Cytomegalovirus Retinitis
Tamara R. Vrabec MD1
Caroline R. Baumal MD2
2 Tufts University, Boston, MA, cbaumal@tufts-nemc.org
1 Geisinger Medical Center, 100 North Academy Avenue, Danville, PA 17822-2120, tvrunning@aol.com, 570 271 6531
Introduction
Before 1982, cytomegalovirus retinitis (CMVR)was a disease so extraordinarily rare that few ophthalmologists ever observed a case. (1) However, during the acquired immunodeficiency syndrome (AIDS) pandemic, CMV (CMV) emerged as a common cause of infectious retinitis worldwide.
In the late 1990s, the introduction of highly active antiretroviral therapy (HAART) revolutionized the therapeutic approach to and clinical course of AIDS. By inhibiting cleavage and maturation of the human immunodeficiency virus (HIV), the combination of protease inhibitors employed in HAART resulted in both a significant and sustained reduction in HIV viral load and a consequent improvement in CD4+ T cell count and function. (2) Repopulation of CD4+ clones active against opportunistic organisms facilitated remission of opportunistic infections including CMVR and prolonged survival in many patients.
Yet, in spite of HAART, the AIDS pandemic is growing worldwide (3), and its scope has expanded beyond homosexual males to include women, IV drug users and children. (4) CMV remains the leading cause of AIDS related vision loss. In addition, there have been several reports of CMVR in immunocompetent persons. (5,6,7,8,9,10,11) This chapter will review the epidemiology, clinical characteristics, treatment approach and differential diagnosis of CMVR in the era of HAART therapy.
Viral Characteristics and Epidemiology
Cytomegalovirus is a double-stranded DNA virus belonging to the human herpes virus family. (1,, 12, 13) CMV is indistinguishable from the other herpes viruses using electron microscopy. Its histopathologic appearance, culture characteristics, and antigenic signature aid in its identification. (13) Clinical characteristics of systemic CMV infections were first described in 1905. (14) In the 1920s, CMV infections, at the time referred to as salivary gland disease, were recognized to be virally mediated. (13, 15) Later, CMV disease became known as cytomegalic inclusion disease because of the characteristic cellular inclusions seen with light microscopy in infected tissue. Although one of the major target organs for CMV is the retina,(16) presumed CMVR was not described until the 1950s. (17,18) The virus was shown to be the causative agent in 1964. (18,19)
CMV is transmitted by infected blood products and bodily secretions. It may also be transmitted across the placenta. (1) In developed countries, exposure to CMV usually occurs in childhood or early adulthood. The incidence of seropositivity increases with age. By 35 years of age nearly all persons living in North America have been exposed to CMV and over 80% have detectable circulating antibodies to the virus. (15,20)
Clinical systemic CMV infection occurs almost exclusively in persons with abnormal cell-mediated immunity and thus affects two major categories of individuals; the immunosuppressed and newborns. After initial exposure and systemic infection, CMV typically attains a dormant state. (21) During periods of immunosuppression, CMV reactivates and spreads hematogenously to infect the retina and other organs. (22) While infection by the human immunodeficiency virus (HIV) is the most common cause of immunosuppression leading to reactivation, CMV infection is also associated with congenital immunodeficiency syndromes, malignancy, systemic pharmacologic immunosuppression of patients with autoimmune disorders or organ transplant, thymectomy (23,24), splenectomy (25,26) and in hematopoeitic stem cell transplant recipients treated with alemtuzumab. (27,28) In addition, CMVR recently has been reported as sequelae of local ocular immunosuppression with intravitreal kenalog injections or intravitreal steroid implants (5,6,7,8,9) as well as in nonimmunocompromised adults. (10,11) Incidence of serologically confirmed CMV infections in newborns range between 0.5% and 2.5%. (15,20) Fortunately, only 10% of these newborns develop clinical disease.
