(1)
Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
Cotton-wool spots in malignant arterial hypertension have been known since Liebreich [1] described them in 1859. Cotton-wool spots are common, acute, nonspecific retinal lesions. Many articles in the literature have reported that they are seen in retinopathies due to a whole host of conditions. There is a voluminous literature on the subject, mostly based on anecdotal case reports. Conditions include hypertensive retinopathy, diabetic retinopathy, retinal vein occlusion, transient retinal artery occlusion, carotid artery disease, cardiac valvular disease, Purtscher’s retinopathy, interferon-associated retinopathy, giant cell arteritis, systemic lupus erythematosus, polyarteritis nodosa, Wegener’s granulomatosis, dermatomyositis, Henoch-Schonlein purpura, IgA nephropathy, human immunodeficiency virus retinopathy, cytomegalovirus retinitis, Bartonella henselae neuroretinitis, ocular Lyme borreliosis, dengue fever, malaria retinopathy, leptospirosis, radiation retinopathy, bone marrow transplantation retinopathy, metastatic carcinoma, leukemic retinopathy, Hodgkin’s disease, X-linked lymphoproliferative disorder, sarcoidosis, Takayasu’s arteritis, retinopathy of pancreatitis, pernicious anemia, polycythemia vera, methotrexate-induced blood dyscrasia, nonfamilial amyloidosis, intravenous drug abuse, and, occasionally, following a marked fall of blood pressure [2]. Brown et al. [3] described the incidence of various diseases associated with cotton-wool spots in 24 patients.
Pathogenesis and Pathophysiology of Cotton-Wool Spots
To understand the true nature and pathogenesis of cotton-wool spots, one has to have a full understanding of the retinal capillary bed; this is discussed in detail in Chap. 8. The retinal capillaries are arranged in two layers [4] (Fig. 17.1): (1) a superficial layer in the ganglion cell and nerve fiber layers and (2) a deeper layer in the inner nuclear layer, which is denser and more complex than the former. Among the superficial layer of retinal capillaries in the posterior part of the fundus, there is a special type of retinal capillaries called radial peripapillary capillaries [5] (Fig. 17.2). Their characteristic features are discussed in Chap. 8. Radial peripapillary capillaries, because of their distinctive features, play an important role in the development of several lesions. For example, cotton-wool spots are often located in their distribution, which indicates that they may play a role in their pathogenesis, as discussed below.
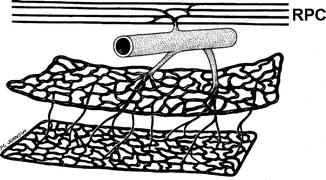
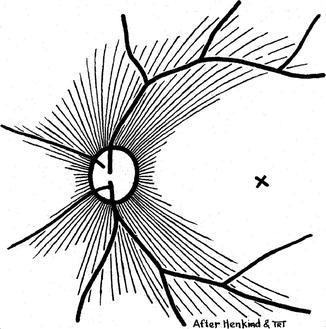
Fig. 17.1
Schematic representation of two layers of the retinal capillaries and radial peripapillary capillaries (RPC) (Reproduced from Henkind [4])
Fig. 17.2
Schematic representation of radial peripapillary retinal capillaries. X = Site of foveola (Reproduced from Henkind [5])
There has been conflict on the pathogenesis and pathophysiology of the cotton-wool spots for a long time, and a voluminous literature has accumulated on the subject. Müller [6] in 1858 reported that ischemia of only a few minutes’ duration resulted in simple swelling of the axons and this occurred focally, giving rise to nodular or varicose enlargement. Since 1929 many authors have concluded that cotton-wool spots are minute infarcts, related to occlusion or spasm in the retinal arterioles [7–9]. Ashton [10] in 1970 provided an excellent comprehensive review of the subject and dealt with the various views reported in the literature at that time; that review is still mostly valid. Following is a brief summary of that and also of some additional information which has emerged since then.
