The field of critical care medicine is complex and rapidly changing. The goal of this chapter is to familiarize the otolaryngologist with some of the basic principles of critical care medicine and provide evidence for common postoperative complications often seen in the intensive care unit (ICU). This chapter increases a general understanding of critical care medicine while facilitating a good working relationship with the intensivist.
TISSUE OXYGENATION AND ORGAN PERFUSION
Many physicians struggle with understanding the difference between tissue oxygenation and organ perfusion. Although these topics are often regarded as synonymous, they are not. This misunderstanding is likely the reason for inappropriate fluid resuscitation and blood transfusions, and emphasizes the importance of understanding their differences and treatment.
OXYGEN DELIVERY
In general terms, oxygen delivery (DO2) refers to the amount of oxygen that is delivered to the tissue. It does not refer to the amount of oxygen uptake at the cellular level. The lack of oxygen delivered into the tissues can be due to several defects including: respiratory failure, inadequate delivery to the tissues, and defective uptake into the tissue. DO2 to the peripheral tissues can be calculated by using the following formula.
DO2 = CO×1.34×Hb×SaO2+(PaO2×0.003)
where CO, cardiac output; Hb, hemoglobin; SaO2, oxygen saturation; and 1.34 is a conversion factor that relates how much oxygen can bind to hemoglobin. (PaO2 × 0.003) describes the amount of oxygen that is dissolved in blood and not bound to hemoglobin.
Notice the amount of oxygen delivered to the peripheral tissues as dissolved oxygen that is not attached to hemoglobin is miniscule (PaO2 × 0.003). Therefore, when the oxygen saturation of hemoglobin is high, it does not help to provide excess supplemental oxygen. The CO, Hb, and SaO2 all have equal contributions to the amount of oxygen delivered to the peripheral tissue. Therefore, CO and Hb are as important as the oxygen content in the blood.
OXYGEN EXTRACTION
Oxygen extraction (VO2) refers to the amount of oxygen that is extracted from the blood into the peripheral tissues at the capillary level and utilized by the cell. Since oxygen is not stored in the cell, extraction (consumption) is equal to the amount of oxygen utilized by the cell. The rate of oxygen extraction is expressed by the following formula:
O2 = CO × 1.34 × Hb × (SaO2 − SvO2)
where CO, cardiac output; Hb, hemoglobin; SaO2, arterial oxygen saturation; SvO2, venous oxygen saturation; and 1.34 is a conversion factor that relates how much oxygen can bind to Hb.
The most important concept to understand in tissue oxygenation is that delivery (DO2) and extraction (VO2) are not the same. The rate of oxygen extraction from the blood into the peripheral tissues (VO2) is done at a constant rate. In normal circumstances (a normal DO2), only 25% of the oxygen in the blood is extracted into the tissues. Therefore, 75% of the oxygen in the blood is not extracted into the tissue and is considered “extra.” The amount of oxygen extracted into the tissue is better described as the oxygen extraction ratio (O2ER).
O2ER = VO2/DO2
The O2ER reveals that as the delivery of oxygen to the tissue (DO2) decreases, the amount of oxygen extracted into the cell is the same (no change in VO2). However, the O2ER will increase (more oxygen disassociation from Hb) to provide the constant transfer of oxygen into the cell.
At some point, the delivery of oxygen (DO2) will be low enough not to provide the constant flow of oxygen into the cell, which is needed for aerobic metabolism. This is the point that must be identified by the physician. This level is often referred to as the critical DO2. This is the level that cellular metabolism changes from aerobic to anaerobic metabolism. Therefore, increasing the delivery of oxygen without a level below the critical DO2 is often unnecessary and may carry the risk associated with the treatment (i.e., inappropriate blood transfusions).