The risk for CMVR increases as the CD4+ cell count decreases. The mean CD4+ T-cell count in adults at the time of diagnosis is typically less than 50 cells/ul. In children, CD4+ count should be adjusted for age. (29) It is rare for adults with CD4+ counts greater than 200 cells/ul to develop the disease, although it has been observed rarely in HAART responders whose pretreatment CD4+ count was less than 50 cells/ul. (2) CMVR may also develop or recur in patients in whom HAART has failed whose CD4+ lymphocyte count returns to a level below 50 cells/ul. (30) Other laboratory risk factors predictive of development of CMVR include elevated qualitative and quantitative serum CMV polymerase chain reaction (PCR), HLA-Bw4 and HLA-DRB115. HLA-Cw7 was found to be protective. (31) Certain subpopulations of patients with AIDS appear to have a lower incidence of CMVR (32,33) including young children who are less likely to have been exposed to and therefore to be harboring latent CMV. (34)
Since the widespread use of HAART, the incidence of CMVR in AIDS patients has decreased. Before the introduction of HAART, the reported estimates for the prevalence of CMVR approached 40%. (35,36,37) In the HAART era, the prevalence of CMVR has decreased to approximately 22%.(38) Nonetheless, CMV remains the leading cause of blindness in AIDS. (21,35) Persons who remain immunosuppressed are at greatest risk 39. CMV related blindness is caused by posterior (zone 1) CMVR and secondary CMV related retinal detachment (RD) in HAART naïve patients or HAART non responders. In HAART responders, catatact and cystoid macular edema (CME) are causes for relative visual loss. CMVR and CMV RDs cause approximately 40% while cataracts are responsible for approximately 25% of incident AIDS related visual loss. (40,41)
Clinical Findings
At the onset, CMVR may produce few symptoms. (21) The presence of symptoms is often related to the extent and location of retinitis. Posterior retinitis (zone 1 disease) is most often associated with blurred vision and scotoma. Peripheral disease may be heralded by the gradual onset of floaters, scintillating scotoma and decreased peripheral vision. Pain and /or redness are uncommon. Patients may be asymptomatic.
CMV causes a full-thickness retinal destruction which often initially affects retinal tissue adjacent to major retinal blood vessels. Posterior or zone 1 lesions are characterized by large areas of retinal whitening often accompanied by hemorrhage in the posterior pole. Papillitis and retinal vasculitis involving both arteries and veins is often present (Fig. 1). Immune-mediated vascular damage may play a role in the vasculitis. (22) A vasculitis resembling “frosted branch angiitis” has been reported (Fig. 2). (42) Small lesions restricted to the macula are often hemorrhage-free and may appear like large cotton wool spots (Fig. 3).
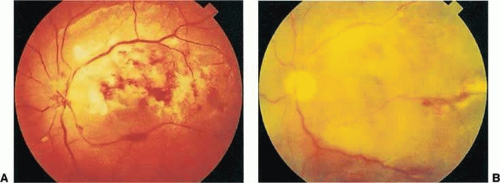 Figure 1. a. Acute posterior “zone 1” CMVR. The fulminant form is characterized by retinitis, retinal vasculitis, and hemorrhage in the posterior pole. b. Relentless progression of the CMVR resulted in no light perception 3 months later. |
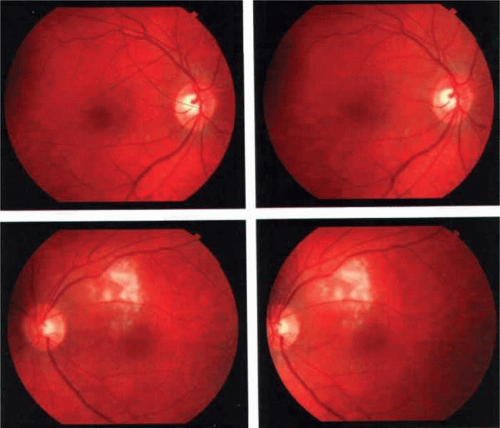 Figure 2. Large macular cotton wool spot. Unlike CMVR, there is no associated hemorrhage or retinal vasculitis. (Courtesy Drs. Adam Martidis and Mark Nelson) (From Vrabec TR. Posterior segment manifestations of HIV/AIDS. Surv Ophthalmo (March-April) 2004; 49:131-157, with permission courtesy Elsevier) |
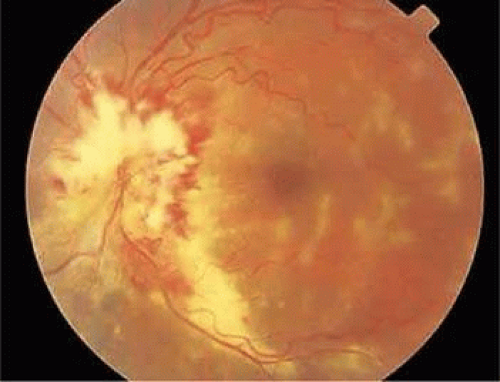 Figure 3. Frosted branch vasculitis is characterized by linear sheathing of vessels in the macular region. Papillitis, with diffuse whitening and necrosis of the optic disc, is also present in this eye with fulminant posterior CMVR. |
Peripheral lesions located anterior to the equator are often smaller, more numerous and granular in appearance with less associated hemorrhage. They are often oriented circumferentially. A subtle retinal vasculitis is often located adjacent to the lesions. Peripheral retinitis is more indolent, and focal granular infiltrates enlarge slowly in a line, leaving behind areas of atrophic retinal pigment epithelium (Fig. 4). There appears to be direct cell-to-cell transfer of infected virions in this pattern of infection. In both posterior and peripheral disease, except in acute infections, it is common to see concurrent areas of healed retinitis, characterized by chorioretinal scarring, and active necrosis which often appears as a grey-white lesion border (Fig. 5).
