 Questions
Questions
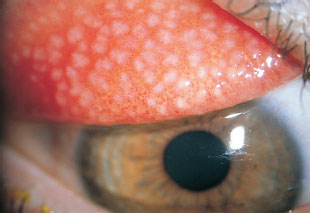
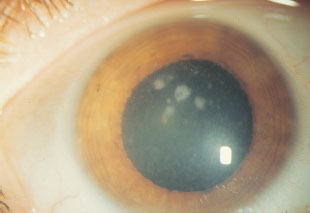
1. A 29-year-old contact lens wearer presents with pain, photophobia, decreased vision, and clinical findings as indicated in the below photograph. Which clinical feature is nearly universal in this disease process?
a. tearing.
b. hypopyon.
c. severe pain.
d. ring infiltrate.

2. With regard to the patient in question 1, which of the following is least likely to be discovered in this patient’s history?
a. use of homemade contact lens solution.
b. recent camping trip and exposure to open freshwater and soil.
c. significant suppuration early in the disease course.
d. recent treatment with topical antiviral and steroid.
3. Which of the following is TRUE regarding the condition in question 1?
a. Epithelial dendrites may be found.
b. Stromal infiltration should be primarily managed by debridement.
c. Primary infection usually occurs on skin and mucosal tissues innervated by the trigeminal nerve.
d. Gram-negative rods are seen on smears obtained by corneal scraping.
4. With regard to the patient in question 1, which of the following laboratory evaluations is LEAST useful in diagnosis?
a. smear stained with Giemsa.
b. smear stained with periodic acid-Schiff (PAS).
c. smear stained with calcofluor white.
d. nonnutrient agar with Staphylococcus overlay.
5. Which of the following is FALSE regarding the management of this disease described above?
a. The risk of recurrent infection after penetrating keratoplasty is very high if performed within the first year of onset.
b. Stromal infiltration often results in the need for prolonged treatment lasting 6 to 12 months.
c. There is no consensus in optimal therapy as antimicrobial agents most commonly used against this organism are effective in killing cysts but have reduced efficacy against the free-living trophozoite form.
d. Confocal microscopy is a useful adjuvant in detecting organisms in vivo.
6. A conjunctival inflammatory response characterized by multiple polygonal nodules with central fibrovascular cores is consistent with a
a. follicular response.
b. papillary response.
c. phlyctenular response.
d. ligneous response.
7. The least reliable location of a conjunctival papillary response for etiologic interpretation is the
a. inferior fornix.
b. superior fornix.
c. superior edge of superior tarsus.
d. inferior edge of superior tarsus.
8. The differential diagnosis of the patient in the photograph below includes all of the following except
a. contact lens–related conjunctivitis.
b. trachoma.
c. atopic keratoconjunctivitis.
d. ocular prosthesis–related conjunctivitis.
9. Clumps of calcific degeneration and eosinophils at the limbus are termed
a. Herbert’s pits.
b. von Arlt’s line.
c. Fuchs’ spots.
d. Horner-Trantas dots.
10. Rounded, depressed regions of necrotic limbal follicles are termed
a. Herbert’s pits.
b. von Arlt’s line.
c. Fuchs’ spots.
d. Horner-Trantas dots.
11. Mild contact lens–related GPC may be differentiated from an infectious follicular conjunctivitis by
a. the presence of itching in the former.
b. the presence of mucous and serous discharge in the latter.
c. injection of bulbar conjunctiva in the latter.
d. findings in the inferior conjunctival fornix of the latter.
12. Follicular conjunctivitides are typically more severe inferiorly than superiorly, except in
a. adult inclusion conjunctivitis.
b. epidemic keratoconjunctivitis (EKC).
c. trachoma.
d. medicamentosa.
13. The differential diagnosis for acute follicular conjunctivitis includes all of the following except
a. epidemic keratoconjunctivitis (EKC).
b. herpes simplex keratoconjunctivitis.
c. trachoma.
d. adult inclusion conjunctivitis.
14. The differential diagnosis for chronic follicular conjunctivitis includes all of the following except
a. EKC.
b. medicamentosa.
c. Parinaud’s oculoglandular syndrome.
d. trachoma.
15. Infectious etiologies of pseudomembranous or membranous conjunctivitis include all of the following except
a. Gonococcus.
b. herpes simplex.
c. adult inclusion conjunctivitis.
d. Candida.
16. Immunologic etiologies of a pseudomembranous or membranous conjunctivitis include all of the following except
a. ocular cicatricial pemphigoid (OCP).
b. vernal keratoconjunctivitis.
c. ligneous keratoconjunctivitis.
d. atopic keratoconjunctivitis.
17. Superficial opacification of the cornea in a horizontal fashion between the eyelid margins is best referred to as
a. superficial punctate keratitis.
b. micropannus.
c. band keratopathy.
d. gross corneal pannus.
18. The predominant cell forms seen in “muttonfat” KPs are
a. lymphocytes.
b. epithelioid histiocytes.
c. PMNs.
d. red blood cells.
19. Which of the following is an advantage of PRK when compared to LASIK?
a. reduced incidence of stromal haze.
b. more rapid epithelial healing.
c. reduced incidence of postoperative endophthalmitis.
d. reduced postoperative pain.
20. A corneal ulcer recalcitrant to routine treatment is rescraped for special staining and cultures. The Gram stain is reported as growing moderate diphtheroids. Which special stain is most likely to be of value in determining the actual diagnosis?
a. Ziehl-Neelsen stain.
b. Warthin-Starry stain.
c. Giemsa stain.
d. periodic acid-Schiff (PAS) stain.
21. The most common agent involved in mycotic ocular infections in the northern half of the United States is
a. Aspergillus.
b. Fusarium.
c. Penicillium.
d. Candida.
22. The most common agent involved in mycotic ocular infections in the southern half of the United States is
a. Aspergillus.
b. Fusarium.
c. Penicillium.
d. Candida.
23. The most basic difference between Candida and Fusarium is
a. Fusarium is a mold, and Candida is dimorphic.
b. Fusarium is dimorphic, and Candida is a mold.
c. Fusarium is a mold, and Candida is a yeast.
d. Fusarium as a yeast has pseudohyphae, whereas Candida has true hyphae.
24. The most common ocular manifestation of cryptococcal infection is
a. membranous conjunctivitis.
b. orbital cellulitis.
c. endogenous endophthalmitis.
d. ulcerative keratitis.
25. Factors that increase the difficulty of laboratory identification of fungal pathogens include all of the following except
a. inclusion of cycloheximide in various media.
b. fastidiousness of the fungal agents.
c. discarding of plates before full identification of fungal species.
d. confusion of pathogenic fungal species as contaminants.
26. Which of the following Epstein-Barr virus (EBV) antibodies does not peak in serum level within the first 6 to 12 weeks of infection?
a. viral capsid antigen IgM (VCA-IgM).
b. VCA-IgG.
c. early antigen-diffuse (EA-D).
d. Epstein-Barr nuclear antigen (EBNA).
27. Which of the following is NOT true regarding laser-assisted subepithelial keratomileusis (LASEK)?
a. There is no stromal flap created.
b. The procedure may offer increased comfort for the patient when compared to LASIK.
c. 20% ethanol can be used to trephine the epithelium.
d. The procedure has less haze associated with it than LASIK.
28. Biologic features of chlamydiae that render them closer to bacterial than viral life forms include all of the following except
a. nucleic acid content.
b. mechanism of replication.
c. cell wall properties.
d. full complement of organelles.