Since the DO2 is irrelevant until it reaches the critical DO2 signifying a drop in tissue oxygenation (VO2), the decrease in VO2 is the important factor. The measurement of the oxygen consumption (VO2) requires invasive devices, like a Swan-Ganz catheter or Metabolic cart, that are not readily available in all situations. However, the O2ER is closely linked to the oxygen consumption (VO2) and can be easily measured since most critically ill patients have a central venous catheter. We know from many human and animal studies that the oxygen consumption (VO2) starts to drop with an O2ER of approximately 50%. The O2ER can be calculated by subtracting the amount of oxygen in the venous blood from the oxygen in the arterial blood. Since the peripheral tissues do not store oxygen, this difference of oxygen content between the arterial and venous blood is the amount of oxygen extracted at the cellular level. This can be expressed as:
O2ER = SaO2 − SvO2
where SaO2, arterial oxygen saturation; SvO2, venous oxygen saturation.
The SaO
2 is easily measured with noninvasive devices such as a pulse oximeter. The SvO
2 is most accurate when obtained in the pulmonary artery that is distal to where the coronary sinus empties desaturated venous blood into the right atrium from the myocardium. A Swan-Ganz catheter is needed to obtain this “mixed venous” (SvO
2) measurement in the pulmonary artery. However, the venous oxygen saturation taken from the superior vena cava (ScvO
2) from the tip of a “central line” is in close proximity to the pulmonary artery oxygen saturation (SvO
2). The average variation between these measurements is about 5% (
1). So the oxygen saturation from a central venous catheter (ScVO
2) can fairly accurately replace the mixed venous saturation (SVO
2), especially when following trends. This allows the physician to fairly accurately predict the oxygen consumption without a Swan-Ganz catheter.
ANAEROBIC METABOLISM
As stated previously, the switch from aerobic to anaerobic metabolism occurs at the point where the supply of oxygen (DO2) cannot meet the metabolic demands (VO2) at the cellular level. This occurs at an O2ER below approximately 50%. Another indirect marker of anaerobic metabolism is lactate. The serum lactate level can be an effective marker of cellular oxygenation but using this to solely determine end-organ perfusion can be problematic. Since lactate is cleared by the liver, its clearance is variable and therefore is not the best immediate marker to guide therapy.
BLOOD TRANSFUSIONS IN THE ICU
Blood transfusions are often a lifesaving therapy in surgical ICUs. However, blood transfusions are also one of the most misused resources available to physicians. We will describe the indications, side effects, and evidence surrounding the use and misuse of blood transfusions in the ICU.
The effect that packed red blood cells (PRBCs) have on tissue oxygenation is often misunderstood. As described earlier, the delivery of oxygen to the tissues is dependent upon cardiac output, amount of hemoglobin, and the oxygen saturation. In normal individuals, only 25% of delivered oxygen (DO2) to the peripheral tissue is utilized (VO2). Therefore, an excess of oxygen is delivered to the tissue. As the DO2 decreases (i.e., decrease in hemoglobin), the amount of oxygen extracted from hemoglobin increases, but the oxygen uptake into the tissues (VO2) remains unchanged. So, giving a blood transfusion when the extraction ratio is above 50% will not increase the amount of oxygen utilized by the cell. In fact, giving a blood transfusion in the setting of isovolemic anemia will often decrease the VO2 due to the increased viscosity of PRBCs causing a decrease in perfusion of the microcirculation.
Blood transfusions are analogous to a “Blood Transplantation” and the side effects of blood transfusions are similar to most other transplanted organs from another human (allograft). The previous concerns for the infectious risk of hepatitis and human immunodeficiency virus are now very uncommon (
2). The most notable side effects consist of immunosuppression and rejection. The immunomodulating effects of receiving a blood transfusion increase the risk of the recipient to developing nosocomial infections, acute respiratory distress syndrome (ARDS), and possible development of autoimmune diseases later in life (
3,
4). However, the most important immunomodulating effect of blood transfusions in postoperative oncologic patients is the significant increase in cancer recurrence and death (
5,
6,
7). Most of the evidence regarding cancer recurrence is in colorectal cancer but some studies have specifically examined the recurrence rate after squamous cell carcinoma (SCC) of the head and neck (
8,
9). Jones et al. (
6) examined the recurrence/metastasis rate in Stage 3 SCC in the head and neck in regards to blood transfusions. They found the recurrence/metastasis rate of SCC to be significantly higher in the group that received a blood transfusion (64% vs. 22%). This reason alone should prompt careful consideration prior to giving a blood transfusion in postoperative patients.
