Skin cancer is the most common human malignancy, with an estimated 3,500,000 nonmelanoma skin cancers cases in the United States annually (1). Most tumors arise on the sun-exposed regions of the head and neck. Basal cell carcinoma is the predominant histologic type and accounts for about 90% of all cutaneous neoplasms in the head and neck region. Second in incidence is squamous cell carcinoma. Less common is melanoma, which accounts for approximately 8,700 deaths each year in the United States. There are 3,000 additional deaths related to other forms of cutaneous cancer (2). Cutaneous malignancies are classically divided into epidermal, dermal, adnexal, and melanocytic. Malignant melanoma has a distinct biologic behavior and is addressed separately in Chapter 114. Other rare skin malignancies of the dermis and adnexa are not discussed specifically, but principles of evaluation and treatment of cutaneous cancers are applicable. This chapter is dedicated to a discussion of nonmelanoma cutaneous malignancy, specifically basal cell carcinoma, squamous cell carcinoma, Merkel cell carcinoma (MCC), their precursors, and associated epidermal neoplasms.
RISK FACTORS
Risk factors for basal and squamous cell carcinomas are strikingly similar. These lesions, although seen in younger age groups, are most often encountered in patients 60 years of age or older.
The mechanism by which ultraviolet (UV) light causes sun-damaged skin has been extensively studied. Laboratory experiments indicate that the wavelengths with the most potential for carcinogenesis are those in the range of 280 to 320 nm, the UVB band. This UVB is responsible for the common sunburn. The transition from normal to actinic (i.e., sun damaged) to cancerous skin is usually a progressive process that occurs over several decades. With the current environmental changes occurring with the earth’s protective ozone layer, the concern for skin cancer becomes much more significant. A dramatic ozone depletion above the Antarctic continent has been detected (3). For each 1% reduction in atmospheric ozone concentration, there is a concomitant 2% increase in UVB penetration (4). Approximately 90% of nonmelanoma skin cancers are estimated to be associated with exposure to UV radiation from the sun (5).
The carcinogenesis of epidermal tumors parallels the multistep development of other neoplasms. As with other neoplasms, certain characteristics render the host more susceptible to the development of cancer. Traits that are associated with an increased incidence of skin cancer include fair complexion, light hair, blue or green eyes, inability to tan, propensity to sunburn, history of multiple or severe sunburns, and Celtic ancestry (6). Other factors implicated include age, occupation, habits (tanning booths), and residential geography, which are considered indirect causes of increased sun exposure.
The bulbs used in tanning booths are almost exclusively UVA wavelength and are promoted as providing a safe suntan. However, recent evidence indicates that UVA (320 to 400 nm) synergistically augments UVB responses and is independently capable of producing deleterious skin alterations and neoplasias (7).
Other etiologic factors are associated with the development of cutaneous carcinoma (6). Chronic exposure to chemical agents, such as arsenic in patients treated with Fowlers solution, has been associated with the development of multiple squamous and basal cell tumors. Patients with chronic radiodermatitis, resulting from superficial radiation therapy, demonstrate a propensity to develop multiple and aggressive lesions. Trauma in the form of burns, ulcers, and scars is also associated with the development of skin cancer (i.e., Marjolin ulcer). Immunosuppression, common in transplant patients and patients with leukemia or lymphoma, can be complicated by an increased incidence or aggressiveness of skin malignancies (8).
Studies of human papillomavirus offer additional support for the importance of immune dysfunction in the development of skin squamous cell carcinoma. One study showed human papillomavirus presence in 60% of cutaneous squamous cell carcinoma lesions found in renal autograft recipients. Moreover, human papillomavirus presence was significantly higher than that found in matched transplant recipients without cutaneous malignancy (9). Furthermore, there is evidence to suggest that human papillomavirus may be related to the development of some nonmelanoma cutaneous malignancies not necessarily associated with immune suppression.
Genetic syndromes, such as xeroderma pigmentosum (autosomal recessive) and nevoid basal cell carcinoma syndrome (autosomal dominant), are associated with a predilection for developing multiple basal cell carcinomas, often at an early age.
