Cystic Tumors
R. Patrick Yeatts
A true orbital cyst is any closed cavity or sac within the bony orbital confines that is lined with epithelium and contains a liquid or semisolid material.1 Many orbital cysts are developmental and present at birth, but some may not be manifest for many years; these cysts include dermoid and epidermoid cysts, cystic teratomas, encephaloceles, congenital cystic eyes, and perioptic hygromas. Other orbital cysts are acquired, arising from neighboring sinuses or adjacent adnexal structures; these cysts include mucoceles or dacryoceles. Epithelial implantations secondary to trauma or surgery also can give rise to cyst formation. Finally, vascular neoplasms, chiefly those in the lymphangioma–venous varix group, may develop cystic cavities or bleed spontaneously, forming blood-filled or “chocolate” cysts.
Often, the term cyst is used loosely in its clinical application to orbital disease. Parasitic encystment is more often an inflammatory granuloma than a cyst, although cyst is commonly used in reference to the manifestation of these infestations. Hematic cysts are not lined with epithelium but are a fibrous encapsulation of blood or blood products. Malignant epithelial neoplasms that secondarily invade the orbit may develop central necrosis and a cyst-like character.
True orbital cysts are discussed in this chapter; those arising from vascular neoplasms are discussed elsewhere in these volumes. Paracytic cysts and hematic cysts, although not epithelially lined, are discussed because of their importance in the differential diagnosis of true orbital cysts.
DERMOID AND EPIDERMOID CYSTS
Dermoid and epidermoid cysts are among the most common periorbital and orbital tumors presenting in childhood.2,3,4,5 Although their incidence is reportedly low, many of them are excluded from orbital tumor series because they commonly are found anterior to the orbital septum along the upper margin of the orbital rim. Most are first seen during the preschool years, although a dermoid cyst may be seen at any age.
Dermoid and epidermoid cysts are choristomas arising from subcutaneous epidermal rests or epidermal tissues trapped along bony suture lines or within the diploe of the bone during embryonic development. The epidermal anlage develops into a cyst lined with stratified squamous epithelium, which is usually intimately associated with or firmly attached to the frontozygomatic suture superotemporally or to the maxillofrontal suture superonasally. Rarely, these cysts involve the suture confluence of the greater with of the sphenoid, zygoma, and frontal bones or the intradiploic space of the lateral orbital rim.6 If the cyst wall contains skin appendages, such as hair follicles, sweat glands or sebaceous glands, the cyst is termed a dermoid cyst. If skin appendages are absent, the cyst is termed an epidermoid cyst.7
Typically, a dermoid cyst presents in a child as a mass protruding forward from beneath the superior orbital rim anterior to the orbital septum (Fig. 1). Dermoid cysts are found most commonly in the superotemporal quadrant and less frequently superonasally, but these cysts may occur elsewhere in the periobital region both anterior and posterior to the orbital septum and in the temporal fossa.
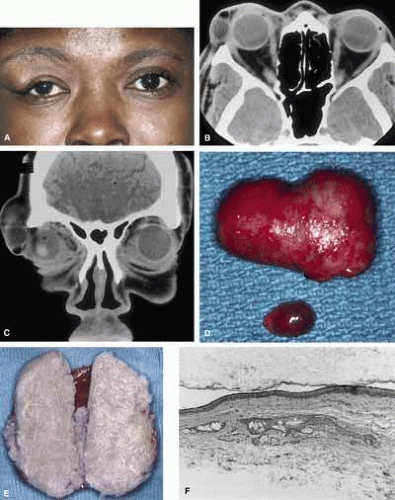 Fig. 1 A. Dermoid cyst in an adult who had a clinically apparent lesion in the superior temporal quadrant of the right eye since early childhood. Note the contour deformity of the eyelid without globe displacement of proptosis. A computed tomogram shows two cysts of different radiodensity in both axial (B) and coronal (C) sections. The two dermoid cysts show differing radiodensities. The small, dark, or radiolucent, lesion belies its high fat content; the larger, radiopaque lesion contains keratin debris. D. Morphologically, the cysts are smooth-walled and vary in content from a tan, oily liquid (small cyst) to a yellow-white, cheesy material (large cyst) as shown in cross section (E). F. Histology of a dermoid cyst shows a stratified squamous epithelium with keratin debris filling the lumen and a pilosebaceous apparatus in the cyst wall (magnification × 100). |
The usual cyst is a painless, smooth, ovoid-to-round, firm, rubbery mass. It may be mobile or immobile, being relatively free or firmly attached to the underlying bone (periosteum), but it is not attached to the overlying skin, distinguishing them from implantation cysts. Although contour abnormalities of the eyelid are common, there is little or no displacement of the globe with dermoid cysts located along the orbital rim. In an adult presentation, a dermoid cyst may frequently have a more posterior location.8 These posteriorly located cysts more typically present in adulthood, are more difficult to palpate, and proptosis and globe displacement are more common.