29. At what point do most flap folds occur after LASIK?
a. within 1 week.
b. after 2 weeks.
c. after 1 month.
d. after 1 year.
30. Which one of the following regarding louse infections of the eye is false?
a. Pediculus capitis and Phthirus pubis are the only organisms that infect the periocular structures.
b. Ocular irritation is due to injection of toxic louse saliva into lid tissue.
c. Sexual contact is felt to be the significant mode of transmission.
d. Eradication of organisms depends on suffocation, either by bland ointments or paralytic medications such as eserine.
31. The method of choice for documenting intracytoplasmic inclusion bodies is
a. Giemsa stain.
b. blood agar with Staphylococcus aureus cultures.
c. Sabouraud’s agar.
d. Ziehl-Neelsen stain.
32. Which of the following antivirals has in vivo activity against herpes simplex virus (HSV)?
a. idoxuridine.
b. vidarabine.
c. trifluridine.
d. acyclovir.
33. Which of the following is false regarding radial corneal incisions?
a. Radial incisions cause a local flattening of the cornea.
b. Radial incisions cause flattening 90° away from the meridian of the incision.
c. Radial incisions have a greater effect as they move further away from the visual axis.
d. Radial incisions have a greater effect the larger they are (up to 11 mm).
34. All of the following have been described as signs of antiviral toxicity except
a. follicular conjunctivitis.
b. anterior uveitis.
c. indolent corneal ulceration.
d. preauricular lymphadenopathy.
35. The drug of choice for presumed filamentous keratomycosis is
a. topical amphotericin.
b. oral ketoconazole.
c. topical clotrimazole.
d. topical natamycin.
36. The drug of choice for Aspergillus keratitis is
a. clotrimazole.
b. flucytosine.
c. natamycin.
d. amphotericin.
37. Which of the following organ systems is most likely to be the target of toxicity from the polyene class of antifungal agents?
a. central nervous system (CNS).
b. hepatic.
c. renal.
d. hematopoietic.
38. Which of the following organ systems is most likely to be the target of the imidazole class of antifungal agents?
a. central nervous system (CNS).
b. hepatic.
c. renal.
d. hematopoietic.
39. The cellular element generally responsible for inflammatory corneal damage is the
a. macrophage.
b. lymphocyte.
c. polymorphonuclear leukocyte (PMN).
d. eosinophil.
40. Which of the following statements regarding intracorneal rings (ICRs) is false?
a. One advantage of ICR implantation is the reversible nature of the procedure.
b. Decreased corneal sensation can be a postoperative complication.
c. The most common complication, corneal perforation, can lead to severe visual loss.
d. More than 90% of patients have <1 D change in refraction at 1-year postoperative follow-up.
41. The topical steroid preparation with the greatest antiinflammatory activity within the cornea is
a. prednisolone phosphate 1.0%.
b. dexamethasone phosphate 1.0% ointment. prednisolone acetate 1.0%.
d. dexamethasone alcohol 0.1% suspension.
42. A patient presents 6 hours after receiving a prescription for topical antibiotic for a suspected bacterial blepharoconjunctivitis. The patient complains of itching and tearing, and an examination documents severe chemosis and mild hyperemia. The most likely diagnosis is
a. anaphylactoid reaction.
b. toxic follicular conjunctivitis.
c. toxic papillary conjunctivitis.
d. contact allergic reaction.
43. A patient presents approximately 6 days after daily use of antibiotic ointment following cataract surgery. The patient describes a gradual onset of scaling and itching of the skin and increasing redness of the eye. The hypersensitivity pattern most likely at play is
a. type I.
b. type II.
c. type III.
d. type IV.
44. The two organisms most frequently involved in phlyctenulosis are
a. Coccidioides immitis and Mycobacterium tuberculosis.
b. Coccidioides and Staphylococcus.
c. Chlamydia trachomatis and Staphylococcus.
d. Mycobacterium tuberculosis and Staphylococcus.
45. The most common cause of hyperacute purulent conjunctivitis is
a. Haemophilus influenzae.
b. Neisseria meningitidis.
c. Streptococcus pneumoniae.
d. Neisseria gonorrhoeae.
46. The only bacterial conjunctivitis that routinely leads to preauricular lymphadenopathy is
a. Haemophilus influenzae.
b. Neisseria meningitidis.
c. Streptococcus pneumoniae.
d. Neisseria gonorrhoeae.
47. Which of the following would be the most appropriate treatment of culture-proven gonococcal conjunctivitis?
a. ceftriaxone 1 g intramuscularly daily for 5 days and doxycycline orally twice daily for 3 weeks.
b. topical penicillin G four times daily with doxycycline 100 mg orally twice daily for 1 week.
c. topical penicillin G four times daily and topical tetracycline four times daily for 1 week.
d. ceftriaxone 1 g intramuscularly daily for 5 days.
48. A child presents with the findings below and associated inferior follicular conjunctivitis. The most likely diagnosis is
a. phlyctenulosis.
b. staphylococcal blepharoconjunctivitis.
c. molluscum contagiosum.
d. primary herpes simplex dermatitis.

49. Classic epidemic keratoconjunctivitis (EKC) is typically caused by
a. enterovirus type 70.
b. adenovirus types 3 and 7.
c. coxsackievirus A24.
d. adenovirus types 8 and 19.
50. The most important element in the management of a patient with EKC is
a. fastidious hygiene.
b. topical trifluridine drops.
c. topical bacitracin.
d. topical prednisolone.
Successful long-term management of adult inclusion conjunctivitis includes
a. recurrent oral tetracycline therapy preparation.
c. conjunctival transplantation.
d. examination with treatment, if necessary, of personal contacts.
52. Important differences between neonatal inclusion conjunctivitis and adult inclusion conjunctivitis include all of the following except
a. more prominent follicular response in neonates.
b. more discharge in neonates.
c. more prominent cytoplasmic inclusion bodies in neonates.
d. better response to topical therapy in neonates.
53. Which of the following disorders is most likely to respond quickly to topical antihistamine therapy?
a. season allergic conjunctivitis.
b. phlyctenulosis.
c. atopic keratoconjunctivitis.
d. giant papillary conjunctivitis (GPC).
54. For which disorder is chronic use of systemic antihistamine most important?
a. season allergic conjunctivitis.
b. phlyctenulosis.
c. atopic keratoconjunctivitis.
d. giant papillary conjunctivitis (GPC).
55. Features distinguishing atopic keratoconjunctivitis from vernal keratoconjunctivitis include all of the following except
a. age range of typically affected patient.
b. seasonal variations of incidence.
c. presence of extensive conjunctival and corneal scarring.
d. presence of eosinophils in conjunctival scrapings.
56. To secure the diagnosis of atopic keratoconjunctivitis, it is critical to inquire about a previous or active history of
a. asthma.
b. sinusitis.
c. vesicular rash consistent with HSV.
d. eczema.
57. An obese 35-year-old man presents to an ophthalmologist complaining of increasing redness and irritation of his left eye (pictured below), progressive over the previous 4 to 6 months. Examination discloses mildly edematous and erythematous left eyelids with mild conjunctival injection and scant mucus discharge. The conjunctival findings are much more prominent superiorly. The right eye appears normal. With this patient, the critical historical feature to inquire about is
a. use of over-the-counter eye medications.
b. any history of previous sexually transmitted diseases.
c. which side of his body he generally chooses to sleep on.
d. any previous history of allergic disorders.