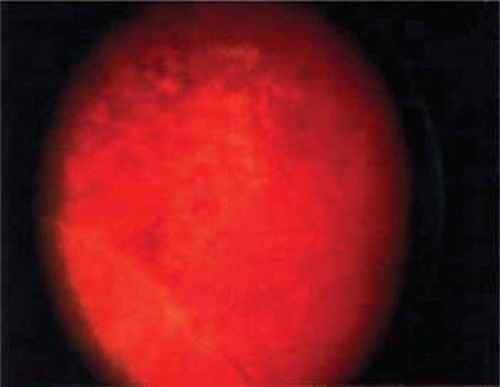 Figure 4. Peripheral indolent CMVR in the peripheral retina is circumferentially distributed. Small retinal hemorrhages and subtle retinal vascular sheathing can be appreciated. (From Vrabec TR. Posterior segment manifestations of HIV/AIDS. Surv Ophthalmo (March-April) 2004; 49:131-157, with permission courtesy Elsevier) |
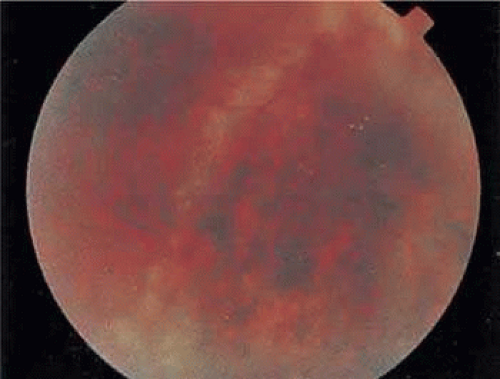 Figure 5. Progressive or recurrent CMVR. An active linear “brush fire” border of grey white retinitis is present between the normal retina to the left and the atrophic retina with associated retinal pigment epithelial scarring to the right. |
Progression of retinitis has been defined in clinical trials as movement of a lesion border at least 750 μm along a front that is 750 μm or more in length or the development of a new CMV lesion in the affected or fellow eye. (43) Retinitis progression may best be detected with serial fundus photography. (44) The rate of retinitis progression has decreased in HAART responders. (45)
Papillitis, or infection of the optic disc may be associated with posterior CMVR (See Fig. 1). CMV affects the optic nerve either directly or by extension from adjacent retinitis. (46,47) When direct involvement occurs, optic neuritis with profound visual loss usually develops. Early diagnosis and treatment may in some cases result in dramatic visual improvement or help prevent irreversible visual loss. (48,49) Untreated eyes progress to no light perception.
Evidence of more than a mild anterior uveitis is unusual with AIDS-associated CMVR. Although a few vitreous cells are typically present, a florid vitritis severe enough to result in media opacity does not develop. When a more prominent iritis or vitritis is present, other infectious agents, such as toxoplasmosis, syphilis and varicella zoster as well as masquerade syndrome caused by lymphoma should be considered. Patients with active CMVR who begin HAART may develop vitiritis or iritis as the immune system begins to reconstitute and fight the infection- see immune recovery uveitis (IRU) discussed below.
