Corneal Perforations
Joel Sugar
Kristina Thomas
Corneal perforations occur in various circumstances. Regardless of the source, treatment is essential to maintain or restore the integrity of the globe, prevent the formation of synechiae, prevent the ingress of microorganisms or epithelium, and limit tissue destruction and scarring. In this chapter the discussion is focused on the causes, diagnosis, and treatment of corneal perforations.
ETIOLOGY
Trauma from sharp objects often leads to lacerating perforations that are amenable to standard surgical repair. At times, however, tissue defects that cannot be coapted remain. Also, even after surgical wounds, leaks may persist or fistulous tracts develop. The use of mitomycin-C for pterygium excision and refractive procedures can be an additional risk for postoperative perforation. Likewise, trauma from chemicals or radiation leading to ulceration may lead to perforation.
Infection is probably the most frequently encountered source of corneal perforation. Direct invasion of microorganisms, proteolytic enzymes elaborated by organisms, corneal cells and inflammatory cells, persistent loss of epithelium, and decreased corneal sensitivity may all enhance the likelihood of ulceration and perforation in the presence of corneal infection. Bacterial, viral (Fig. 32-1), fungal, and protozoal infections can all result in loss of corneal substance and perforation. A suggestion has been made that the type of treatment of ulcers may affect perforation with an increased perforation rate reported following fluoroquinolone treatment of bacterial keratitis.1
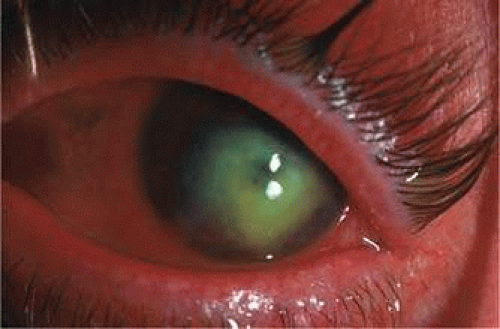 Figure 32-1. Perforated cornea from herpes simplex viral keratitis. |
Exposure of the cornea owing to abnormal lid function as can be seen after eyelid injury or ectropion from herpes zoster, or with limited lid closure and poor Bell phenomenon as seen in some myopathies and neuropathies may lead to drying of the corneal surface, loss of epithelium, lysis of corneal stroma, and perforation. Entropion with trichiasis may also lead to corneal trauma and subsequent ulceration.
Tear insufficiency and ocular surface disorders may be associated with disruption of the epithelial barrier of the cornea and subsequent ulceration and perforation.
Inflammatory conditions affecting the cornea may also lead to melting and perforation. Rheumatoid arthritis may cause marginal melting or central melting and perforation.2 Wegener granulomatosis may cause similar changes. Inflammatory syndromes of unknown cause, including Mooren ulcer, Fuchs superficial marginal keratitis, and Terrien degeneration, may lead to corneal perforation. Corneal inflammation induced by bacterial toxins and abnormalities of meibomian secretions in phlyctenulosis and rosacea may lead to perforation as well. Conjunctival inflammatory disorders including Stevens-Johnson syndrome and mucous membrane pemphigoid may lead to entropion and trichiasis, with ultimate corneal disruption and perforation.
Other disorders that may be associated with corneal perforation include keratomalacia secondary to vitamin A deficiency and, very rarely, keratoconus with hydrops.3
DIAGNOSIS
The diagnosis of corneal perforation seems intuitively obvious, but this is not always the case. Usually, shallowing of the anterior chamber is present and a perforation site can be readily seen. However, at times the site of leakage of aqueous may be small or obscured by necrotic, infiltrated, or edematous tissue and the chamber may be only minimally shallow. In this instance, Seidel testing is appropriate. This is done by covering the cornea with concentrated fluorescein, which is quenched or fails to fluoresce. When diluted by a trickle of aqueous humor, however, it fluoresces under cobalt blue light at the slitlamp (Fig. 32-2A). The same information may be obtained by moistening a fluorescein strip and painting the unquenched fluorescein on the cornea and looking under cobalt blue light for a stream of clear aqueous flowing into the green fluorescence (Fig. 32-2B). At times, gentle pressure on the globe may be necessary to demonstrate tiny leaks, and sometimes a flat chamber or iris plugging the leak will lead to a negative test.
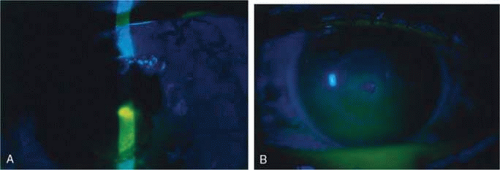 Figure 32-2. A. A perforated cornea showing a positive Seidel test. Under cobalt blue light, the fluorescein does not radiate in the slit beam where it is quenched. In the lower portion of the beam where there is a bright reflection, the fluorescein is unquenched and glowing a bright yellow-green. B. A perforated cornea showing clear aqueous diluting unquenched fluorescein. (Courtesy Elmer Tu, MD.) |
As important as making the diagnosis of the perforation is identifying the underlying cause. In trauma, the history is often sufficient to make the diagnosis. In infections, laboratory confirmation is important, and scraping and culture are often essential. Corneal biopsy may at times be necessary and may be part of the definitive treatment of the perforation, with the excised cornea at keratoplasty being used to make the diagnosis. External ocular examination including evaluation of lid function and anatomy, testing of corneal sensation, and evaluation of tear function may also help establish the etiologic diagnosis. In noninfectious inflammatory corneal melting, an evaluation for systemic inflammatory disease may be necessary.
