and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
Silicone tendon expanderSuperior oblique palsyThree-step testThird nerve palsySixth nerve palsyInferior oblique palsy8.1 Superior Oblique Palsy
8.1.1 Clinical Features
The clinical features of superior oblique paresis vary widely depending on the type. Common features include an ipsilateral hypertropia that increases on contralateral gaze, and a positive head tilt test with the hypertropia increasing on head tilt to the side of the hypertropia. Congenital superior oblique paresis is commonly associated with ipsilateral inferior oblique overaction and relatively less superior oblique underaction. Acquired superior oblique paresis, on the other hand, has relatively normal versions and minimal inferior oblique overaction, but significant extorsional diplopia. The head tilt test can help to differentiate primary inferior oblique overaction from inferior oblique overaction secondary to superior oblique paresis. A positive head tilt test indicates a superior oblique paresis, and a negative head tilt test suggests primary inferior oblique overaction.
8.1.2 Parks Three-Step Test
The Parks three-step test is used in patients with a hypertropia, to help diagnose whether a vertical muscle is paretic and to identify the paretic muscle. The head tilt test is a crucial part of the test. If the head tilt reveals a change of more than 5 PD on tilt from one side to the opposite side, it is considered a positive test and indicates the strong possibility of a vertical muscle palsy. The paretic muscle is identified by completing the Parks three-step test (see Table 8.1). For example, a patient presents with a left hypertropia that increases in right gaze and increases on left head tilt, as in Fig. 8.1. The highlighted muscles in Table 8.1 show the process of elimination (left to right) to identify the paretic muscle: left superior oblique (LSO). A positive head tilt test is not pathognomonic of a vertical muscle palsy. Both dissociated vertical deviation and a small hypertropia associated with intermittent exotropia can have positive head tilt tests. The head tilt test is applicable only to a single paretic vertical muscle, as multiple paretic muscles or the presence of restrictive strabismus make the test unreliable.
8.1.3 Head Tilt Test Made Easy
Because of the complexity of the three-step test, it is difficult to do it in your mind without a paper and pencil and at least one textbook on strabismus. A trick that simplifies the three-step test is to consider the head tilt first. If the hypertropia increases on head tilt to the side of the hypertropia, then an oblique muscle is paretic. A hypertropia that increases on head tilt to the opposite side of the hypertropia is caused by a paretic vertical rectus muscle. This quickly narrows the field of possibilities. For example, a left hypertropia that increases on head tilt to the left (same side as the hypertropia) indicates a paretic oblique muscle, either LSO or RIO. If the left hypertropia increases in right gaze, it is a paretic LSO. If the left hypertropia increases in left gaze, it is a RIO palsy.
Table 8.1
Parks three-step test
First step: hyper in primary position | Second step: hyper increases in gaze | Third step: hyper increases with head tilt | ||
|---|---|---|---|---|
RSO | ||||
RIR | RIR | |||
RHT | R | R = LIO | ||
LSR | LIO | L = RIR | ||
LIO | ||||
RSO | ||||
L | R = RSO | |||
L = LSR | ||||
RSR | ||||
RIO | RSR | |||
LHT | R | R = RSR | ||
LSO | LSO | L = LSO | ||
LIR | ||||
RIO | ||||
L | R = LIR | |||
LIR | L = RIO | |||
8.1.4 Unilateral Versus Bilateral Superior Oblique Paresis
Signs of unilateral and bilateral superior oblique paresis are listed in Table 8.2. A unilateral superior oblique palsy typically has a significant hypertropia in the primary position that increases to the opposite gaze and with tilt to the side of the hypertropia. Signs of a bilateral superior oblique palsy include small or no hypertropia in the primary position, reversing hypertropias in side gaze, and head tilt. There is a right hypertropia on tilt right, a left hypertropia on tilt left, a right hypertropia in left gaze, and a left hypertropia in right gaze. The presence of a V-pattern and bilateral extorsion on fundus exam further suggest bilateral involvement.
Table 8.2
Unilateral versus bilateral superior oblique paresis
Clinical sign | Unilateral | Bilateral |
|---|---|---|
Superior oblique underaction | Ipsilateral underaction | Bilateral underaction |
Inferior oblique overaction | Ipsilateral overaction | Bilateral overaction |
V-pattern | <10 PD | >10 PD |
Hypertropia | >5 PD | <5 PD (except asymmetric paresis) |
Head tilt test | Increasing hyper on ipsilateral head tilt | Positive head tilt test to both sides (RHT tilt right and LHT tilt left) |
Objective torsion on fundus exam | Ipsilateral | Bilateral |
Extorsion on double Maddox rod test | <10° (congenital; usually do not have subjective extorsion) | >10° (congenital; usually do not have subjective extorsion) |
An asymmetric bilateral superior oblique paresis can look like a unilateral superior oblique paresis and is termed “masked” bilateral superior oblique paresis. A masked bilateral paresis should be suspected if there is even trace inferior oblique overaction of the opposite eye. Also, if there is a large hypertropia in the primary position that precipitously diminishes on gaze to the same side of the hypertropia, consider a masked bilateral superior oblique paresis. For example, the patient in Fig. 8.1 has a left superior oblique palsy with a LHT 20 PD in the primary position that diminishes to LHT 2 PD in left gaze, and trace right inferior oblique overaction.