Rarely, an orbital cyst may pass through bony suture lines to extend intracranially or to the temporal fossa (Fig. 2).5,6 Pressure placed on the extracranial portion of a bilobed cyst may be transmitted through the bony dehiscence into the orbit, and is a cause for the mastication proptosis reported by Bullock and Bartley.9
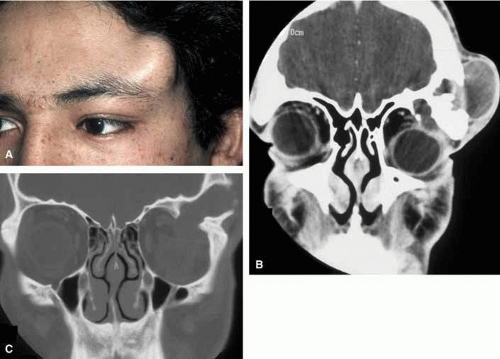 Fig. 2 A large dermoid cyst is seen in the left temple of a young man (A) that shows both an intraorbital and extraorbital component with associated bone change seen on computed tomography (B). A coronal view of the orbit with a setting to highlight bone detail shows a confluence of the intraorbital and extraorbital components through a bone defect in the superior lateral orbital wall (C). |
The nature of an orbital dermoid cyst can be demonstrated well by computed tomography (CT): the cyst has a low-density lumen and its relationship to the underlying bone is often manifested by smooth remodeling of the bone secondary to cyst expansion; the high content of fatty material within the cyst makes it radiolucent.
Because of the variable presentation of dermoid cysts, Shields et al.,5 have suggested a classification of orbital dermoid cysts by their association (or lack of association) with suture lines of the skull and assist the clinician in appropriate management. Cysts are classified as juxtasutural, sutural, or soft-tissue dermoid cysts. Those cysts adjacent to the bony suture line but not firmly attached are juxtasutural. A sutural dermoid cyst is firmly attached to bony sutures causing bone erosion, tunnels or an hourglass configuration. Soft tissue dermoid cysts may be strictly confined to soft tissues without any connection to a bone structure. Intradiploic epidermoid cysts are distinctly uncommon and were not included in Shields’ classification (Fig. 3).
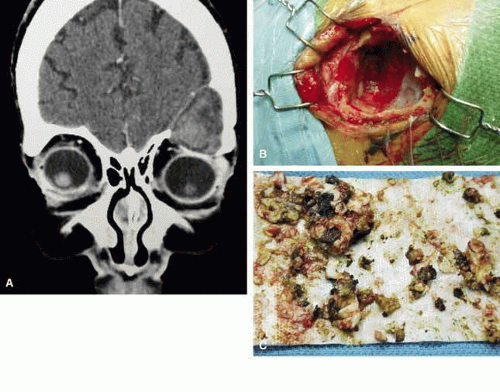 Fig. 3 In a coronal image of a computed tomogram, an intradiploic dermoid cyst is shown to involve the superior orbital rim and roof of the left orbit displacing the globe downward (A). The intraoperative cavity (B) of the cyst is observed with the evacuated keratin debris shown (C). |
It is often cosmetic considerations that prompt the parents of an affected child to seek treatment. These cysts enlarge as the child grows and the possibility of accidental traumatic rupture is ever present. In adults, mass effect or periorbital inflammation due to leakage of cyst contents may prompt medical attention and surgical removal (Fig. 4).5,10
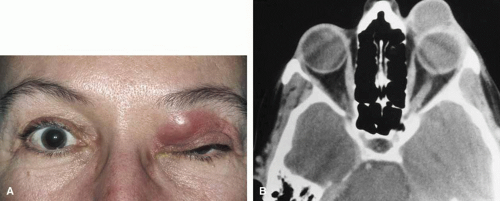 Fig. 4 A. Neglected dermoid cyst in a 47-year-old woman showing recurrent inflammation manifested by lid edema and erythema. B. Computed tomogram shows large cyst attaining a size nearly equal to that of the globe. |
Surgical removal is the treatment of choice. The surgical approach is dictated by the location of the cyst and its association with boney suture lines. In the majority of juxtasutural dermoid cysts, the lesion can be reached through an incision placed directly over it. Because many of these cysts are located along the superior orbital rim, a brow incision may be placed directly over the cyst along the superior orbital rim. Because of a potentially visible scar, however, use of an upper eyelid crease incision has been advocated.11 A posteriorly located cyst (soft-tissue dermoid) or a bilobed cyst with transmission through the orbital rim (sutural dermoid), in contrast, requires more careful planning for an approach through an anterior and/or a lateral orbital route. Large intradiploic cysts and cysts located along the orbital roof and temporal fossa may require multidisciplines and approach transcranially or a temporal skull base approach.12,13
Surgical extirpation should be complete. Intraoperative rupture of the cyst with release of its contents into the orbit may incite a mild but smoldering granulomatous inflammation. The contents of these cysts may vary from an oily, tan liquid to a cheesy, yellow-white material. When inadvertent rupture occurs, the operating surgeon must flood the wound with irrigating solution to be sure that all this material has been washed away. Complete removal of the cyst wall is curative; incomplete removal may be followed by recurrence. Although marsupialization of deep and extensive dermoid cysts has been advocated by some practitioners,14 this technique is not recommended.8
Histologic study of all these cysts is recommended, because rare cases of epidermoid cysts undergoing malignant transformation into squamous cell carcinoma have been reported in adult patients.15 Although granulomatous inflammation may be seen histologically in as many as two-thirds of dermoid cysts removed in one large retrospective series, the clinical signs of inflammation are observed in the minority of patients.5,10
TERATOMAS
Similar to dermoid cysts, teratomas are congenital tumors and choristomas.7,16,17 Although dermoid and epidermoid cysts are derived from only one germinal layer, a true teratoma has all three germinal anlagen: ectoderm, mesoderm, and endoderm.