BASAL CELL CARCINOMA
There are several clinical types of basal cell carcinoma. Smith (10) outlined five clinical forms: nodular or noduloulcerative, morphea-like or sclerosing, superficial multicentric, pigmented, and fibroepithelioma. Although other less common types exist, subclassification is not clinically useful. The most common type is the nodular or noduloulcerative lesion. This lesion typically presents as a discrete, raised, circular lesion that appears pink and waxy with a capillary network that is easily visible. There is often an area of central ulceration and the border of the lesion is rolled. This is the type of basal cell carcinoma that is easiest to recognize and treat. A variant of this lesion is cystic basal cell carcinoma, which is also waxy and well demarcated but is more cystic in appearance.
The superficial basal cell carcinoma lesion shows evidence of scarring and atrophy, with a thread-like waxy border. This lesion may consist of one or several red scaling patches. These crusted lesions have irregular borders and gradually increase in size by peripheral extension. They are relatively uncommon in the head and neck and more frequently occur on the trunk or extremities.
The most aggressive clinical form of basal cell carcinoma is the morphea type, also called sclerosing or fibrosing basal cell carcinoma. This variety is typified by its macular, whitish, or yellowish plaque. Some physicians have noticed an increased incidence among women. The margins may be quite indistinct, and the lesion may go unnoticed for years in some patients. Complete excision is difficult because of ill-defined margins. The lesion may look like a scar, may develop telangiectasia, or may ulcerate.
A less common basal cell carcinoma variant is pigmented basal cell carcinoma, which is characterized by its brown pigmentation and may resemble a pigmented nevus or a melanoma. The appearance and behavior of this lesion seems to parallel that of nodular basal cell carcinoma. Pigmented basal cell carcinoma differs from the noduloulcerative type only by the brown pigmentation of the lesion. This type of lesion may also be mistaken for seborrheic keratosis, melanoma, or dermatofibroma.
Fibroepitheliomas, another variant, present as firm pedunculated lesions that resemble fibromas. It was first described in 1953 by Pinkus (11). These lesions commonly occur on the back.
The nevoid basal cell carcinoma syndrome is an autosomal dominant disease. During childhood, small cutaneous nodules appear, often numbering in the hundreds. These lesions initially have a rather indolent course during the nevoid phase, but as the patient ages, a neoplastic phase may occur in which the lesions show a marked change in aggressiveness. The lesions become invasive, destructive, and mutilating. Abnormalities associated with nevoid basal cell carcinoma syndrome include jaw cysts, bifid ribs, scoliosis, mental retardation, and frontal bossing.
The characteristic cell in basal cell carcinoma has a large, oval, or elongated nucleus with relatively little cytoplasm. These cells may resemble the basal cells of the epidermis, but the neoplastic forms lack intercellular bridges. The nuclei are rather uniform in size and configuration. A connective tissue stroma proliferates with the tumor and is oriented in parallel bundles around the tumor masses, causing peripheral palisading of the cells and stromal retraction. This is commonly referred to as peritumoral lacunae. The stroma is often mucinous. Because mucin shrinks with dehydration and fixation of the specimen, the stroma may show retraction from the tumor islands. This detachment of tumor islands from the stroma is known as clefting and is a helpful diagnostic sign.