58. The two leading causes of corneal blindness in the United States are
a. trachoma and trauma.
b. trachoma and herpes simplex.
c. trauma and herpes simplex.
d. trachoma and onchocerciasis.
59. Latent type 1 HSV (responsible for recurrent orofacial infection) generally resides in the
a. oculomotor nucleus.
b. gasserian ganglion.
c. sphenopalatine ganglion.
d. superior cervical ganglion.
60. Clinical features differentiating primary from recurrent HSV infection include all of the following except
a. prominent follicular membranous conjunctivitis.
b. preauricular lymphadenopathy.
c. duration and size of corneal dendrites.
d. vesicular blepharitis.
61. Potential outcomes of overtreatment with topical antivirals for HSV keratitis include all of the following except
a. sterile corneal ulceration.
b. pseudodendrites.
c. punctate keratitis with photophobia.
d. bacterial superinfection.
62. Two weeks after initial diagnosis and topical therapy of HSV epithelial keratitis, a patient returns with a 4 mm, oval, central epithelial defect with smooth rolled edges. Factors that may be important in the pathogenesis of this finding include all of the following except
a. active intraepithelial virus replication.
b. underlying stromal inflammation.
c. overuse of prescribed topical antivirals.
d. impaired corneal sensation.
63. Which of the following is not seen as part of the spectrum of HSV disciform keratitis?
a. Descemet’s folds.
b. peripheral anterior synechiae.
c. mild anterior uveitis with KP.
d. glaucoma.
64. A circular, superficial distribution of neutrophils around an area of corneal edema or inflammation is called
a. Wessely ring.
b. disciform keratitis.
c. metaherpetic ulcer.
d. ring ulcer.
65. All of the following features of corneal dendrites favor the diagnosis of herpes zoster ophthalmicus except
a. a large, frequently branching dendrite.
b. a dendrite with no terminal bulb.
c. coarse, ropy dendrites with blunt ends.
d. a dendrite with dull fluorescein and no rose-bengal staining.
66. Which of the following is not a systemic risk factor for the development of bacterial keratitis?
a. drug abuse.
b. diabetes mellitus.
c. vitamin deficiency.
d. hypertension.
67. Which of the following is not considered an independent risk factor for the development of fungal keratitis?
a. prolonged use of topical corticosteroids.
b. previous history of herpetic keratitis.
c. prolonged use of broad-spectrum topical antibiotics.
d. corneal trauma.
68. Leading causes of interstitial keratitis (IK) in the United States include all of the following except
a. sarcoidosis.
b. lepromatous leprosy.
c. herpes zoster virus (HZV).
d. syphilis.
69. Cogan’s syndrome is frequently associated with which systemic disorder?
a. polyarteritis nodosa.
b. Wegener’s granulomatosis.
c. rheumatoid arthritis.
d. systemic lupus erythematosus.
70. Which one of the following regarding Thygeson’s superficial punctate keratitis is false?
a. The presenting symptom is typically photophobia or tearing.
b. There is usually an associated follicular conjunctivitis.
c. The corneal deposits may resemble those of EKC.
d. Topical steroids have been used for symptomatic relief but may prolong the natural history of the disorder.
71. There is a definite association of superior limbic keratoconjunctivitis (SLK) with
a. valvular heart disease.
b. thyroid disease.
c. inflammatory bowel disease.
d. systemic lupus erythematosus.
72. Which class of chemicals constitutes the greatest threat for ocular injury?
a. solvents.
b. petroleum products.
c. acids.
d. alkali.
73. After thorough and copious irrigation of the conjunctival fornices, the next most important step in initial management of a patient with a chemical burn is
a. topical steroid agents.
b. topical antibiotic agents.
c. debridement of any foreign bodies.
d. topical ascorbate.
74. The primary goal in intermediate therapy of chemical burns is
a. normalization of intraocular pressure.
b. reestablishment of limbal blood flow.
c. control of intraocular inflammation.
d. reepithelialization of the corneal surface.
75. Which one of the following regarding episcleritis is false?
a. Both nodular and diffuse forms have been described.
b. The majority of cases are sectoral.
c. The majority of cases will be recurrent.
d. The condition may lead to scleritis if not promptly treated.
76. The most benign form of scleritis is
a. diffuse anterior scleritis.
b. nodular anterior scleritis.
c. necrotizing scleritis with inflammation.
d. scleromalacia perforans.
77. The scleritis associated with the gravest systemic prognosis is
a. diffuse anterior scleritis.
b. nodular anterior scleritis.
c. necrotizing scleritis with inflammation.
d. scleromalacia perforans.
78. The scleritis most likely to be associated with rheumatoid arthritis is
a. diffuse anterior scleritis.
b. nodular anterior scleritis.
c. necrotizing scleritis with inflammation.
d. scleromalacia perforans.
79. Infectious scleritis may be seen due to all of the following except
a. Chlamydia.
b. syphilis.
c. tuberculosis.
d. herpes zoster.
80. Agents helpful in the medical management of autoinflammatory sclerokeratitis include all of the following except
a. topical indomethacin.
b. oral prednisone.
c. subtenon’s injection of corticosteroid.
d. cyclosporine A.
81. The most common cause of acute, painful enlargement of the lacrimal gland is
a. sarcoidosis.
b. Sjögren’s syndrome.
c. bacterial dacryoadenitis.
d. herpes zoster virus.
82. The most common cause of painless, bilateral enlargement of lacrimal glands is
a. sarcoidosis.
b. Sjögren’s syndrome.
c. bacterial dacryoadenitis.
e. herpes zoster virus (HZV).
83. Mikulicz’s syndrome refers to the combination of chronic dacryoadenitis with
a. rheumatoid arthritis.
b. enlargement and inflammation of the parotid glands.
c. keratoconjunctivitis sicca.
d. dacryocele.
84. The treatment of choice for the most common cause of chronic canaliculitis is
a. topical tetracycline for 2 weeks.
b. oral tetracycline for 3 weeks.
c. surgical evacuation of the canaliculus.
d. topical corticosteroids.
85. A patient presents with a tender mass below the medial canthal tendon and mucopurulent discharge from the inferior canaliculus. One week of oral antibiotic treatment and warm compresses leads to an increase in size and fluctuance of the mass. The next step in treatment should be
a. change in antibiotic agents.
b. increasing the frequency of dosage of the antibiotic agent.
c. probing and irrigation of the nasolacrimal system.
d. incision and drainage of the fluctuant mass.
86. A 2-month-old infant with unilateral epiphora in the left eye is brought to the ophthalmologist by her parents. Gentle compression of the lacrimal sac produces reflux of mucus from the canaliculi, but only on the left. There is obviously increased tear flow on the left as well. The next step should probably be
a. reassurance with once daily antibiotic ointment and gentle medial canthal massage.
b. probing and irrigation of the nasolacrimal system on the left.
c. incision and drainage of the lacrimal sac.
d. oral antibiotics.
87. A 13-month-old infant with chronic epiphora and discharge in the left eye is brought to the ophthalmologist by his parents. Gentle massage of the medial canthal area produces a reflux of mucus from the left canaliculi. The next step in management should be
a. reassurance with once daily antibiotic ointment and gentle medial canthal massage.
b. probing and irrigation of the nasolacrimal system on the left.
c. incision and drainage of the lacrimal sac.
d. oral antibiotics.
88. Which of the following with regard to wavefront analysis and wavefront aberrations is true?
a. Wavefront analysis is only used to describe reference spheres and cannot be used in patients with irregular astigmatism.
b. A penetrating keratoplasty using eight interrupted sutures will produce a four-leaf clover.
c. Spherical aberration occurs when central rays focus more in front of peripheral rays, leading to night myopia in some postoperative LASIK patients.
d. An eye with no astigmatism will have no wavefront aberration.
