomic relations of the deep neck spaces. 1, parapharyngeal space; 2, carotid space; 3, retropharyngeal space; 4, danger space; 5, prevertebral space; AD, alar division of deep layer; PD, prevertebral division of deep layer. |
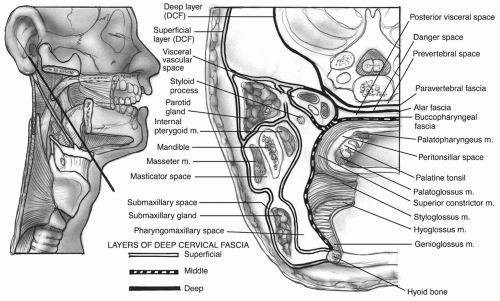 Figure 55.4 Oblique section through the neck shows the anatomic relations of the spaces limited to above the hyoid bone to the spaces that transverse the entire neck. The important relation between the parapharyngeal (pharyngomaxillary) space and the other spaces is evident. |
Carotid Space
Also referred to as the visceral vascular space, this is a potential space enclosed by the carotid sheath extending from the skull base to the thorax (Fig. 55.4). Its contents include the carotid artery, IJV, vagus nerve (cranial nerve X), and sympathetic plexus. Spread is generally from the adjacent parapharyngeal space, penetrating trauma, or IVDA (12).
Spaces above the Hyoid Bone
Parapharyngeal Space
Also known as the lateral pharyngeal, peripharyngeal, or pharyngomaxillary space (Figs. 55.3, 55.4, 55.5). This has classically been described as an inverted pyramid with the base at the skull base superiorly, and the apex at the greater cornu of the hyoid bone inferiorly. The lateral borders are the lateral pterygoid muscle, mandible, and parotid gland. The medial boundaries include the superior constrictor and levator and tensor veli palatini muscles, all enveloped by the middle layer of the deep cervical fascia. It lies posterior to the medial pterygoid muscle (where involvement will result in trismus) and pterygomandibular raphe, and anterior to the prevertebral fascia. This space is further split into the prestyloid and poststyloid compartments by the styloid process, which are anterior and posterior to this landmark, respectively. The poststyloid compartment houses neurovascular structures including: cranial nerves IX, X, XI, XII, the sympathetic chain, the carotid artery, and the IJV. The prestyloid compartment contains fatty tissue, the styloglossus and stylopharyngeus muscles, the deep lobe of the parotid gland, and lymph nodes. Several notable neurovascular structures course through this compartment as well: the internal maxillary artery; and the auriculotemporal, lingual, and inferior alveolar nerves. The parapharyngeal space serves as a hub for infectious spread from several deep neck spaces. The carotid space travels through the parapharyngeal space en route to the mediastinum. Lateral spread of infection will communicate with the masticator space, inferior spread will reach the submandibular space, and posteromedial extension appears in the retropharyngeal space (12).
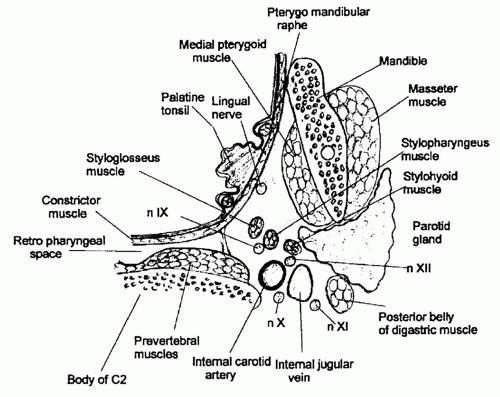 Figure 55.5 Schematic representation of the parapharyngeal space in an axial view at the C2 level. |
Submandibular and Sublingual Spaces
These two spaces communicate freely, and are hence presented together. It should be noted though that the terms submandibular or submaxillary space are commonly utilized in describing the combined submandibular and sublingual spaces. The superior border of these spaces is the mucosa of the floor of the mouth. They are limited by the hyoid bone posteroinferiorly, the mandible anteriorly and laterally, and the base of tongue posteriorly. The submandibular and sublingual spaces themselves are separated by the mylohyoid muscle, with the prior lying below and the latter lying above this landmark. Both spaces, however, communicate around the posterior edge of this muscle. It is for this reason that Ludwig’s angina will result in a generalized swelling of the submandibular area along with elevation of the floor of the mouth. While underlying the mylohyoid, the submandibular space is further separated
from (but also freely communicates with) the submental space by the anterior belly of the digastric muscle. The sublingual space houses the hypoglossal nerve, the sublingual salivary gland, and Wharton duct. The submandibular gland sits in both the sublingual and submandibular spaces as it straddles the posterior edge of the mylohyoid muscle. The mylohyoid line is an oblique line along the mandible that aids in the evaluation of submandibular or sublingual space infections from odontogenic sources. The incisors to first molars lie above this line. Infections originating in the roots of these teeth generally present initially in the sublingual space. On the other hand, the second and third molars are situated below the mylohyoid line, with infectious processes of these tooth roots draining primarily to the submandibular or parapharyngeal space (12).
from (but also freely communicates with) the submental space by the anterior belly of the digastric muscle. The sublingual space houses the hypoglossal nerve, the sublingual salivary gland, and Wharton duct. The submandibular gland sits in both the sublingual and submandibular spaces as it straddles the posterior edge of the mylohyoid muscle. The mylohyoid line is an oblique line along the mandible that aids in the evaluation of submandibular or sublingual space infections from odontogenic sources. The incisors to first molars lie above this line. Infections originating in the roots of these teeth generally present initially in the sublingual space. On the other hand, the second and third molars are situated below the mylohyoid line, with infectious processes of these tooth roots draining primarily to the submandibular or parapharyngeal space (12).