Cotton-wool spots are localized areas of swelling in the inner layers of the retina, predominantly involving the nerve fiber layer. There have been experimental and clinical studies to investigate their pathogenesis and pathophysiology. In experiments, these lesions were produced by injecting artificial emboli, e.g., latex microspheres in dogs [11], glass spheres in pigs [12, 13], and polystyrenedivinylbenzene beads in owl monkeys [14]. All these studies showed that ischemia was the cause. It has also been shown that ischemia may be due either to arteriolar or to capillary obstruction [11]. Clinically, cotton-wool spots are seen in association with diseases producing emboli, from the heart and carotid arteries, but also in other conditions (see above). Cotton-wool spots have been described in malignant arterial hypertension in man and animals [9, 15–17] and ascribed to fibrinoid necrosis in the vessel wall, which causes occlusion. Fibrinoid necrosis also would seem a likely cause of cotton-wool spots in systemic lupus erythematosus, dermatomyositis, and polyarteritis nodosa. Leishman [9] reported that a cotton-wool spot in malignant arterial hypertension is caused by occlusion of a small arteriole.
Ashton [18] showed that in hypertensive retinopathy, on India ink injection, the capillaries within cotton-wool spots did not fill, but the vessels were found to be present in retinal digest preparations. In hypertensive retinopathy, these microscopic observations have been confirmed in the living eye by fundus fluorescein angiography, which shows no filling of the capillaries in the region of the cotton-wool spot. The arterioles in the region of the cotton-wool spot have been shown to have structural changes, and in hypertensive retinopathy, this has been fibrinoid necrosis. Thus, with all the evidence available at that time, Ashton [15] favored the view that the cotton-wool spot resulted from focal circulatory insufficiency in the territory supplied by the occluded arteriole.
In an experimental study, where cotton-wool spots were produced in pigs by occluding the retinal arterioles (by injecting glass microspheres into the carotid artery), the following findings were reported by Dollery et al. [13]. The spots resembled the human cotton-wool spots as regards their color and texture and poor capillary perfusion. Fluorescein fundus angiography showed that the capillary bed in the occluded arteriole did not fill, and there was no leak of fluorescein in the retina, and there was no vascular abnormality around the border of the cotton-wool spot. In addition, India ink preparations in the vascular bed underlying cotton-wool spots showed poor filling of the superficial radial peripapillary capillaries in the area of the lesion, even though deeper retinal capillaries were better filled; the reason for the location of cotton-wool spots in the radial peripapillary capillary region may be the relative sparsity of inter-capillary links in the radial peripapillary capillaries. This study showed that cotton-wool spots developed exclusively at sites of arteriolar occlusion and that the areas most likely to develop cotton-wool spots were those near the optic disc, which had poor collateral flow in the early stages following embolization. By 4–6 weeks the retina returned to a normal appearance in the areas of cotton-wool spots – which is a well-known phenomenon in all retinal ischemic infarcts. Dollery et al. [13] reported the development of collateral filling of vessels in a number of animals in the territory of the blocked arteriole, and the amount varied with the size and position of the lesion. The efficiency of collateral blood flow continued to increase for up to 6 weeks after embolization, and the collateral vessels did not leak fluorescein.
In Dollery et al.’s [13] experimental study, ultrastructural changes in the cotton-wool spots were investigated [19]. Within 1 h after embolization, there was focal swelling with opacification of the inner retina in the center of the embolized area, and this was found to be predominantly caused by a massive fusiform swelling of nerve fibers. The swelling was located in the axoplasm. Therefore, white opacification of the retina, which is the cardinal feature of the cotton-wool spot, is predominantly due to swelling or intracellular edema of the retinal nervous elements, notably the nerve fibers, and not to exudation or extracellular edema. After about 72 h, the swollen segments of the nerve fibers became filled with mitochondria, membrane-bound microvesicles, dense bodies, membranous whorls, and neurofilaments, which are signs of orthograde axoplasmic flow obstruction. These changes are characteristic of the axonal reaction at this stage and are most evident at the periphery of the cotton-wool spot, where the swollen axons and their ganglion cells have not been affected by ischemia. There were active macrophages removing the degenerated nerve endings in the 3-day and older specimens. The late changes (4–25 days after embolization) were predominantly reactive to the injured tissue, and condensed masses of proliferating organelles and neurofilaments can sometimes be seen ingested within macrophages and reactive astrocytes. Finally the ischemic area is represented solely by a glial scar containing a few persistent nerve fibers, hyaloid bodies, vessels, and macrophage-ingested materials. Based on this experimental study, the authors [19] concluded that the pseudonucleus of the cytoid body probably consisted of an aggregation of the proliferating and degenerating axonal structures, which were lying either within the swollen terminal bulb of the axon or engulfed within a macrophage or astrocyte.