89. In which of the following conditions would lamellar keratoplasty be least efficacious?
a. Terrien’s marginal degeneration.
b. pellucid marginal degeneration.
c. Salzmann nodular degeneration.
d. Fuchs endothelial dystrophy.
90. Which of the following statements accurately represents Munnerlyn’s formula?
a. The ablation depth (in microns) is equal to the (diopters of myopia divided by 3) multiplied by the square of the optical zone (in millimeters).
b. The ablation depth (in microns) is equal to the (diopters of myopia multiplied by 3) divided by the square of the optical zone (in millimeters).
c. The ablation depth (in microns) is equal to the (diopters of myopia divided by 5) multiplied by the cube of the optical zone (in millimeters).
d. The ablation depth (in microns) is equal to the (diopters of myopia multiplied by 3) divided by the cube of the optical zone (in millimeters).
91. Which of the following is not a common feature of a conjunctival papilloma?
a. hyperkeratosis.
b. acanthosis.
c. parakeratosis.
d. anaplasia.
92. A 33-year-old man presents to an ophthalmologist complaining of a “growth” on his eyelid. He maintains that the lesion developed over the preceding 4 weeks and is nontender. He produces a driver’s license photo from 4 months earlier, which shows normal eyelids. Examination discloses a 3.5-cm round elevated lesion of the right lower eyelid with a central depressed area and debris within. There is no pigmentation. The most likely diagnosis is
a. seborrheic keratosis.
b. actinic keratosis.
c. keratoacanthoma.
d. basal cell carcinoma.
93. Which one of the following regarding seborrheic keratosis is false?
a. It is a lesion most commonly seen in elderly people.
b. The lesion must be carefully distinguished from actinic keratosis.
c. Texturally, the lesion appears dry and scaly.
d. Histopathologically, there is prominent dyskeratosis and hyperpigmentation in a papillary growth pattern.
94. With regard to the photograph below, which one of the following true?
a. Growth is typically explosively rapid.
b. In 25%, the conjunctiva is primarily involved with secondary skin involvement.
c. The upper eyelid is affected more frequently than the lower eyelid.
d. Nuclei at the periphery of tumor cell nests retain polarity with palisading.

95. Which of the following growth patterns of basal cell carcinoma carries the worst prognosis?
a. fibrosing.
b. cystic.
c. adenocystic.
d. nodular.
96. Which location of basal cell carcinoma carries the poorest prognosis?
a. lateral lower lid.
b. lateral canthus.
c. upper lid.
d. medial canthus.
97. Basal cell carcinoma causes the most significant systemic morbidity and mortality via
a. hematogenous metastasis to the brain.
b. local invasion of skull and central nervous system (CNS).
c. lymphatic metastasis.
d. hematogenous metastasis to liver.
98. Which one of the following regarding squamous cell carcinoma of the eyelid is false?
a. Growth pattern is usually rapid.
b. Chronic actinic exposure plays a role in its development.
c. The upper eyelid is more frequently involved than the lower eyelid.
d. Metastatic potential is greater than for basal cell carcinoma.
99. A 68-year-old woman complains to her ophthalmologist that her stye just will not go away, despite 3 months of warm compresses and two surgical drainages. She undergoes full-thickness biopsy of her lower lid; a light microscopic section is shown below. Which of the following is true regarding her situation?
a. The disorder typically affects middle-aged or elderly people.
b. Prompt drainage of the initial chalazion would have been curative.
c. The lesion is likely derived from Moll’s glands.
d. Mohs’ micrographic techniques can be curative at this stage.
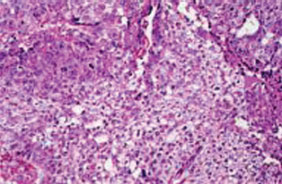
100. The biopsy specimen from the patient in question 99 should also have undergone which one of the following histopathologic techniques?
a. electron microscopy.
b. cell surface marker studies.
c. cellular adhesion studies.
d. frozen section processing.
101. Adnexal tumors of hair follicle origin include all of the following except
a. syringoma.
b. trichoepithelioma.
c. trichilemmoma.
d. pilomatrixoma.
102. Which of the following tumors is most likely to calcify?
a. syringoma.
b. trichoepithelioma.
c. trichilemmoma.
d. pilomatrixoma.
103. Which one of the following regarding nevi is false?
a. Pigmentation and growth generally increase around the onset of puberty.
b. With time, nevi tend to advance superficially, toward the surface epithelium.
c. Junctional activity carries the greatest potential for malignant transformation.
d. Subepithelial or dermal activity carries the least potential for malignant transformation.
104. Which one of the following regarding Kaposi’s sarcoma is false?
a. The disorder is generally more aggressive and lethal in the immunocompromised individual.
b. The disorder is endemic in Central Africa.
c. In the setting of normal immune regulation, the disease typically affects the lower extremities of older men.
d. Radiation currently plays no role in the management of ocular Kaposi’s sarcoma.
105. Potential etiologies for multiple discrete eyelid nodules include all of the following except
a. juvenile xanthogranuloma.
b. Hand-Schüller-Christian disease.
c. xanthelasma.
d. syringoma
106. A 32-year-old man from North Carolina presents to an ophthalmologist for routine examination. The ophthalmologist notes bilateral bulbar leukoplakia at the nasal and temporal limbus. On further questioning, the patient reports that these lesions have been present for many years and that several of his siblings have similar find-ings. Examination of which of the following is most likely to confirm the probable diagnosis?
a. the patient’s fundus.
b. history of sunlight exposure.
c. intertriginous areas of the patient’s body.
d. the patient’s mouth.
107. Epithelial neoplasms of the conjunctiva and cornea bear striking pathologic similarities to neoplasms of the
a. stomach.
b. ovary.
c. cervix.
d. urinary bladder.
108. Which one of the following is not a risk of clear lens exchange as a corrective treatment for high myopia?
a. endophthalmitis.
b. stromal flap dehiscence.
c. IOL dislocation or decentration.
d. retinal detachment.
109. The most common location of origin for corneal intraepithelial neoplasia is
a. the inferior fornix.
b. the superior fornix.
c. the limbus.
d. the bulbar conjunctiva.
110. The key structure preventing local invasion of squamous cell carcinoma of the cornea is
a. corneal stroma.
b. Bowman’s layer.
c. endothelium.
d. Descemet’s membrane.
111. Which one of the following regarding conjuncti-val nevi is false?
a. Because of the absence of a dermal layer, conjunctival nevi are of the junctional variety only.
b. Conjunctival nevi are frequently cystic.
c. Due to sudden enlargement, mucus secretion within nevi can lead to the false impression of malignant transformation.
d. Conjunctival nevi are more frequently amela-notic or lightly pigmented than skin nevi.
112. With regard to the diagnosis associated with the photograph below, which of the following statements is accurate?
a. This entity is equally common among Caucasians, African Americans, and Asians.
b. This entity is more common in Caucasians, but malignant transformation to melanoma is more common in African Americans and Asians.
c. This entity is more common in Asians and African Americans, in whom malignant transformation is more common.
d. This entity is more common in Asians and African Americans, but malignant transformation is more common in Caucasians.