Rhegmatogenous retinal detachment (RRD) may develop in eyes with active or inactive CMVR as a consequence of multiple necrotic retinal breaks due to vitreoretinal traction and adhesions in areas of chronic retinitis or devitalized retina. (50) Prior to HAART, risk of RRD approached 50% in patients living more than 1 year after diagnosis. (51) The rate of RRD has decreased in the HAART era, particularly in persons with CD4+ > 200 cells/ul. (52) RRD is most likely to occur when retinitis is peripheral or involves more than 25% of the retina (Fig. 6). (50,53) Retinal breaks in eyes with CMVR typically occur within or at the border of necrotic atrophic retina. (54) Because breaks may be multiple, posterior and difficult to identify, RRDs are difficult to repair with standard scleral buckling procedures. Scleral buckling may be considered in cases of small peripheral detachments with inactive retinitis when the entire involved area of retinitis can be completely placed on the buckling element.
 Figure 6. CMV related retinal detachment with associated active retinitis. |
In the majority of cases, pars plana vitrectomy and retinal tamponade with silicone oil or long-acting intraocular gas is indicated (Fig. 7). (50,55,56) Oil removal may be considered in selected cases however it may be complicated by retinal redetachment in approximately 50% of cases. (57) Although anatomic success of macular reattachment with surgery is high, the visual results may be limited by the progressive retinitis in patients not responsive to HAART, postoperative cataract and silicone oil induced refractive error. (58) Demarcation laser photocoagulation may be used to delimit macula-sparing CMV-related RRDs (Fig. 8). (59) The advantage laser include better postoperative best corrected visual acuity (BCVA) by avoiding silicone oil induced refractive error and postoperative cataract.
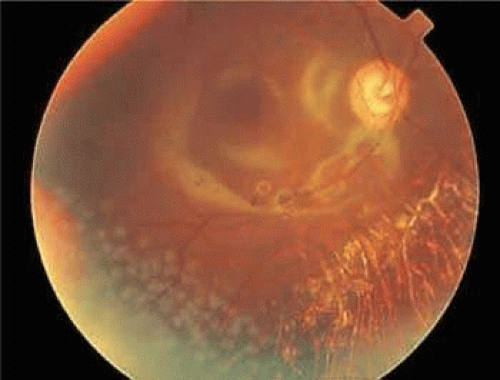 Figure 7. Attached retina following repair with vitrectomy and silicone oil injection. Reflections from the silicone oil are present in the macular region. Laser is present inferotemporally. |
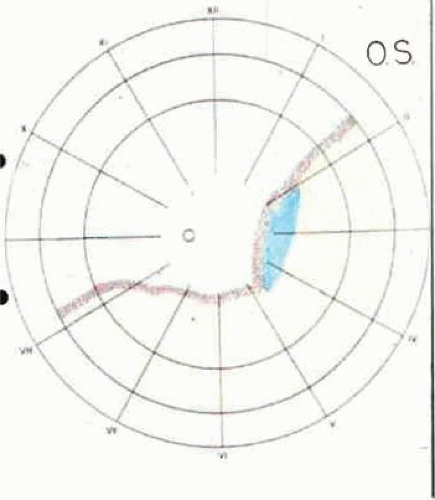 Figure 8. Schematic representation of Demarcation Laser Photocoagulation. Laser photo coagulation spots are applied in a confluent band which extends from ora serrata to ora serrata posterior to the entire region of retinal detachment and associated active or inactive retinitis. (From Vrabec TR. Posterior segment manifestations of HIV/AIDS. Surv Ophthalmo (March-April) 2004; 49:131-157, with permission courtesy Elsevier) |
Active CMVR may be asymptomatic in 15% of patients and nearly 75% of patients present with disease that is considered immediately sight-threatening by the ophthalmologist. (12) In addition, HAART-nonresponders are more likely than treatment naïve patients to have bilateral or asymptomatic disease, better visual acuity, and more peripheral retinitis. (60) Although the efficacy of screening asymptomatic patients at risk for CMVR has not been clearly defined, routine screening has been advocated at 3 month intervals in all patients with CD 4+ count less than 50 cells/ul. (61) Educating high risk patients about the symptoms of CMVR aids in early detection. (62)
COMPLICATIONS OF HAART and IMMUNE RECONSTITUTION
Immune recovery disease (IRD) is spectrum of organ specific chronic inflammatory syndromes associated with clinical immune reconstitution in AIDS patients. Patients with CMVR may develop immune recovery uveitis (IRU) during HAART. (63,64,65,66,67,68,69) IRU affects up to 63% of HAART responders (68), and is the leading cause of visual morbidity in these individuals. (40,70) IRU does not represent clinical infection. In contrast, the rejuvenated immune response to persistent intraretinal CMV antigen results in secondary findings similar to those which develop during the course of other forms of intraocular inflammation. An alternative hypothesis is that IRU may be perpetuated by an autoimmune response.