Ashton [10], based on a review of the literature, concluded that “There would therefore appear to be considerable argument in favour of focal ischaemia as the primary cause of cotton-wool spots” and, in different diseases with cotton-wool spots, arteriolar obstruction “may be a common factor, the differing reactions depending upon its degree, extent and rate of development.”
Cytoid Bodies
These were first described by von Heymann [20] in 1855 in a case of malignant arterial hypertensive retinopathy, and he regarded them as degenerate ganglion cells. Müller [6], in 1858, showed that they were swollen varicose nerve fibers. Friedenwald [8] in 1949 felt they were due to retinal precapillary arteriole occlusion, with resulting ischemia of the nerve fiber layer. Ashton [10], in his review, discussed the controversy on the nature of cytoid bodies in detail. A cytoid body is a swelling of a nerve fiber and consists of large numbers of mitochondria with numerous vesicles and granules of varying size. Wolter [21] showed that the bulbous swellings are associated with interrupted nerve fibers and that the swellings are in the part of the axon still attached to the ganglion cell. Based on microdissection and electron microscopic studies of post-mortem hypertensive retinopathy [15], experimental hypertension in monkeys [16], and experimental study of cotton-wool spots produced by injection of glass microspheres into the carotid artery [13, 19], Ashton [10] concluded that the axon’s “distal stump attached to the ganglion cell forms a bulb-like swelling, which may develop into a cytoid body.” Its pseudonucleus was thought to be due to aggregated elements within the swollen exoplasm [15].
McLeod et al. [22] in 1977 experimentally occluded small retinal arterioles in 4 pigs aged between 6 and 12 weeks old by argon laser photocoagulation. They did axoplasmic flow studies in these eyes by autoradiography by intravitreal injection of tritiated leucine. The leucine concentrated in the swollen axon terminals on the peripheral aspect of 2-day-old infarcts, due to interruption of orthograde axoplasmic transport; but it was absent from the terminals on the disc side of infarcts. They also demonstrated obstruction to both orthograde and retrograde axoplasmic flow in these eyes. They “concluded that cotton-wool spots should be redefined as accumulations of cytoplasmic debris in the retinal nerve-fibre layer caused by obstruction of orthograde or retrograde axoplasmic transport in ganglion cell axons.” It is well established that axonal ischemia interrupts axoplasmic flow. Therefore, the obstruction of orthograde or retrograde axoplasmic transport in this study was due to focal ischemia in the axons. The same findings were demonstrated previously by ultrastructural studies in experimentally produced cotton-wool spots in pigs [19] (see above). Later in 2005, McLeod [23] argued that cotton-wool spots are not retinal nerve fiber infarcts. This view is contradicted by the following evidences:
1.
On resolution of cotton-wool spots, retinal nerve fiber loss develops corresponding to the distribution of the cotton-wool spots [17, 24], as is well demonstrated in Fig. 17.3, where Fig. 17.3a shows the distribution of the cotton-wool spots during the acute phase in malignant arterial hypertensive retinopathy, and Fig. 17.3b of the same eye later on when the infarct opacity has resolved and regional nerve fiber loss has developed. This was also reported by other investigators clinically [25– 28]. A fundus photograph by Kozak et al. [29] also shows this. These findings are proof of the fact that there is infarction of the nerve fibers in the region of the cotton-wool spots. In view of these findings, any claim that there is no retinal nerve fiber infarct in cotton-wool spot cannot be accepted. However, one has to be aware of the following two caveats: (1) If the size of the infarct is minute, this nerve fiber loss may not be detectable by ophthalmoscopy, giving a false impression. (2) Also, permanent loss of the axons depends upon the severity of ischemic insult, so that mild ischemic damage, while it may produce cotton-wool spots, may not be severe enough to produce apparent nerve fiber loss. My experimental study showed that complete loss of nerve fibers occurs with severe acute retinal ischemia lasting for 4 h or more [17].