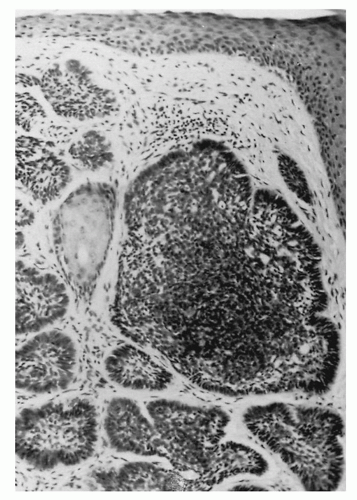
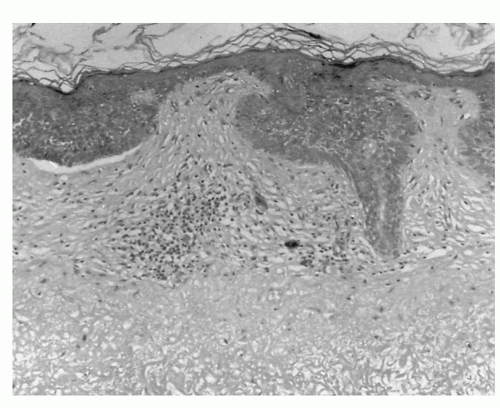
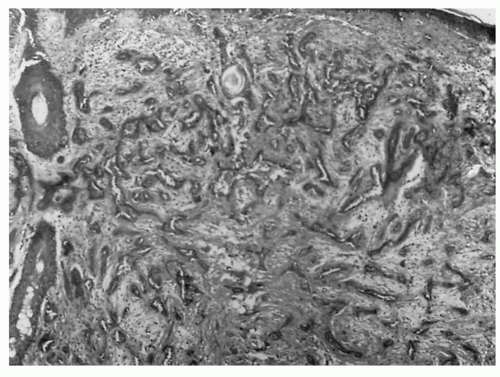
Lever (12) divided basal cell carcinoma into four basic histologic patterns: solid, keratotic, cystic, and adenoid. In the solid pattern, the cells show no differentiation. This type generally displays tumor masses of various sizes and shapes embedded in the dermis (Fig. 113.1). The peripheral cell layer may show a palisading of the nuclei. Basal cell carcinomas that differentiate toward hair structures are referred to as keratotic. This lesion is typified by undifferentiated cells in combination with parakeratotic cells and horn cysts (Fig. 113.2). Cystic tumors show differentiation toward sebaceous glands. Histologically, there may be one or several cystic spaces within the tumor lobules. In the adenoid variety of basal cell carcinoma, the tumors display a tubular or glandular formation. The strands of epithelial cells commonly form a lace-like pattern (Fig. 113.3).
Keratotic basal cell carcinoma, also known as basosquamous cell carcinoma or metatypical carcinoma, has been the subject of much controversy. The confusion arises because histologically there are coexistent features of both basal cell and squamous cell carcinomas in the same lesion, frustrating accurate assessment of prognosis and behavior. Most dermatopathologists currently believe that basosquamous tumor is a variant basal cell carcinoma, referred to by many as keratotic basal cell carcinoma (12). Although there is limited potential for metastasis, keratotic basal cell carcinoma is thought to be more biologically aggressive than many of the other types of basal cell carcinomas.
Far less common than basal cell carcinoma, squamous cell carcinoma accounts for approximately 10% of skin malignancies. As with its counterpart, basal cell carcinoma, squamous cell carcinoma is related to chronic (i.e., 10 to 20 years) sun exposure. As the equator is approached, the relative incidence of squamous cell carcinoma increases compared with basal cell carcinoma. Cutaneous squamous cell carcinoma, like basal cell carcinoma, is more common in men.
Figure 113.2 Undifferentiated cells with parakeratotic and horn cysts (keratotic type).
Squamous cell carcinoma of the skin usually presents as an erythematous, ulcerated, crusting lesion. The tumor often demonstrates a granular base that may be friable and tends to bleed with minimal trauma. There is usually an elevated area of induration at the lesion edge and there may be an inflammatory response in the adjacent tissues.
These lesions present in different patterns. Squamous cell carcinoma can present as a thickened hyperkeratotic patch or an area of crusting. Under this crust is an ulcerated base with a rolled margin. Other lesions may be recognized as areas of persistent ulceration, possibly in the site of previous trauma, burns, or an old scar (i.e., Marjolin ulcer). Neoplastic change in a chronic ulcer may result in basal cell or squamous cell carcinoma and is associated with a poorer prognosis and higher rates of metastasis. Superficial multifocal lesions can arise in actinic skin. These lesions are usually accompanied by a scaling patch that bleeds with minimal trauma. Diagnosis and determination of the extent of the lesion can be difficult, and multiple biopsies may be necessary. Squamous cell carcinoma occasionally presents as a nodular exophytic lesion. Initially cystic, it later tends to become ulcerative and progressively enlarges. These lesions may also demonstrate a sudden growth spurt.