113. Which of the following regarding primary acquired melanosis of the conjunctiva is not true?
a. The pigmented lesions represent proliferation of intraepithelial melanocytes.
b. It is primarily a disorder of the middle-aged and elderly.
c. The most troublesome sign (indicating potential malignant transformation) is nodular thickening.
d. The most frequently involved region is the palpebral conjunctiva.
114. The anterior segment dysgeneses reflect developmental abnormalities related to what cell line?
a. surface ectoderm.
b. neuroectoderm.
c. neural crest.
d. mesoderm.
115. An abnormally prominent Schwalbe’s line is referred to as
a. posterior embryotoxon.
b. Rieger’s anomaly.
c. Peters’ anomaly.
d. Axenfeld’s anomaly.
116. A patient presents with bilateral glaucoma. Gonioscopy reveals an anteriorly displaced, prominent Schwalbe’s line with attached iris processes and slit lamp exam is significant for iris stromal hypoplasia and polycoria. There are no other obvious systemic abnormalities noted. This patient’s clinical condition would be most correctly termed
a. posterior embryotoxon.
b. Axenfeld-Rieger syndrome.
c. Peters anomaly.
d. ICE syndrome.
117. All cases of Peters’ anomaly share which of the following features?
a. Central absence of Descemet’s membrane and endothelium.
b. cataract or ectopia lentis.
c. posterior embryotoxon.
d. polycoria.
118. Which of the following regarding corneal birth trauma is true?
a. There are no means of distinguishing the findings from those of congenital glaucoma.
b. The presenting finding is typically corneal stromal edema in the first postnatal week and may recur later in life.
d. If corneal edema clears, there are no permanent physical findings.
c. If corneal edema clears, there are no visual consequences.
119. Which one of the following regarding pingueculae is false?
a. The agent most frequently implicated in the pathogenesis is ultraviolet light.
b. Histologically, accumulation of abnormal elastin material can be observed.
c. The nasal limbus is more frequently involved than the temporal limbus.
d. Surgical excision is generally not pursued unless there are cosmetic or comfort issues.
120. Which of the following regarding pterygia is/ are true?
a. Epidemiologically and histologically, pterygia are clearly extensions of pingueculae.
b. Corneal invasion is limited in depth by the epithelial basement membrane.
c. Mild inflammation and copper lines at the leading edge are typically seen.
d. Like pingueculae, surgical intervention is usually mandated for comfort.
121. Methods to diminish the recurrence rate of pterygia following excision include all of the following except
a. conjunctival autotransplantation.
b. beta-irradiation.
c. topical mitomycin C.
d. 5-fluorouracil.
122. The stain of choice for suspected amyloid deposits of the external eye is
a. hematoxylin and eosin (H&E).
b. congo red.
c. periodic acid-Schiff (PAS).
d. alcian blue.
123. A conjunctival deposit of amyloid is examined via biopsy and stained with Congo red. As a polarizing filter between the illuminating light and the specimen is rotated 90°, the amyloid deposits seem to change from cherry red to apple green. This phenomenon is known as
a. birefringence.
b. autofluorescence.
c. metachromasia.
d. dichroism.
124. The most common form of conjunctival amyloidosis is
a. primary localized.
b. primary systemic.
c. secondary localized.
d. secondary systemic.
125. The most common type of eyelid amyloidosis is
a. primary localized.
b. primary systemic.
c. secondary localized.
d. secondary systemic.
126. Corneal forms of amyloidosis include all of the following except
a. limbal girdle of Vogt.
b. primary gelatinous droplike dystrophy.
c. lattice dystrophy type I.
d. Meretoja’s syndrome.
127. Which one of the following regarding corneal arcus is false?
a. The deposits generally begin in the interpalpebral fissure and spread superiorly and inferiorly with time.
b. Incidence approaches 100% in patients over the age of 80.
c. There is generally a lucent zone between the limbus and the peripheral edge of the arcus.
d. Unilateral corneal arcus may be seen in the setting of contralateral high-grade carotid stenosis.
128. A 65-year-old woman is examined as part of a routine annual checkup. On retroillumination of the cornea, fleck-like deposits in the deep corneal stroma are detectable centrally. Visual acuity is normal, and there are no other ocular findings. The most likely diagnosis is
a. Hassall-Henle bodies.
b. cornea guttae.
c. cornea farinata.
d. central cloudy dystrophy.
129. Clinically and histopathologically, the earliest calcium deposits in band keratopathy are located in the
a. horizontal peripheral cornea, Descemet’s membrane.
b. vertical peripheral cornea, Descemet’s membrane.
c. vertical peripheral cornea, Bowman’s layer.
d. horizontal peripheral cornea, Bowman’s layer.
130. The two most commonly encountered chemical compositions of band keratopathy are
a. urate and cholesterol.
b. cholesterol and calcium.
c. urate and calcium.
d. cholesterol and amyloid.
131. Which of the following corneal degenerations is generally seen only in association with corneal neovascularization?
a. Salzmann’s nodular degeneration.
b. spheroidal degeneration.
c. Coats’ white ring.
d. lipid keratopathy.
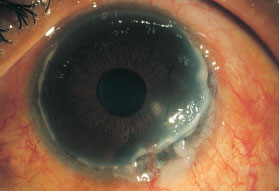
132. A 63-year-old woman presents with a red, painful right eye (photographed below). Examination discloses an ulcerative, circumferential marginal keratitis with a leading, undermined edge and early neovascularization. Which one of the following regarding the condition is false?
a. There is dysregulation in both cellular and humoral immunity.
b. A milder, less painful variant may be seen in young African American men.
c. Medical management might include oral prednisone, cyclophosphamide or methotrexate.
d. An evaluation for connective tissue disease is mandatory.
133. The most common anterior corneal dystrophy is
a. Meesman dystrophy.
b. map-dot-fingerprint dystrophy.
c. central cloudy dystrophy.
d. Reis-Bückler dystrophy.
134. Which one of the following regarding anterior membrane dystrophy is false?
a. Examination of family members may disclose a familial pattern.
b. Abnormalities in basement membrane production are manifest as map and fingerprint lines.
c. Dots represent calcification of epithelial debris.
d. Symptoms are generally related to defective epithelial adherence.
135. Treatment modalities useful in symptomatic anterior membrane dystrophy include all of the following except
a. copious lubrication.
b. hypertonic saline ointments.
c. stromal puncture.
d. penetrating keratoplasty (PK).
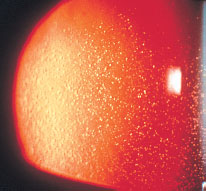
136. A 28-year-old patient presents to an ophthalmologist complaining of irritation and episodic blurry vision bilaterally. Slit-lamp examination reveals intraepithelial bubbles that are too numerous to count and that are visible only on retroillumination (photographed below). These bubbles appear entirely transparent. A lamellar keratoplasty specimen should reveal
a. areas of reduplicated basement membrane and trapped epithelial cells.
b. PAS staining of epithelially contained “peculiar substance.”
c. focal areas of absence of basement membrane and fibrocellular invasion of Bowman’s zone.
d. hyaline deposits in the anterior stroma.
137. Which of the following corneal dystrophies is the most disabling visually?
a. anterior membrane dystrophy.
b. Reis-Bückler dystrophy.
c. Meesman dystrophy.
d. central cloudy dystrophy.
138. A 29-year-old woman undergoes a routine ophthalmic examination. Visual acuity is normal. Slit-lamp examination discloses numerous crumblike deposits in the anterior corneal stroma as shown in the photograph below, which are bilaterally symmetric, densest centrally. Intervening stroma is clear. Which one of the following is likely to be false?
a. Careful history may elicit a history of recurrent corneal erosions.
b. Examination of family members will disclose similar findings.
c. Visual acuity generally remains normal throughout life.
d. Histopathologic review will reveal hyaline deposits on the Masson trichrome stain.