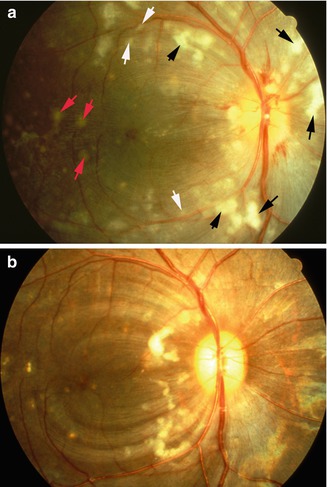
Fig. 17.3
Fundus photographs of the right eye of a monkey with experimental malignant arterial hypertension. (a) Shows multiple cotton-wool spots (black arrow), focal intraretinal arteriolar transudates (white arrow) and acute focal retinal pigment epithelial lesions (red arrow), and macular edema (Reproduced from Hayreh et al. [24]). (b) It shows resolution of old cotton-wool spots and appearance of new ones, with development of multiple areas of nerve fiber bundle loss in the location of resolved cotton-wool spots (seen as dark semicircular bands in the macular region) (Reproduced from Hayreh et al. [17])
I have conducted detailed studies of cotton-wool spots in 60 eyes with hypertensive retinopathy [17] and in more than a thousand eyes with various types of retinal vein occlusion. The various aspects of cotton-wool spots in malignant arterial hypertension are discussed at length elsewhere [17]. Based on that study I described the ophthalmoscopic, fluorescein angiographic, and other features of cotton-wool spots and concluded as follows: “There is overwhelming evidence in the literature and also in my study that cotton wool spots are due to occlusion of the terminal retinal arterioles, with focal nonperfusion of the retinal capillaries in their distribution, resulting in acute focal inner retinal ischemia, development of cotton wool spots and infarction of the nerve fibers in their location.”
The presence of cotton-wool spots in giant cell arteritis requires special mention, since giant cell arteritis is an ophthalmic emergency. There are several reports of finding of cotton-wool spots in giant cell arteritis. In my study [32] of ocular involvement by giant cell arteritis, of the 123 eyes with visual loss, one third had cotton-wool spots during the early stages of the disease (Fig. 17.4). It is well established that giant cell arteritis has a special predilection to involve the posterior ciliary artery and cause thrombosis in it. My studies [33] suggest that the posterior ciliary artery and central retinal artery often arise by a common stem from the ophthalmic artery (Fig. 17.5). The primary lesion caused by giant cell arteritis is thrombosis in the artery. A partly thrombosed artery can throw microemboli, and if those microemboli enter the retinal terminal arterioles, they result in the development of cotton-wool spots [32]. It is well known that giant cell arteritis is a disease of the medium-sized and large arteries; therefore, giant cell arteritis cannot itself involve the terminal retinal arteriole and cause development of cotton-wool spots.
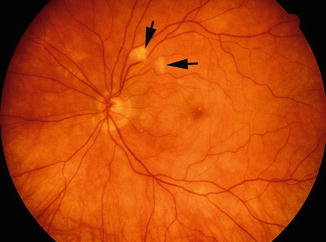
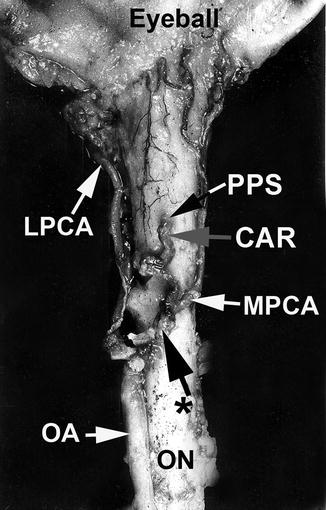
Fig. 17.4
Fundus photograph of the left eye of a patient with giant cell arteritis. It shows two cotton-wool spots (arrows)
Fig. 17.5
The central artery of the retina and medial posterior ciliary artery arising by a common trunk from the ophthalmic artery, as seen from below (Reproduced from Hayreh [33]) CAR central artery of the retina, LPCA lateral posterior ciliary artery, MPCA medical posterior ciliary artery, OA ophthalmic artery, ON optic nerve, PPS point of penetration into the sheath by CAR, * common trunk of origin of CAR and MPCA
Conclusion
All the available evidence shows that cotton-wool spots are due to occlusion of retinal terminal arterioles, which results in acute ischemic lesion in the involved inner retina, particularly the retinal nerve fibers. Cotton-wool spots are mostly located in the region of the retinal radial peripapillary capillaries, which have distinctive features different from other retinal capillaries; those may play an important role in the development of cotton-wool spots (see Chap. 8). The reason for the location of cotton-wool spots in the radial peripapillary capillary region may be the relative scarcity of inter-capillary links in the radial peripapillary capillaries. Cotton-wool spots are often due to embolism, but other factors can equally be responsible, e.g., in hypertensive retinopathy, vasculitis, and other conditions mentioned above.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