More recently it has been shown that not all units of PRBCs are equal (
9) and that the length of storage makes a significant difference in the quality of PRBCs that are transfused. Longer storage times are associated with ATP depletion, decreased 2,3 DPG, protein oxidation, and loss of membrane flexibility. The combination of the membrane flexibility and decreased 2,3 DPG would conceptually reduce the quality of the PRBC transfusion the most. The loss of membrane flexibility limits the ability of the red blood cell (RBC) to pass through the microvascular circulation, and the decrease in 2,3 DPG will cause a left shift in the oxygen-hemoglobin disassociation curve causing less off-loading of oxygen to the peripheral tissues. The loss of membrane flexibility and increased viscosity of PRBCs are often cited as being the culprits for decreasing the DO
2 following the administration of PRBC. This is best displayed in a study examining the progressive normovolemic hemodilution in canine skin flaps (
10). The authors progressively infused a colloid solution while removing blood from the canine to drop the hemoglobin while maintaining adequate intravascular volume and cardiac output, which effectively decreased the viscosity of the blood (normovolemic hemodilution). As the hemoglobin dropped, the authors measured the tissue oxygenation on the skin flaps. They found that as the hemoglobin decreased, the tissue oxygenation actually improved instead of the decline. The tissue oxygenation of the normal skin continued to improve until the canine reached a hemoglobin of 4.
In 1942, Adam and Lundy (
11) suggested a hemoglobin level of less than 10 should prompt a blood transfusion. Since that time, study after study has attempted to find the optimal hemoglobin level that would necessitate a blood transfusion in the nonhypovolemic patient. Thus far, the Transfusion Requirement in Critical Care (TRICC) trial is the only prospective randomized controlled trial with an adequate sample size to examine this issue. The TRICC trial (
12) examined the difference between a hemoglobin transfusion trigger of 7 versus 10 in euvolemic patients in the ICU. The authors concluded “A restrictive strategy of red-cell transfusion is at least as effective as and possibly superior to a liberal transfusion strategy in critically ill patients, with the possible exception of patients with acute myocardial infarction and unstable angina.” This was later confirmed in another prospective randomized controlled trial (
13). In 2006, Marik et al. (
14) performed a systematic review of the literature and concluded “the need for a PRBC transfusion should be individualized based on a patient’s clinical circumstances rather than an arbitrary hemoglobin concentration.”
SHOCK
The term shock is used very commonly throughout the medical field but is often poorly understood. In simple terms, shock is synonymous with tissue dysoxia. The treatment of shock is guided by correcting the variables in the DO2 equation that are abnormal (CO < 6 L/min, Hb < 7, and oxygen saturation < 90%). There are two situations in which shock is not caused by decreased DO2; mitochondrial dysfunction (sepsis, cyanide, etc.), and vasodilatory states (systemic inflammatory response syndrome, sepsis, spinal shock, etc.). There is no treatment for the mitochondrial dysfunction seen in sepsis other than supportive care. Vasopressors are likely the optimal treatment for vasodilatory states (i.e., systemic inflammatory response syndrome) in the setting of normovolemia.
VASOACTIVE AGENTS IN THE ICU
The use of vasoactive infusions in the ICU is not uncommon and their use can be lifesaving. However, severe complications can be associated with the use of vasopressors. There is not good evidence to support which vasopressor to use in a given situation or if they improve outcomes in shock. However, we will review commonly used vasopressors in the ICU and the ideal situations in which they should be applied (see
Tables 5.1 &
5.2).
There are several things in which a physician should consider prior to initiating vasopressor infusion. These considerations should include: cardiac output, volume status, peripheral vascular resistance, and causes of hypotension. All four of these considerations are very important and must be known prior to initiating any vasopressor for hemodynamic support.