139. A 38-year-old man presents to the ophthalmologist complaining of gradual diminution in vision bilaterally. Visual acuity is 20/100 in both eyes. Slit-lamp examination reveals focal gray deposits in the stroma, densest centrally but extending to the limbus. Intervening areas of stroma have an ill-defined haze as photographed at the right column. Which one of the following regarding this condition is likely to be false?
a. The patient’s siblings may be affected, but his offspring are unlikely to be.
b. It is the stromal dystrophy most likely to be associated with recurrent erosions.
c. It is the least common of the stromal dystrophies.
d. A blood test may aid in the diagnosis.
140. A 59-year-old woman presents to the ophthalmologist complaining of gradual loss of vision in each eye over the previous 5 years. Visual acuity is 20/80 in both eyes. Slit-lamp examination reveals the findings represented in the photograph shown at the top of the next page. The peripheral corneal is clear. Both eyes are symmetrically involved. Which one of the following statements is likely to be false?
a. Each of the patient’s children has a 50% chance of being affected with the same disorder.
b. Recurrence in donor corneas following penetrating keratoplasty is more likely with this disorder than any other related disorder.
c. The patient, on further questioning, will probably complain of a history of double vision or facial droop.
d. With polarizing filters on both sides of the specimen, light microscopic evaluation of the patient’s corneal button following keratoplasty will reveal birefringence of the abnormal deposits.
141. Which of the stromal dystrophies is photographed below and may be associated with systemic hyperlipidemia?
a. granular dystrophy.
b. central crystalline dystrophy.
c. fleck dystrophy.
d. central cloudy dystrophy of Francois.
142. Which one of the stromal dystrophies may be associated with keratoconus, atopy, or pseudox-anthoma elasticum?
a. granular dystrophy.
b. central crystalline dystrophy.
c. fleck dystrophy.
d. central cloudy dystrophy of Francois.
143. Which one of the following stromal dystrophies is least likely to be associated with poor vision?
a. granular dystrophy.
b. lattice dystrophy.
c. macular dystrophy.
d. central cloudy dystrophy of Francois.
144. Which one of the following regarding Fuchs’ endothelial dystrophy is false?
a. At one end of the spectrum are corneal guttata; at the other are epithelial bullae.
b. Symptoms usually consist of blurry vision and pain, worse in the evening.
c. Typically, stromal edema develops before epithelial abnormalities are noted.
d. Penetrating keratoplasty (PK) may need to be undertaken at the time of cataract surgery, even though corneal symptoms are minimal or nonexistent.
145. An infant is born with bilaterally thickened, hazy corneas with epithelial edema as demonstrated in the photograph below. Corneal diameters are normal. There is associated nystagmus. Which one of the following regarding this condition is false?
a. Intraocular pressure (IOP) is likely to be elevated.
b. Another variant of the disorder exists in which there is no nystagmus and the onset is later.
c. Features distinguishing this disorder from congenital hereditary stromal dystrophy include corneal thickening and epithelial edema.
d. Descemet’s membrane may be thickened but there are no guttata.

146. A 28-year-old man presents claiming “someone said my eyes look funny.” Visual acuity is normal bilaterally. Slit-lamp examination reveals multiple abnormalities on the posterior corneal surface, including groups of blisterlike deposits, scalloped banding, and irregular maplike grayish deposits on the endothelium with focal stromal edema. These findings are bilateral, as is corec-topia, with the pupil drawn temporally. Careful questioning fails to reveal any family history of eye disorders. Which one of the following regarding this condition is probably false?
a. Careful examination of a sibling may reveal milder but similar findings.
b. The most likely diagnosis is iridocorneal endothelial syndrome (ICE).
c. Gonioscopy may reveal anteriorly placed peripheral anterior synechiae.
d. Histopathologic findings of the eye, if reviewed, would reveal an abnormally pro-liferative corneal endothelium with desmo-somes and microvilli.
147. The most common finding in the contralateral eye of a patient with unilateral keratoconus is
a. Vogt’s striae.
b. horizontal breaks in Descemet’s membrane.
c. fleck dystrophy.
d. myopia with high astigmatism.
148. The time of greatest progression of keratoconus is during the
a. first decade.
b. second decade.
c. third decade.
d. The condition is generally static.
149. A patient with known keratoconus presents to the ophthalmologist with a sudden decrease in vision and tearing from the right eye. Which one of the following regarding this situation is probably false?
a. The “tearing” represents spontaneous perforation and demands immediate surgery.
b. The corneal findings at the slit lamp may slowly resolve with time.
c. There may be considerable associated pain.
d. Typically, the condition is painless.
150. A patient presents to the ophthalmologist unhappy with his latest refraction. Examination discloses vision of 20/50 with each eye through his new pair of spectacles. This improves to 20/25+ with a pinhole over either lens. Keratometry reveals 45.5 D at 180° and 53.5 D at 90° in each eye. The next logical intervention should be
a. photorefractive keratectomy.
b. toric soft contact lens fitting.
c. rigid gas permeable contact lens fitting.
d. penetrating keratoplasty.
151. Contact lens fitting is usually most challenging for patients with
a. keratoconus.
b. keratoglobus.
c. pellucid marginal degeneration.
d. posterior keratoconus.
152. At what point does diffuse lamellar keratitis post-LASIK surgery typically manifest?
a. 6 to 12 hours postoperatively.
b. 24 to 48 hours postoperatively.
c. Within the first week postoperatively.
d. Within the first month after LASIK.
153. Which one of the following regarding tear defi-ciency states is false?
a. Classic signs include ropy mucus discharge, corneal filaments, and punctate rose bengal staining in the exposure zone.
b. Pathophysiologically, the problem is a loss of adequate tear volume.
c. Patients may complain of epiphora.
d. Tests to be considered in the evaluation of potential tear deficiency include Schirmer’s tests, rose bengal stain, and observation of tear breakup time.
154. A patient presents with complaints typical for dry eye syndrome. Schirmer’s testing with and without anesthesia is normal. A hypothesis of tear deficiency state due to inadequate tear lipid or mucus layer would be best confirmed by
a. tear breakup time testing.
b. tear osmolarity testing.
c. rose bengal staining.
d. tear lysozyme testing.
155. Classic Sjögren’s syndrome consists of keratoconjunctivitis sicca, xerostomia, and
a. eczema.
b. arthritis.
c. Raynaud’s phenomenon.
d. SS-A and SS-B autoantibodies.
156. Patients with primary Sjögren’s syndrome are not at increased risk for subsequent development of
a. autoimmune thyroiditis.
b. Waldenström’s macroglobulinemia.
c. lymphoma.
d. adenoid cystic carcinoma of the lacrimal gland.
157. A patient with established dry eye syndrome is suffering persistent discomfort and blurry vision despite hourly topical artificial tears. The next most appropriate intervention might be
a. warm compresses to both eyes twice a day.
b. lateral tarsorrhaphy.
c. a trial of temporary inferior punctal occlusion with collagen plugs.
d. permanent thermal punctal occlusion for all four puncta.
158. A patient with a history of previous severe herpes zoster keratitis presents with Bell’s palsy and decreased corneal sensation. Appropriate intervention at this point should include
a. hourly artificial tears.
b. bandage contact lens.
c. lateral tarsorrhaphy.
d. conjunctival flap.
