Cosmetic Blepharoplasty
Marcus M. Marcet
Tamara R. Fountain
Brian S. Biesman
Background
Presently, blepharoplasty ranks among the top five cosmetic surgical procedures. In the year 2006 alone, 233,000 blepharoplasty surgeries were performed.1 Humans, however, have had a documented interest in improving the appearance of the periorbital region for over 4,000 years.
The Ebers papyrus from ancient Egypt described the custom of using eye makeup consisting of a black paste (known as kohl in Arabic) on the brow and lid margins to make the eyes appear larger and brighter.2 One of the earliest descriptions of upper eyelid blepharoplasty was from the Arabian physician Ali ibn Isa of Baghdad (AD 940-1010).3 Ali ibn Isa’s surgical technique involved the use of controlled tissue necrosis (Fig. 1) to remove the excess eyelid skin.4 Modern plastic surgery emerged in the early 19th century with refinements and advancements in surgical techniques, including blepharoplasty. However, the modern technique of blepharoplasty was not described until 1951 by Salvador Casta[not tilde]ares.3 Moreover, in 1952 Sidney Fox (1898 to 1983) first termed the condition of excess eyelid skin associated with aging as dermatochalasis.5
 Figure 1. Ali ibn Isa’s surgical technique used controlled tissue necrosis to remove the excess eyelid skin. (Reifler DM: The American Society of Ophthalmic Plastic and Reconstructive Surgery [ASOPRS]. The first twenty-five years: 1969–1994; history of ophthalmic plastic surgery: 2500 BC-AD 1994. San Francisco: Norman Publishing, 1994, with permission.) |
The modern approach to blepharoplasty includes varying amounts of excision and/or repositioning of eyelid skin, orbicularis oculi muscle (Fig. 2), and orbital fat. The desired outcome of cosmetic blepharoplasty has evolved to currently emphasize a surgical outcome giving a natural, refreshed look (Fig. 3). Although the surgery itself is not especially technical, an excellent understanding of the anatomy and preoperative planning individualized to the patient are of paramount importance.
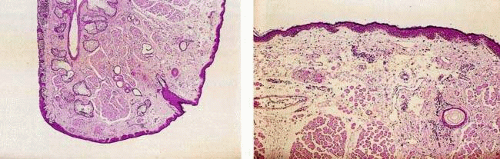 Figure 2. Normal eyelid skin. (Figure 2-1 from Sassani JW: Ophthalmic Pathology with Clinical Correlations. New York: Lippincott Raven, 1997:13, with permission). |
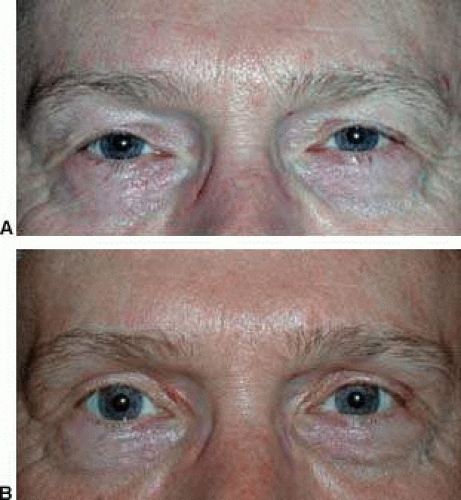 Figure 3. A. Patient with dermatochalasis prior to surgery. B. Postoperative appearance following bilateral upper eyelid blepharoplasty. |
Evaluation
The preoperative evaluation begins with listening to the patient. Establishing rapport with the patient is helpful in putting the patient at ease. Ascertaining the patient’s aesthetic desires, concerns, and expectations is essential to guiding preoperative planning. A handheld mirror can facilitate the preoperative discussion. Reviewing old photographs of the patient serves to establish the patient’s original anatomy and appearance. An optional second preoperative visit can further strengthen the relationship with the patient and can give the patient additional time to study the details of their condition at home.6 An ideal patient candidate for cosmetic blepharoplasty will have a clear understanding of the surgery and reasonable expectations about the outcome.
At the initial preoperative consultation, the patient’s general health is assessed including asking about thyroid disease (Fig. 4) and diabetes. Obtain a list of the patient’s medications, with special attention to blood thinning medications, such as nonsteroidal anti-inflammatory drugs (NSAIDS), aspirin, and coumadin. Given the increased tendency for hemorrhage in patients taking platelet inhibiting medications, if medically not contraindicated, these medications should be discontinued prior to surgery.
 Figure 4. Eyelid retraction secondary to thyroid eye disease. |
Assess the patient’s past ocular history by asking the patient about any dry eye conditions, contact lens use, other ophthalmic disorders, or periocular skin disease. Also note any previous eye surgeries such as LASIK and glaucoma filtering procedures. Ask the patient about any past oculofacial plastic surgery (e.g., face lift, blepharoplasty), and any past trauma. Inquire about keloid or scar formation.
Patient Preparation for Surgery
Preoperatively the patient should stop all blood thinning products. If sedation will be used, then the patient must not eat or drink anything by mouth after midnight on the day before surgery. The patient needs to make arrangements to bring a driver to take them home after the procedure. The patient should also plan to have a friend or relative care for them postoperatively on the day of surgery. The patient must be aware that postoperatively they will have bruising (Fig. 5), swelling, and skin stitches. In addition, after surgery the patient must minimize physical exertion and follow postoperative instructions carefully.
 Figure 5. A. This 60-year-old man has significant brow ptosis, which gives the appearance of dermatochalasis. B. Normal postoperative bruising is seen one week after endoscopic brow lift surgery (blepharoplasty was not performed). |
Anatomic Considerations of Cosmetic Blepharoplasty
An advanced knowledge of the anatomy of the eyelids and periocular structures is essential to achieving successful outcomes in oculofacial cosmetic surgery. Although each patient represents an individual anatomic variation, there are average measurements that can serve as a guideline. With the eyes in primary position, the normal palpebral fissure measures 9 to 11 mm. The vertical height of the cornea is usually 10 mm. The distance from the upper eyelid margin to the light reflex on the cornea (MRD1) typically measures 3.5 to 5 mm.7 In the lower eyelid, the eyelid margin typically rests at the inferior limbus and thus the distance from the margin to the corneal light reflex (MRD2) is about 5 mm. The horizontal intercanthal distance is usually 28 to 30 mm. The lateral canthal angle is approximately 2 mm higher than the medial canthal angle.8 The average height of the upper eyelid crease and eyebrows can vary depending on the sex of the patient. Women tend to have a lid crease measuring between 10 to 12 mm, whereas men often have a lid crease measuring 7 to 8 mm. Although there is a wide range of normal, women also tend to have eyebrows which rest higher on the orbital rim and often have a gentle arch which peaks in the lateral third and slopes downward nasally. Men, in contrast, have flatter brows that sit lower on the orbital rim.9 Last, the height of the eyelid crease can vary by the ethnicity of the patient. The well described anatomic differences in the site of fusion between the levator aponeurosis and the orbital septum, for example, in Caucasian eyelids compared to Asian eyelids result in frequently noticeable differences in the presence and/or height of the upper lid crease.10