Common Pitfalls to Avoid with Vasopressors
Systolic Left Ventricular Failure
In patients with severe systolic dysfunction, a rapid increase in peripheral vascular resistance will cause increased myocardial work and worsening cardiac output with rapid decline. These patients may benefit from inotropic support or decreased peripheral vascular resistance rather than a vasoconstrictor.
Diastolic Dysfunction
Diastolic dysfunction is often misunderstood. A simplistic view of diastolic dysfunction is to imagine a muscular bodybuilder that cannot straighten his arms due to the tight bicep muscle. This bicep muscle is very strong but it cannot completely relax. This is analogous to a hypertrophied left ventricle in diastolic dysfunction. The left ventricle is unable to stretch and accept enough preload to generate sufficient cardiac output despite being able to contract normally. It is a preload problem; therefore, the ejection fraction is normal despite a low cardiac output. Although ventricular hypertrophy is the most common type of diastolic dysfunction, any disease process that limits the ability of the ventricle to relax is considered diastolic dysfunction. Patients with severe diastolic
dysfunction can be very difficult to manage perioperatively. If the patient is underresuscitated and placed on a vasoconstrictor in the setting of severe diastolic dysfunction, the cardiac output will quickly decrease as the vasopressor infusion is quickly titrated upward to maintain hemodynamic stability. This type of patient must get adequate volume resuscitation prior to starting a vasopressor for hemodynamic support.
Cardiac Valve Disease
Cardiac valvular disease can be difficult to treat or diagnose without imaging studies (i.e., echocardiogram). Vasopressor therapy can dramatically worsen valvular abnormalities such as but not limited to aortic/mitral stenosis and insufficiency. The immediate clue that a cardiac valve abnormality may be significantly contributing to the hemodynamic instability is a murmur on cardiac auscultation. The presence of a murmur in the setting of hemodynamic instability should prompt an immediate echocardiogram.
Tachycardia
Vasopressors with high beta-adrenergic activity can be highly arrhythmogenic. These medications can create a variety of arrhythmias including: ventricular ectopy, ventricular tachycardia, and sinus tachycardia. Tachycardias that reach rates above 130 often create a decrease in ventricular filling time (decreased preload) that exacerbates the tachycardia. Epinephrine, dobutamine, and dopamine are the usual culprits. Tachyarrhythmias may be indication to decrease the dose or switch to another agent.
Rapidly Increasing Vasopressor Requirements
Any time a vasopressor is initiated and the patient starts to rapidly decompensate or the vasopressor requirement steadily increases, the diagnosis and intravascular volume should be reevaluated immediately. This should always make the physician question the cause of hypotension. Inappropriate use of vasopressors can cause rapid hemodynamic decomposition and can be fatal.
Types of vasopressors:
Epinephrine: Epinephrine is a naturally occurring catecholamine that has potent β1 and α1 properties. The combination and potency of these properties often limit its use in the ICU.
Norepinephrine: Norepinephrine is the most widely used vasopressor in surgical ICUs. It possesses the same α1 properties as epinephrine but has limited β1 properties. The reduced β1 properties limit the associated tachycardia and ectopy that is seen with other β1 agonists. Norepinephrine is considered the first choice vasopressor in most situations requiring hemodynamic support.
Vasopressin: Vasopressin is identical to antidiuretic hormone, which is secreted by the posterior pituitary. Vasopressin affects V1 and V2 receptors as an agonist. The V1 receptor is found on peripheral blood vessels that causes vasoconstriction. There is some evidence to suggest vasopressin is beneficial as a second vasopressor when the hypotension is refractory to norepinephrine. It should not be used at a dose greater than 0.04 µg/kg due to mesenteric ischemia.
Dobutamine: Dobutamine is a pure other β agonist. Therefore, it has potent inotropic (increased contractility) and chronotropic (increased heart rate) activity. It is often the drug of choice when inotropic activity is needed. However, its potent β1 activity can create tachycardia and ventricular ectopy at higher doses. The β2 properties often cause hypotension, which can be counteracted with avoidance of hypovolemia or addition of an α1 agonist.