Fifty percent of incident visual loss in patients with IRU is attributable to CME (Fig. 9) and cataract (40) while vitritis (64,71), optic disc edema, and macular epiretinal membrane formation (72), vitreomacular traction syndrome (73), optic disc neovascularization (74) and proliferative vitreoretinopathy (69) may also develop. Many of the complications of IRU may be managed with anti inflammatory medications. In some cases, CME may be less responsive steroids. (75) Surgical intervention may be needed in cases of cataract and epiretinal membrane. Patients may develop more severe postoperative inflammation following cataract or other intraocular surgery. (69)
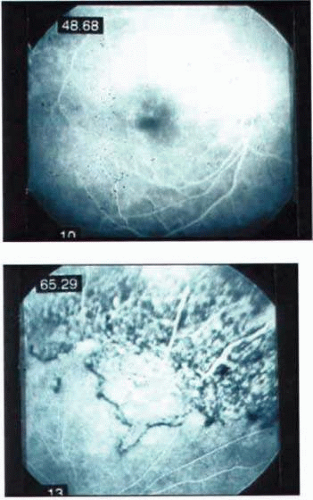 Figure 9. IRU with CME. a. Fluorescein angiogram demonstrates late staining in the macula consistent with cystoid macular edema. b. Extensive retinal scarring due to inactive CMVR is seen in peripheral views. (From Vrabec TR. Posterior segment manifestations of HIV/AIDS. Surv Ophthalmo (March-April) 2004; 49:131-157, with permission courtesy Elsevier) |
Diagnosis
In most cases ophthalmoscopic examination combined with clinical history is sufficient to confirm the diagnosis of CMVR. (12) However, in cases where the diagnosis is in question, it is important to recognize that given nearly all immunosuppressed patients who are at risk for CMVR will show serologic or culture evidence of the virus in bodily fluids. Therefore, documented CMV viremia alone, or combined with viruria does not confirm the diagnosis of CMVR.(21) Standard cultures of an aqueous or vitreous sample are also of little assistance although polymerase chain reaction (PCR) may detect CMV DNA from small amounts of intraocular fluid. (76) Aqueous and vitreous specimens can provide accurate markers to differentiate active and inactive CMVR. (77) Sensitivities for vitreous, aqueous and tear samples were reported as 67%, 37% and 12% respectively. (78) These markers were superior to extraocular measures, such as plasma PCR and blood and urine CMV cultures. PCR may be particularly useful in cases where the diagnosis is uncertain. Tissue diagnosis may be made with retinal biopsy specimens obtain during vitrectomy repair of RD. (50) Retina biopsy may show cytomegalic cells, although severe tissue necrosis may preclude this finding.
Treatment Overview
There are two principal approaches to the treatment of CMV retinitis, reversal of the underlying cause of immunosuppression and treatment with CMV specific antiviral agents.
Haart
CMVR may be controlled by reducing pharmacologic immunosuppressant therapy in patients who develop CMV retinitis outside the setting of HIV infection. (79) In AIDS patients, HAART employs a combination of medications including protease inhibitors alone or in combination with nucleoside analogues to reconstitute the immune system. (80)
Immune reconstitution is defined as an increase in absolute CD4+ count by at least 50 cells/ul to a total count of at least 100 cells /ul. (74) Until favorable HAART response has developed, patients are typically examined every 4 weeks for evidence of CMVR reactivation. In addition it is important to recognize that immune reconstitution may not include all T-cell clones, hence it is possible that CMV specific CD4+ T cell clones may be absent and deficits in pathogen-specific immune responses may persist in some individuals in spite of improved CD4+ counts and reduced HIV viral load. This may in part account for the cases of CMVR in persons with elevated CD4+ count that have been reported. (81,82,83)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