TREATMENT
Treatment of corneal perforation has two goals. One is to re-establish the integrity of the globe, and the other is to treat the underlying problem so that ulceration and perforation will not recur.
With infectious processes, appropriate antimicrobial therapy must be initiated. Often, 24 hours of appropriate antibiotic treatment is carried out in bacterial perforations before definitively treating the perforation. In situations in which eyelid deformity has led to the problem, the eyelid abnormalities can be addressed concurrent with the treatment of the perforation. The same is true of patients with dry eyes in whom tear replacement, punctal occlusion, and other measures can be carried out at the same time as treatment of the perforation. With decreased corneal sensation, tarsorrhaphy can be performed after treatment of the perforation. In inflammatory conditions, immunosuppressant treatment may be necessary coincident with definitive repair and systemically or topically after repair.4
Definitive, that is, reparative, treatment of corneal perforation depends on the cause, location, size, and status of treatment of the underlying condition. Accompanying problems such as endophthalmitis and cataract may also play a role in the decision on definitive treatment.
Self-sealing perforations may need no reparative treatment. These perforations may occur with shelved lacerations or with small puncture wounds in which tissue swelling occludes the perforation tract. Wounds that are sealed by tissue prolapse usually require repair. Self-sealed wounds with tissue displacement may also be best repaired to reduce the likelihood of induction of irregular astigmatism.
Very small perforations with no associated tissue displacement may be amenable to the use of patching or soft contact lens placement. This is most likely to be effective in small leaks evident only with pressure or in descemetoceles in which tissue stabilization is essential to allow healing and in which the inciting process is under control.5 Small dry eye perforations are perhaps the most responsive to this approach. When soft contact lenses are used, frequent follow-up is essential, and more aggressive techniques may be necessary if this fails.
The use of tissue adhesives is an appealing approach to treatment of small perforations or descemetoceles with impending perforation. The advantage is that the adhesive may be applied under topical anesthesia at the slitlamp or in a minor procedure room. The disadvantages are that the glue may induce significant inflammation, may be uncomfortable for the patient, may adhere inadequately, may serve to harbor organisms once polymerized,6 and is often effective only in small perforations that can be readily dried. The tissue adhesives most commonly used in the United States are cyanoacrylates, usually isobutyl or higher alkyl compounds. None of these are approved for ophthalmic use by the Food and Drug Administration. 2-Octyl cyanoacrylate (Dermabond, Ethicon, Somerville, NJ) is approved by the U.S. Food and Drug Administration (FDA) for use on skin and has been effective in sealing corneal perforations. These substances polymerize rapidly when in contact with water. Various techniques have been described for the use of tissue adhesives. All require dbridement of necrotic tissue and epithelium surrounding the perforation, drying of the area to which the glue is to be applied, and application of the least amount of glue that can cover the defect. Drying of the defect can be carried out with cellulose sponges, and air or viscoelastic may be placed behind the perforation to separate tissue and reduce the fluid present.7,8 The glue itself may be applied to a small plastic disk and then placed over the perforation (Fig. 32-3), applied directly from the tip of a fine needle attached to a tuberculin syringe,9 or applied with a specially made plastic applicator (Squeez-ett, Ellman Manufacturing Co, Hewlett, NY).10,11 The glue may come off and need to be reapplied, at times repeatedly. Usually, because of the rough surface of the polymerized glue, a bandage soft contact lens is placed on the eye after the glue has polymerized. The glue may be left in place until there is obvious healing of the perforation, until the glue spontaneously loosens because epithelium has grown beneath it, or until a more definitive procedure such as keratoplasty is carried out. Fibrin adhesives (e.g., Tisseel, Immuno Canada, Ltd) may be used in a similar fashion but have less inherent strength than the cyanoacrylates and have been used less frequently in the United States.12 The advantages of the biodegradable fibrin adhesives are that they induce minimal stromal inflammation, foreign body reaction, or neovascularization, and no tissue necrosis.13 Thus, fibrin glue may be a better choice over cyanoacrylate adhesives if a penetrating keratoplasty is to be considered, as the subsequent risk for allograft rejection may be less. Both tissue adhesives are best suited for perforations of 2 mm or less in diameter; however, successful management of perforations up to 3 mm has been reported for both.14 A recent study comparing fibrin and cyanoacrylate tissue adhesives found that while both are effective in closing small perforations, fibrin glue allows quicker healing and induces less vascularization but also takes a much longer time for formation of the adhesive plug.15 Photopolymerized sealants are also being studied. These have the advantage of more controlled polymerization and hardening through laser irradiation after adhesive placement rather than the uncontrolled, very rapid polymerization seen with the cyanoacrylates.16
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