Dopamine: Dopamine is still one of the most widely used vasopressors despite the common side effects of tachycardia and ectopy. Due to these side effects, most intensivists use it as an alternative to norepinephrine. Dopamine may be beneficial in early sepsis but is contraindicated in septic shock. The cardiovascular effects and target receptors are dependent upon the dose administered (
Tables 5.1 and
5.2). It is important to remember these ranges are approximate and vary in each patient.
Phenylephrine: Phenylephrine is a pure α1 agonist. It is often used following spinal cord injuries that cause vasodilation. Phenylephrine often causes a reflex bradycardia secondary to the acute vasoconstriction and should be used with caution in patients with bradycardia.
MECHANICAL VENTILATION
The first form of mechanical ventilation was introduced as the “iron lung” in the 1920s. Modern ventilators introduced in the mid-1980s have changed critical care medicine as a specialty. Ventilators are very complex machines with a simple function, to breathe for the patient. Although the concept is simple, the complexity of the interaction between the patient and ventilator can take an entire career to completely understand. Ventilator dysynchrony (“Bucking the Vent”) is common and the correct treatment almost never involves sedation. A skilled or experienced intensivist can often immediately determine the etiology of the dysynchrony. The correct treatment for dysynchrony is simple—fix the cause. This involves knowing the intricacies of the ventilator and understanding the different modes available.
Modes of Mechanical Ventilation
Volume Control
Volume control (VC) is a mode of mechanical ventilation commonly used in the medical ICUs. The respiratory rate and tidal volume are set by the physician. When the patient initiates a breath, the ventilator will give the prescribed volume. If the patient does not initiate a breath, the ventilator will give the same prescribed volume. Therefore, the minute ventilation in VC is determined by the respiratory rate multiplied by the prescribed tidal volume (which is not true for synchronized intermittent mechanical ventilation [SIMV]).
Pitfalls with VC
Breath-stacking can be a dangerous complication of VC. This occurs when the patient or ventilator initiates a breath before complete exhalation of the previous tidal volume. By stacking several breaths on top of one another, the mean airway pressures may reach levels high enough to cause barotrauma, pneumothorax, or pulseless electrical activity (PEA). Anytime a patient suddenly develops high airway pressures, PEA, or desaturation; the physician should first disconnect the ventilator from the endotracheal tube to equalize mean airway pressures. This same concept (“airtrapping”) often applies to patients with obstructive lung disease who often have prolonged expiratory times.
Synchronized Intermittent Mechanical Ventilation
SIMV is the most frequently used ventilator mode in the surgical ICU. The surgical ICU, unlike the medical ICU, rarely initiates mechanical ventilation for primary respiratory failure (e.g., pneumonia or chronic obstructive pulmonary disease exacerbation). SIMV is very similar to VC except that a patient initiated breath will not be given the prescribed tidal volume. The physician sets a respiratory rate and a prescribed tidal volume that will only be given if the ventilator initiates the breath. SIMV differs from the older IMV models by “synchronizing” a patient initiated breath that is very close to a ventilator initiated breath. For instance, if the patient initiates a breath very close to a predetermined ventilator breath, the ventilator will fully support this patient initiated breath with the prescribed tidal volume and not give the predetermined ventilator breath. The advantage to SIMV is that it is difficult to create breath-stacking or airway-trapping. However, if the patient
initiated breaths do not generate sufficient tidal volumes to maintain minute ventilation, the patient will quickly become tachypneic and fatigued. This can be avoided by adding pressure support ventilation (PSV) to each patient initiated breath to increase the tidal volumes.
Pressure Control Ventilation
Pressure control ventilation (PCV) is very similar to VC and SIMV except the ventilator will stop the inspiratory flow at a prescribed pressure rather than a prescribed volume. This mode of mechanical ventilation was developed to prevent high airway pressures when the patient has poor lung compliance.