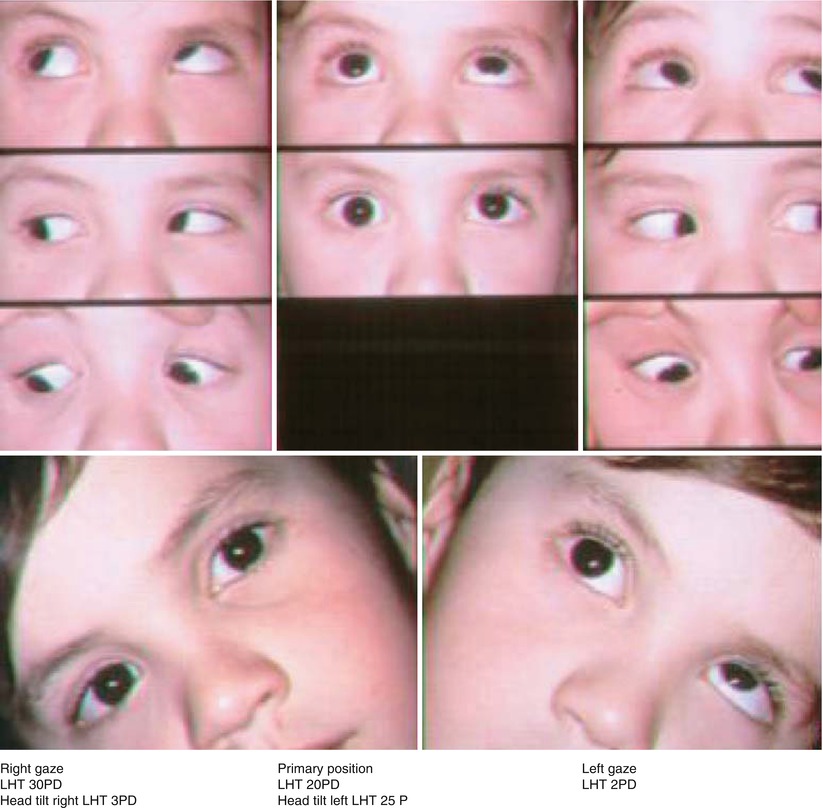
Fig. 8.1
Masked bilateral superior oblique palsy
This indicates that the right superior oblique is also paretic, with right inferior oblique overaction reducing the left hypertropia in left gaze. Surgery for a unilateral superior oblique palsy can unmask a masked bilateral superior oblique paresis with postoperative overaction of the contralateral inferior oblique muscle.
8.1.5 Congenital Superior Oblique Palsy
The cause of congenital superior oblique palsy is unknown. In some cases, the superior oblique paresis is associated with a lax tendon and, rarely, an absent superior oblique tendon. The Indiana group [1] suggests performing an exaggerated forced duction test of the superior oblique tendon at the beginning of surgery to see if the tendon is lax or absent.
8.1.5.1 Clinical Features
Patients with congenital superior oblique paresis adopt a compensatory head tilt opposite the side of the palsy to minimize the deviation and establish binocular fusion. Facial asymmetry is commonly present and may be the result of chronic head tilt. There is usually a large hypertropia in the primary position and a significant inferior oblique overaction, usually with relatively less superior oblique underaction. Although the paresis is present at birth, the first clinical signs of congenital superior oblique paresis often present in late childhood or even adulthood. Patients with congenital superior oblique paresis develop large vertical fusional amplitudes and fuse large hypertropias up to 35 PD. The presence of large vertical fusion amplitudes is an important clinical sign that the hyperdeviation is long-standing, rather than acquired, and is suggestive of a congenital superior oblique palsy. Fusional control weakens over time, resulting in a deviation that becomes manifest in later life. Review of family photographs will often document a long-standing head tilt opposite to the side of the hypertropia, indicating a congenital rather than an acquired superior oblique palsy.
Patients with congenital superior oblique paresis typically have good stereopsis and manifest the hyperdeviation intermittently when they are fatigued. Even though patients with congenital superior oblique paresis typically have high-grade stereopsis, most have the ability to suppress, avoiding diplopia. Some patients will complain of diplopia, but usually not torsional, although they have objective extorsion on indirect ophthalmoscopy.
8.1.5.2 Indications for Surgery
Surgery is indicated for a significant head tilt, a hypertropia causing asthenopia, and symptomatic diplopia. The timing of surgery is controversial. Some suggest early surgery, even in infancy, to prevent secondary facial asymmetry, but others advocate waiting until 2–3 years of age. Advocates for late surgery reason that strabismus measurements are more reliable and binocular function is more mature and stable after infancy. There is no good evidence to clearly choose. Our advice is to wait until 2 years of age as long as the head tilt is mild and binocular fusion is maintained. If head tilt is severe or binocular fusion is compromised, early surgery is indicated.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