159. Which one of the following regarding rosacea is false?
a. It is more common in fair-skinned races.
b. Facial lesions include telangiectasis, papules, pustules, and comedones.
c. Nasal skin thickening (rhinophyma) is a late sign.
d. Alcohol consumption can aggravate the disorder.
160. A 42-year-old man of Irish descent presents to the ophthalmologist complaining that his eyes have been red for several months. Examination discloses multiple brow and cheek telangiectasias with small papillary rash at the tip of the nose. All four eyelids are thickened with telangiectasias crossing the lid margin. There is focal meibomian gland loss. Both eyes have moderate conjunctival injection, and the right eye has a marginal infiltrate under intact epithelium at the inferior temporal limbus. An effective treatment strategy might include all of the following except
a. topical bacitracin ointment to the eyelids twice a day.
b. topical prednisolone 1.0% to the right eye every 2 to 4 hours.
c. topical metronidazole for the skin findings.
d. long-term oral doxycycline.
161. The mucous membrane most frequently involved in cicatricial pemphigoid is
a. oral.
b. conjunctival.
c. pharyngeal.
d. genitourinary.
162. Which one of the following regarding the clinical features of ocular cicatricial pemphigoid (OCP) is false?
a. Women are more commonly affected than men.
b. The disease most typically presents as insidious, bilaterally asymmetric chronic conjunctivitis.
c. Chronic use of topical ocular medications may induce a clinically identical picture.
d. The most sensitive region of the eye to examine for early findings is the superior tarsus.
163. The classic histologic finding in ocular cicatricial pemphigoid (OCP) is
a. complement and immunoglobulin bound to epithelial basement membrane.
b. intraepithelial immunoglobulin and intraepithelial bullae.
c. granulomatous destruction of epithelial basement membrane.
d. mast cells and eosinophils in the epithelium and subepithelial stroma.
164. Ocular findings consistent with vitamin A defi-ciency include all of the following except
a. keratinization and bacterial superinfection of bulbar conjunctiva.
b. tear deficiency state.
c. deep white lesions of the peripheral retina.
d. focal corneal necrosis with ulceration.
165. Bilateral corneal ulceration should be presumed to be due to vitamin A deficiency until proved otherwise all of the following patients except
a. patients with cystic fibrosis.
b. patients with history of gastric bypass surgery.
c. patients with cirrhosis.
d. patients with normal nutrition and a history of heavy smoking.
166. A 32-year-old woman presents to the ophthalmologist complaining of recurrent pain and tearing of her right eye over the previous 1 to 2 months. Closer questioning discloses that her symptoms are virtually always present upon awakening and disappear after 2 or 3 hours. She denies any history of contact lens use. Which of the following statements is least likely to be true?
a. Careful questioning may reveal a history of corneal abrasion or trauma in the right eye.
b. Careful examination of the right eye may disclose a focal abnormality in tear breakup.
c. Careful examination of the left eye may reveal map or fingerprint abnormalities.
d. This syndrome may be seen more frequently in patients with hypertension.
167. Modalities accepted for treatment of recurrent erosion syndrome include all of the following except
a. pressure patching.
b. 5% sodium chloride ointment at bedtime for 2 to 4 weeks.
c. bandage contact lens.
d. anterior stromal puncture with a 27-gauge needle.
168. Which of the following concerning the mucopolysaccharidoses (MPS) is false?
a. Lysosomal enzyme defects lead to accumulation of metabolites within keratocytes.
b. The MPS least likely to demonstrate corneal clouding is type III (Sanfilippo’s syndrome).
c. Metabolites that accumulate include keratan sulfate, dermatan sulfate, and heparan sulfate.
d. These disorders are all inherited on an auto-somal-recessive basis.
169. The typical corneal finding in a patient with Fabry’s disease is
a. corneal clouding.
b. anterior membrane dystrophy.
c. vortex keratopathy.
d. corneal neovascularization.
170. A 26-year-old woman presents for a routine ophthalmic examination. Slit-lamp examination discloses a vortex keratopathy bilaterally with telangiectatic conjunctival vessels. Her mother and father are both healthy. Which one of the following is false?
a. A careful drug history should be taken.
b. The patient should be warned of potentially lethal renal failure.
c. Fundus findings might include telangiectatic retinal vessels.
d. Half of the patient’s brothers will be seriously affected by the same disorder.
171. A patient presents with photophobia and blurry vision. Examination discloses crystalline deposits throughout the entire stroma, most dense peripherally. Findings important in determining the correct diagnosis include all of the following except
a. family history of eye findings.
b. previous history of kidney transplant.
c. history of peptic ulcer disease (PUD).
d. presence of pigmentary retinopathy in each eye.
172. The corneal findings in tyrosinemia most closely resemble those of
a. anterior membrane dystrophy.
b. herpes simplex keratitis.
c. Wilson’s disease.
d. ochronosis.
173. Which one of the following regarding vortex keratopathy is false?
a. Drugs associated with the finding include amiodarone, indomethacin, chloroquine, and chlorpromazine.
b. The findings in drug-induced vortex keratopathy are identical to those of Fabry’s disease.
c. The drug-induced varieties are accompanied by a pigmentary retinopathy.
d. Cessation of drug therapy will usually lead to resolution of vortex keratopathy.
174. A patient is sent to an ophthalmologist by a gastroenterologist to “rule out Wilson’s disease.” The key part of the ophthalmologist’s examination should be
a. visual acuity measurement.
b. slit-lamp examination.
c. gonioscopy.
d. dilated funduscopy.
175. The most accurate characterization of donor endothelial cell counts following penetrating keratoplasty is
a. no significant change.
b. slow, steady increase in endothelial cell count over 10 to 15 years.
c. rapid loss of endothelial cells over the first postoperative year, slow loss of endothelial cells over the next 10 to 15 years, with stable cell counts after 15 years.
d. slow, progressive loss of endothelial cells over 10 to 15 years with stabilization thereafter.
176. Currently, the most frequent indication for penetrating keratoplasty in the United States is
a. keratoconus.
b. bullous keratopathy following cataract extraction.
c. Fuchs’ dystrophy.
d. herpes simplex keratitis.
177. Which of the following is considered a favorable prognostic factor for penetrating keratoplasty?
a. relatively young age.
b. glaucoma.
c. large graft size (>8.5 mm).
d. no previous history of graft rejection.
178. The primary cause of poor vision following penetrating keratoplasty (PK) for aphakic bullous keratopathy is
a. glaucoma.
b. endophthalmitis.
c. cystoid macular edema.
d. graft rejection.
179. The condition in which same-size or smaller-than-host-bed donor buttons often used is
a. keratoconus.
b. Fuchs’ dystrophy.
c. bullous keratopathy after cataract surgery.
d. corneal stromal dystrophies.
180. Which method of closure of penetrating keratoplasty (PK) causes the greatest amount of irregular astigmatism (prior to suture removal)?
a. interrupted.
b. single running.
c. double running.
d. combined interrupted plus single running.
181. A patient returns for follow-up 8 weeks after penetrating keratoplasty (PK). The central cornea is clear but too irregular to permit accurate keratometry. Vision is 20/400, pinholing to 20/30. What is the most reliable and effective method of visual rehabilitation?
a. random removal of sutures, one per week.
b. removal of sutures that appear tightest at the slit lamp.
c. use of keratoscope to guide suture removal.
d. contact lens refraction and correction.