Pitfalls of PCV
The inspiratory volumes are different with every breath in PCV so the minute ventilation also varies. Also the lung compliance can improve, which will increase the tidal volumes that can create volutrauma. The patient should be closely supervised when using PCV.
Pressure Support Ventilation
Pressure support ventilation (PSV) is a commonly used mode of mechanical ventilation used in all ICUs. It can be used as the primary mode or used in addition to another mode of mechanical ventilation. In a nutshell, PSV supports a patient initiated breath. In PSV, the ventilator delivers a flow-rate sufficient to reach the prescribed airway pressure and the ventilator will terminate the inspiration when the flow rate decreases by 25% which signifies that the patient has stopped inhaling. All breaths that are spontaneously initiated by the patient will be supported to the amount of pressure prescribed by the physician. PSV is an excellent method of weaning mechanical ventilation. The advantages of PSV are that the patient can determine their minute ventilation, which minimizes ventilator dysynchrony when compared to VC, SIMV, or PC.
Pitfalls of PSV
Since there are no mandatory ventilator breaths with PSV, hypoventilation can be problematic in patients on sedatives due to decreased respiratory drive.
Pressure Regulated Volume Control
Pressure regulated volume control (PRVC) is a complex mode of mechanical ventilation that is most often used in patients with poor lung compliance (acute lung injury or ARDS). It can be used with VC or SIMV. PRVC is a volume cycled mode (inspiratory flow stops at prescribed volume), which will constantly adjust the inspiratory flow rate during the inspiration of each delivered breath. The adjustment of the inspiratory flow rate allows more inspiratory volume at lower airway pressures. Similar to other volume cycled modes of mechanical ventilation (e.g., VC or SIMV), PRVC will stop the inspiratory flow if the peak airway pressure reaches a predetermined value.
Airway Pressure Release Ventilation
Airway pressure release ventilation (APRV) is often referred to as a newer mode of mechanical ventilation. It was actually first introduced in the late 1980s. Although many physicians struggle with understanding APRV, it is merely continuous positive airway pressure (CPAP) with occasional releases. It offers the advantage of allowing the patient to spontaneously breathe without additional inspiratory flow from the ventilator. Allowing spontaneous breathing offers many benefits. It decreases ventilator dysynchrony while improving oxygenation and cardiac output. There are many studies that reveal the improvement of oxygenation and cardiac output when compared to standard mechanical ventilation. However, despite these improvements there has been no proven survival benefit when using APRV. Also, the improved patient-toventilator interaction often requires less sedation.
High-Frequency Oscillation
High frequency oscillation (HFO) is used primarily as a rescue mode of mechanical ventilation in refractory hypoxemia seen in ARDS. This unconventional mode of mechanical ventilation improves oxygenation by maintaining an increased mean airway pressure (similar to APRV), which enables recruitment of collapsed alveoli. The constant mean airway pressure maintains alveolar recruitment, which reduces shunting and prevents high peak pressures. Like APRV, HFO significantly improves oxygenation without changing mortality.
Pitfalls of HFO
Only experienced providers should use HFO due to its complexity. The patient often has to be completely sedated secondary to the extreme discomfort experienced with this unconventional mode of ventilation. Hypercarbia (high CO2) can be problematic due to the small tidal volumes seen in HFO.
Proportional Assist Ventilation
This newer mode of mechanical ventilation was developed to limit ventilator dysynchrony. In general terms, proportional assist ventilation (PAV) is a newer generation of PSV. PAV differs from PSV by adjusting the inspiratory flow-rate during each breath to attain the percentage of effort that is prescribed by the physician. The physician prescribes the amount of “work” that is done by the ventilator compared to the patient. The ventilator will calculate the “work” or energy in joules required for each inspiration. The ventilator will provide enough flow to match the prescribed “work.” This mode should allow for rapid weaning and reduced ventilator dysynchrony. However, the available literature has not revealed an advantage over PSV.