Several histologic characteristics are important in analyzing squamous cell carcinoma. The usual histologic picture of squamous cell carcinoma of the skin is that of irregular masses of epidermal cells that proliferate downward and invade the dermis. The tumor masses may be well differentiated or may show atypical or anaplastic cells. The differentiated tumors tend to be associated with evidence of keratinization, such as keratin pearls.
Figure 113.3 Lace-like patterns of epithelial cells (adenoid type).
Some squamous cell carcinomas are actinically induced, and some arise de novo. Lesions arising in sun-exposed areas appear to follow a more benign course with a low incidence of metastasis. The de novo lesions are more aggressive in their behavior and exhibit greater potential for metastasis. It has been estimated that up to 54% of patients with de novo lesions develop regional or distant metastases (13). It is often possible to differentiate clinically between the two types of squamous cell carcinoma. Histologically, a determination can usually be made by looking for actinic changes in the skin adjacent to the squamous cell carcinoma.
Squamous cell carcinoma has metastatic potential, and regional metastatic spread is correlated with depth of invasion. Squamous cell carcinoma lesions that penetrate to Clark level IV or V are associated with a 20% regional metastatic rate.
Histologic variations of squamous cell carcinoma are numerous and include adenoid, bowenoid, verrucous, and spindle-pleomorphic types (14). The generic type is characterized by actinic changes. In the adenoid type, there is a pseudoglandular arrangement. These tubular or alveolar formations result from dyskeratosis and subsequent acantholysis. The lumina are lined with one or several layers of epithelium and are filled with desquamated acantholytic cells. The bowenoid type of squamous cell carcinoma is characterized by evidence of invasion coexistent with the findings of Bowen disease.
Verrucous carcinoma is seldom seen as a skin neoplasm on the head and neck, but it is well known as a tumor of the oral cavity and larynx. It presents as a white cauliflower-like lesion. The tumor is well differentiated, demonstrating hyperkeratosis, parakeratosis, and acanthosis. Clinical and pathologic correlations are needed to confirm the diagnosis.
In the spindle-pleomorphic type of squamous cell carcinoma, there is little evidence of differentiation. These tumors are anaplastic, show little or no keratinization, and are usually considered to be a Broders grade 4 tumor. The spindle cells are intermingled with collagen, may be arranged in whorls, and can be associated with pleomorphic giant cells.
PREMALIGNANT LESIONS
Several skin lesions are considered premalignant. This group includes a low-grade malignancy that can be treated as if it was a premalignant lesion. The most common of these are actinic keratosis, Bowen disease, and keratoacanthoma.
Actinic Keratoses
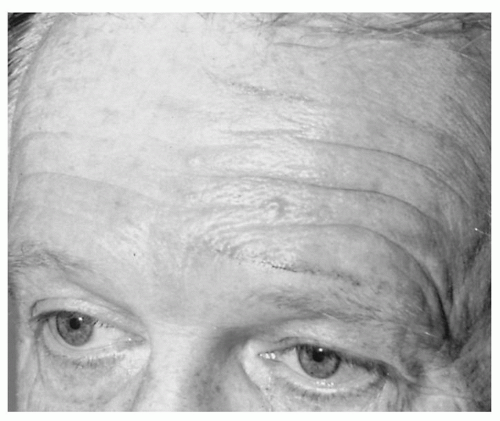
Actinic keratoses (i.e., solar keratoses or senile keratoses) is the most common premalignant lesion of the head and neck and is seen almost exclusively in sun-exposed areas of the skin. The lesions are generally less than 1 cm in diameter and are commonly located on the face, scalp, hands, and forearms (Fig. 113.4). They are considered precancerous. The chance of progression to epidermal cutaneous carcinoma has been estimated to be as great as 20% (12). They usually present as an erythematous patch, often covered by an adherent scale. Clinically, they show little or no sign of inflammation. Occasionally, there is a marked hyperkeratosis, giving the appearance of a cutaneous horn. A sandpaper-like scale is the most distinctive feature on clinical examination. Because these lesions have malignant transformation potential, most physicians believe they should be treated. Depending on the clinical setting, superficial shave excision, cryosurgery, topical treatment with 5-fluorouracil, or trichloroacetic acid peel may provide effective treatment. The differential diagnosis includes seborrheic keratosis, benign lentigo, squamous cell carcinoma, and basal cell carcinoma.