Parotid Space
This space, also known as the parotidomasseteric space, is created as the superficial layer of the deep cervical fascia envelopes the parotid gland, periparotid lymph nodes, facial nerve, posterior facial veins, and external carotid artery (Fig. 55.4). The fascia adheres tightly to the gland laterally. The resultant firm capsule deems differentiation of an abscess versus cellulitis within this space virtually impossible on physical examination, despite the relatively superficial location. In contrast, deficiency of the fascia along the medial border allows for communication of the gland with the prestyloid parapharyngeal space (12).
Masticator Space
This space is also formed by an investment of the superficial layer of the deep cervical fascia (Fig. 55.4). Its contents include the masseter, medial and lateral pterygoid muscles, body and ramus of the mandible, inferior alveolar vessels and nerves, buccal fat pad, and temporalis tendon. The masticator space may be divided into the masseteric space, between the mandibular ramus and masseter muscle; and the pterygoid space, between the mandibular ramus and pterygoid muscles. The masticator space is situated anterolateral to the parapharyngeal space and deep to the temporal space. Infections of this space are primarily from the third mandibular molar (12).
Peritonsillar Space
The peritonsillar space is sandwiched between the palatine tonsillar capsule medially, and the superior pharyngeal constrictor muscle laterally (Fig. 55.4). The anterior and posterior limits are formed by the palatoglossus and palatopharyngeus muscles or anterior and posterior pillars, respectively. The posterior third of the tongue serves as the inferior boundary. Delayed drainage of purulent collections from this space may result in parapharyngeal space extension (12).
Temporal Space
The temporal space is enclosed by the squamous temporal bone medially and the superficial temporalis fascia laterally. This space is further split into superficial and deep components by the temporalis muscle. Notable contents include the internal maxillary artery and the third division of the trigeminal nerve (V3) (12).
Spaces below the Hyoid Bone
Anterior Visceral Space
This space runs from the thyroid cartilage down to the level of the fourth thoracic vertebra (Fig. 55.2). The pharynx, esophagus, trachea, thyroid and parathyroid glands are the most notable components, all enclosed by the visceral division of the middle layer of the deep cervical fascia and nested behind the strap muscles. The most common portals of infection into this space include perforation of the anterior esophageal wall by trauma, foreign bodies, and endoscopic instrumentation (12).
Suprasternal Space
This is a potential space that sits just above the sternal notch, enveloped by the superficial layer of the deep cervical fascia. The suprasternal space of Burns features a small lymph node and bridging vessels between the anterior jugular veins (12).
BACTERIOLOGY
During the preantibiotic era, the organism most often isolated from deep neck space abscesses was Staphylococcus aureus. Since the introduction of antibiotics, aerobic Streptococcal species and non-Streptococcal anaerobes have become the chief offending agents in DNSIs. Most infections, however, are polymicrobial (13,14). These organisms generally represent members of oral flora, reflecting the most common site of origin: odontogenic infections. Practically speaking though, the organisms isolated will vary with the initial portal of entry. Notable aerobic species include Streptococcus viridans, Streptococcus pyogenes, Staphylococcus epidermis, and S. aureus (14,15). Two important relationships are that of S. viridans, S. pyogenes, and S. aureus with IVDA and S. aureus with infants. Methicillinresistant Staphylococcus aureus (MRSA) has been increasingly associated with IVDA, infants, and immunocompromised patients as well (16,17,18,19,20,21,22). Currently, the most frequently isolated anaerobes include Peptostreptococcus, Fusobacterium, and Bacteriodes (6,14,19,23), though their overall prevalence is likely underestimated in most reports due to difficulty in culture growth. Production of beta-lactamase has led to the growing resistance of anaerobic agents to penicillin (23,24). Eikenella corrodens is increasingly found in head and neck infections, bringing with it a very clinically relevant resistance to clindamycin and metronidazole.
Gram-negative rods, such as Haemophilus, Escherichia, Pseudomonas, and Neisseria, are usually only seen in hospitalized, debilitated, or immunocompromised patients (3). Klebsiella pneumoniae is found to have a predilection for poorly controlled diabetics. Atypical and granulomatous
organisms, including Actinomyces, tuberculous and nontuberculous mycobacteria, cat scratch or Bartonella henselae, and tularemia (25,26), are seen far less frequently.
organisms, including Actinomyces, tuberculous and nontuberculous mycobacteria, cat scratch or Bartonella henselae, and tularemia (25,26), are seen far less frequently.
DIAGNOSIS
History, physical examination, laboratory tests, and diagnostic imaging yield vital information in diagnosing and managing patients with DNSIs. The first priority, however, is expedient and aggressive management of potential respiratory compromise. Upon confirmation or achievement of a secure airway, a comprehensive and careful evaluation is necessary in elucidating possible sources of infection in order to direct optimal therapeutic approaches. It is also important to note that many patients presenting to an otolaryngologist with a possible DNSI have already been placed on an outpatient antibiotic regimen, possibly altering the typical presenting symptoms and findings, underscoring the importance of a thorough evaluation (1,27).
History and Physical Examination
As with any disease process, a thorough history of the present illness must be solicited. This starts with a survey of symptom onset, intensity, duration, and any systemic inflammatory symptoms and signs such as pain, fever, swelling, malaise, fatigue, or redness. Localizing complaints of dyspnea, odynophagia, dysphagia, voice changes, drooling, trismus, and otalgia direct the clinician toward a possible site of infection (13,28,29,30




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