A teratoma may become manifest at any age, but the majority are present at or shortly after birth. The tumor is rare,17,18,19 often only single cases being reported in large series of orbital tumors. Rarely is the presentation of other orbital tumors as dramatic as that of a teratoma, the eye seeming to be a mere appendage to the massive orbital component of the tumor (Fig. 5). CT imaging reveals the multicystic nature of these lesions and the often-encountered intracranial extensions.
 Fig. 5 Cystic teratoma in a newborn. (Photograph courtesy of Thomas J. Leisegang, MD, Mayo Clinic, Jacksonville, FL) |
The histology of teratomas is complex because of the presence of all three germinal layers. The presence of multiple epidermoid cysts and embryonic forms of mucin-secreting gastrointestinal mucosa within these lesions contributes to their cystic nature. Most teratomas are benign, although some seen in newborns may be malignant.
Tumor growth and unacceptable cosmetic appearance dictate the surgical removal of an orbital teratoma. Although the globe and optic nerve are not intrinsic parts of the tumor, surgical efforts to salvage vision and ocular function have been disappointing. One should preserve the globe whenever possible16,20; however, incomplete removal of the cyst leads to recurrence. Exenteration, although not recommended,18 may be necessary to effect a complete cure.
CEPHALOCELES
A congenital dehiscence in the bony cranium may enable the meningeal tissue to herniate into the orbit forming a cystic structure filled with cerebrospinal fluid: an orbital meningocele. If brain protrudes inside the meningeal sac, the term encephalocele or meningoencephalocele applies.
These cephaloceles are rare. Their diagnosis most often is made in infancy, although a cephalocele presenting deep in the orbit may not be recognized until later in life.21 Cephaloceles form during embryonic development and their formation is either the result of the failure of the neuroectoderm to separate from the surface ectoderm or to defects in osseous development when fetal fissures fail to close. In the former instance, brain tissue is pinched off by the developing bony cranium, the result being a cephalocele attached to the brain by a tissue stalk that extends through sutures between the frontal, ethmoid, lacrimal, and/or maxillary bones. In the latter instance, defects in osseous development result in true herniation of intracranial contents.22
An encephalocele most commonly presents as an anterior protrusion between the nose and eyebrow or as a lateral protrusion into the orbit (Fig. 6). Painless and elastic, the encephalocele may enlarge slowly, and pulsations may be present. The larger the defect, the greater the degree of pulsation and often, the more rapid the increase in size. A Valsalva maneuver or crying can cause a mild increase in size. Orbital signs are limited to the mass effect. Globe displacement or proptosis occurs and is related to the location and size of the cephalocele.23,24 When protruding from the nose into the lower lid, a cephalocele may resemble, and be confused with, a mucocele of the nasolacrimal sac or with a dacryocele.
 Fig. 6 Large frontal encephalocele. |
The diagnosis of an encephalocele should be considered in any child with a midline or paramedian cystic tumor. Facial anomalies such as hypertelorism, broad nasal root, or increased bitemporal diameter should alert the clinician to the possibility of an encephalocoele.
Radiographic analysis by CT or magnetic resonance imaging (MRI) is critical, both to the diagnosis and to the management of cephaloceles. Recognition of these cysts permits appropriate management rather than an accidental surgical encounter. Surgical treatment is indicated, consisting of exposure, ligation, and excision of a small encephalocele, and of transfrontal craniotomy with excision of a larger encephalocele followed by dural patching, and possibly by bone grafting if the bone defect is large.
MICROPHTHALMOS WITH CYST AND CONGENITAL CYSTIC EYE
Failure of the fetal fissure to close at 4 weeks of development results in proliferation of neuroectoderm through the opening, leading to formation of an orbital cyst. In almost all cases, the resulting eye is defective, smaller than normal, and has an attached cystic mass at birth.25,26 The cyst may be smaller or larger than the eye; its appearance is dependent on the size of the ocular defect and its rate of expansion; microphthalmos with a cyst may be bilateral.27,28,29 The cyst is slate blue and translucent, and may displace the globe (Fig. 7).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