Figure 113.4 Actinic keratosis on forehead.
Bowen Disease
Bowen disease is considered a preinvasive form of squamous cell carcinoma. It can be considered synonymous with carcinoma in situ of the skin. Histologically, there is full-thickness dysplasia of the epidermis without evidence of invasion. Clinically, the lesion presents as a well-circumscribed, erythematous, scaly patch or plaque with an irregular border. As with squamous cell carcinoma, these lesions generally occur in sun-exposed areas. They are particularly common in patients with a history of chronic arsenic ingestion in whom lesions often occur on nonexposed skin. The lesion may resemble a superficial basal cell carcinoma, but it lacks the fine pearly border.
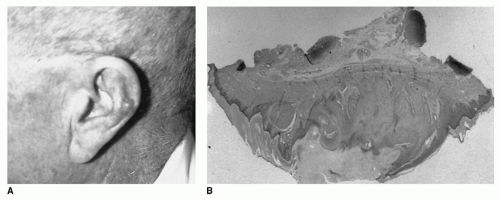
Figure 113.5 A: Keratoacanthoma of the auricle. B: Histologic volcano-appearance.
Keratoacanthoma
Keratoacanthoma is a benign usually self-limited epithelial tumor that is easily confused clinically and histopathologically with squamous cell carcinoma. It is more common in males and typically presents in older patients. There is a history of rapid growth, usually over 2 to 6 months. The lesion begins as a smooth rounded nodule, but with further enlargement, the center becomes ulcerated and filled with keratinous material, taking on a volcano-like appearance. The hallmark of keratoacanthoma is rapid growth over weeks or months.
The most common site affected is the nose. Although histologically the lesion resembles a squamous cell carcinoma (Fig. 113.5), it may involute spontaneously, leaving only a depressed scar. Because of the lack of predictability, surgical excision is recommended.
TUMOR BEHAVIOR
Staging for cutaneous basal cell carcinoma and squamous cell carcinoma has been defined by the American Joint Committee on Cancer using the TNM classification as shown in Table 113.1 (15). Tumor histology, local extent or infiltration, tumor size, anatomic site, associated risk factors (e.g., age, prior irradiation, genetic syndromes), and previous treatment must be considered in determining the risk of recurrence for a given lesion. High-risk features include depth and extent of invasion, anatomic location, and histologic differentiation (Table 113.2).
The clinical and histologic types are significant prognostic variables. The morphea type of basal cell carcinoma is well known for its subversive attitude. This lesion generally spreads centrifugally by way of finger-like projections of tumor. It is deceptive in its behavior and can be difficult to evaluate and control. Keratotic (i.e., basosquamous), recurrent basal cell, and spindle cell variants of squamous cell carcinomas are also associated with worse prognoses. Poorly differentiated or undifferentiated tumors are considered high-risk features for staging purposes.
TABLE 113.1 AJCC CLASSIFICATION FOR CUTANEOUS SQUAMOUS CELL CARCINOMA AND OTHER CUTANEOUS CARCINOMAS (EXCLUDING THE EYELID)
Primary tumor (T)
TX: Primary tumor cannot be assessed.
T0: No evidence of primary tumor
Tis: Carcinoma in situ
T1: Tumor 2 cm or less in greatest dimension with less than two risk features
T2: Tumor >2 cm or tumor of any size with two or more high-risk features
T3: Tumor with invasion of the maxilla, mandible, orbit, or temporal bone
T4: Tumor with invasion of the skeleton (axial or appendicular) or perineural invasion of the skull base
Regional lymph nodes (N)
NX: Regional lymph nodes cannot be assessed.
N0: No regional lymph node metastasis
N1: Metastasis in a single ipsilateral lymph node, 3 cm or less
N2a: Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm
N2b: Metastasis in multiple ipsilateral lymph nodes with none more than 6 cm
N2c: Metastasis in bilateral or contralateral lymph nodes with none more than 6 cm
N3: Metastasis in a lymph node more than 6 cm
Distant metastasis (M)
M0: No distant metastasis
M1: Distant metastasis
Only gold members can continue reading. Log In or Register to continue