Discontinuing Mechanical Ventilation
It is clear that prolonged intubation or mechanical ventilation is linked to increased mortality, morbidity, length
of stay, and costs; thus, it is important to extubate the patient when appropriate. Most authors would suggest that a 10% reintubation rate is appropriate. This number may be inflated for surgical patients since the ventilator is usually not for pulmonary dysfunction that is often seen in the medical ICU. It is also clear that reintubation in the ICU carries a significant increase in morbidity and mortality. These factors are why the decision for extubation is both important and difficult.
Factors to consider when contemplating extubation represent both pulmonary and nonpulmonary origins. The first consideration for extubation is to be sure the primary reason for intubation has been resolved. Other nonpulmonary contributors would include: neurologic status, ability to clear secretions, hemodynamic stability, nutrition, and acid-base status. The acid-base status is a very important consideration. The respiratory system is the first compensatory mechanism to correct metabolic acidosis/alkalosis. For instance, in metabolic acidosis the patient will become tachypneic in order to increase the pH. This tachypnea increases dead-space ventilation while also increasing energy expenditure in a patient that may have a predilection for respiratory fatigue. The opposite is true for metabolic alkalosis in which the primary compensation is hypoventilation.
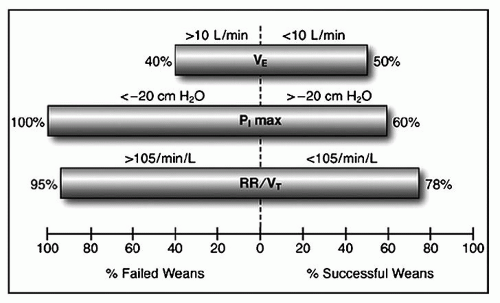
There are many methods of weaning from mechanical ventilation. In 1995, Esteban et al. (
15) compared four methods of weaning from mechanical ventilation. They revealed that patients managed with spontaneous breathing trials at least once daily were the best protocol for weaning. Ely et al. (
16) later demonstrated that combining the daily wean screen with spontaneous breathing trials further decreased time of mechanical ventilation. Common measures used to determine the likelihood of successful extubation are displayed in
Figure 5.1.
Common Protocols
(17) for Discontinuation of Mechanical Ventilation
Spontaneous daily awakening (
18)
Spontaneous breathing trials (
19)
Timing of Tracheostomy
The optimal timing of tracheostomy in a patient receiving prolonged mechanical ventilation is controversial. A recent examination of the National Trauma Databank revealed large variations in the timing of tracheostomy during prolonged mechanical ventilation (
20). In 1984, Whited (
21) noticed subglottic damage from the endotracheal tube/cuff was evident at 7 days. A short time later, the National Association of Medical Directors of Respiratory Care recommended tracheostomy to be performed in patients that required mechanical ventilation greater than 3 weeks (
22). Since that time, many observational studies have suggested early tracheostomy is beneficial. However, these studies have mixed results. One concern with the available literature is that many studies use different terminology to describe early versus late tracheostomy.
The perceived advantage of early tracheostomy would include: decreased sinusitis, decreased tracheal stenosis, decreased mechanical ventilation, decreased ventilator associated pneumonia (VAP), better secretion clearance, and decreased mortality. However, not all of these are supported by the literature and there is no evidence that early tracheostomy improves long-term mortality. A recent randomized controlled trial examined tracheotomy at 6 to 8 versus 13 to 15 days in 600 ICU patients (
23). There were more VAPs in the 13- to 15-day group but this did not reach statistical significance (
p = 0.07). This study also found the early group required less time on the ventilator and decreased ICU stay. There was no change in mortality at 28 days. Interestingly, 39% of patients that received a tracheostomy had a complication associated with its placement. The authors concluded, “considering that anticipation for tracheotomy of
1 week increased the number of patients who received a tracheotomy, and more than one-third of the patients experienced an adverse event related to the tracheotomy, these data suggest that a tracheotomy should not be performed earlier than after 13 to 15 days of endotracheal intubation.”