182. A 62-year-old woman presents complaining of slow loss of vision in each eye. She denies any previous ocular history. Visual acuities are 20/400 in the right eye and 20/100 in the left eye. Slit-lamp examination reveals corneal guttata in both eyes with central stromal thickening more prominent on the right. The corneal epithelium is normal bilaterally. There is dense nuclear sclerosis on the right and moderate nuclear sclerosis on the left. The view of the fundus is consistent with the patient’s vision. The next appropriate step for visual rehabilitation in this patient might be
a. cataract extraction only in the right eye.
b. cataract extraction with posterior chamber intraocular lens (PCIOL) in the right eye.
c. penetrating keratoplasty (PK) alone in the right eye.
d. PK, cataract extraction, and PCIOL in the right eye.
183. Mucous membrane grafting in anticipation of penetrating keratoplasty is most hazardous in patients with
a. Stevens-Johnson syndrome.
b. ocular cicatricial pemphigoid (OCP).
c. trachoma.
d. keratoconjunctivitis sicca.
184. Persistent epithelial defects of the donor cornea following PK are likely to be seen in all of the following except
a. ocular cicatricial pemphigoid (OCP).
b. alkali burns.
c. keratoconus.
d. herpes zoster ophthalmicus.
185. Recurrence of the original disease process has been reported following penetrating kera-toplasty for each of the following conditions except
a. lattice dystrophy.
b. herpes simplex keratitis.
c. Reis-Bückler dystrophy.
d. Fuchs’ dystrophy.
186. The most common postoperative complication seen after penetrating keratoplasty is
a. infectious keratitis.
b. recurrence of the original disease process.
c. high astigmatism.
d. wound leak.
187. A patient presents to the ophthalmologist 12 weeks following penetrating keratoplasty. Complaints consist of increasing redness and discomfort in the operated eye. Visual acuity is the same as the previous office visit 2 weeks earlier. Examination discloses a white, crystalline infiltrate at the donor/host interface between sutures. The infiltrate has indistinct borders, and the stroma appears thickened by it. There is overlying epithelial irregularity but no confluent epithelial defect. Gram’s stain of a corneal scraping reveals gram-positive cocci in chains. Cultures on blood agar grow multiple colonies with alpha hemolysis. Which one of the following statements regarding this condition is false?
a. The causative organism, as with cases originally described, is Streptococcus viridans.
b. This infection is generally slowly progressive.
c. This condition is generally quite responsive to topical antibiotics.
d. Historical factors most significant in the development of the lesion include topical steroid use and keratoplasty.
188. A patient presents the day following penetrating keratoplasty for keratoconus. Examination discloses visual acuity of counting fingers at 1 ft. Slit-lamp examination shows diffuse corneal stromal edema with epithelial irregularity. Intraocular pressure is normal. Which of the following concerning this condition is likely false?
a. By definition this constitutes primary graft failure.
b. The probable cause of this condition is inadequate donor endothelium.
c. A potential cause is inadvertent trauma to the donor button at the time of transplant.
d. It may represent the earliest sign of immunologic graft rejection.
189. Which one of the following regarding corneal allograft rejection is false?
a. Epithelial rejection frequently manifests as subepithelial keratitis identical to EKC.
b. Epithelial rejection is generally more severe and damaging to the donor button than endothelial–stromal rejection.
c. Endothelial–stromal rejection is unlikely to develop in a first graft before 10 to 14 days postoperatively
d. Endothelial–stromal rejection may be incited by suture removal or intraocular laser procedures.
190. Indications for lamellar keratoplasty include all k of the following except
a. Reis-Bückler dystrophy.
b. superficial traumatic corneal scars.
c. lattice dystrophy.
d. Terrien’s marginal degeneration.
191. Which one of the following regarding tissue adhesive closure of corneal defects is false?
a. Polymerization is rapid when the adhesive contacts free anions.
b. The bed to which the adhesive is to be attached must be dry at the time of treatment.
c. Polymerization releases considerable amounts of heat (exothermic).
d. Bandage contact lenses are generally needed following successful adhesive application.
192. Indications for conjunctival flap surgery include all of the following except
a. large perforation in the bed of an infectious corneal ulcer.
b. bullous keratopathy.
c. chronic painful band keratopathy.
d. neurotrophic ulceration.
193. Regarding therapy of herpes simplex stromal keratitis, each of the following is true, except
a. Patients treated with an appropriate regimen of topical steroid will improve more quickly than those without such treatment.
b. Prompt initiation of topical steroids offers no long-term visual advantage in herpes simplex stromal keratitis.
c. Up to one in five patients who are not treated with topical steroid will recover as quickly as patients so treated.
d. Topical trifluridine appears to shorten the duration and lessen the severity of herpes simplex stromal keratitis.
194. Which single-dose oral agent has been shown to be as effective as 7 weeks of topical tetracycline for the treatment of active trachoma?
a. erythromycin.
b. ceftazidime.
c. azithromycin.
e. rifampin.
195. Following incisional keratotomy, radial corneal wounds regain up to what percentage of unin-cised corneal tensile strength?
a. 10%.
b. 25%.
c. 50%.
e. >95%.
196. Which one of the following is not considered a risk factor for the development of bacterial keratitis?
a. topical steroid use.
b. keratoconus.
c. diabetes mellitus.
d. dry eye syndrome.
197. Which one of the following conditions is not seen more commonly in patients with keratoconus?
a. Down’s syndrome.
b. atopic dermatitis.
c. Ehlers-Danlos syndrome.
d. diabetes mellitus, type I.
198. One potential complication of topical ciprofloxacin treatment of infectious corneal ulcers is
a. decreased corneal sensitivity.
b. chronic corneal crystalline deposits.
c. chronic dry eye syndrome.
d. acute dacryocystitis.
199. A 26-year-old female presents with pain, redness, photophobia, and blurred vision in her right eye after sleeping in her soft contact lenses for the past week. Her clinical findings are represented in the photograph shown at the top of next column. Posterior segment examination reveals a quiet vitreous and no retinal pathology. What is the most appropriate next step in management of this patient?
a. penetrating keratoplasty.
b. culture and sensitivity with Gram stain analysis of corneal swab.
c. tap and inject.
d. corneal topography
200. Which of the following is the best initial topical management for the patient shown in question 199?
a. topical moxifloxacin every hour.
b. topical tobramycin/dexamethasone combination every hour.
c. topical fortified antibiotics such as vancomycin with tobramycin every hour.
d. topical chlorhexidine every hour.
 Answers
Answers1. c. This vignette demonstrates a classic case of Acanthamoeba keratitis. Patients often present with pain out of proportion to clinical findings, which is likely secondary to perineural inflammation.
2. c. Acanthamoebae are protozoa found in freshwater and soil and are resistant to killing by levels of chlorine routinely used in municipal water supplies, swimming pools, and hot tubs. Early cases of keratitis have a gray-white superficial, nonsuppurative infiltrate. Acanthamoeba keratitis can present with dendrites and are often misdiagnosed as herpetic keratitis for which topical antiviral and steroid are started.
3. a. As mentioned above, dendrites can be found in some cases of Acanthamoeba keratitis. Early epithelial infiltration can be managed by corneal debridement followed by a short course of anti-amebic therapy. Stromal infection usually occurs in the central cornea. Infection along the distribution of the trigeminal nerve is associated with herpetic infection, not Acanthamoeba.
4. d. Nonnutrient agar with Escherichia coli or Enterobacter aerogenes overlay is the preferred media for culturing amebae.
5. c. Agents used in topical therapy for Acanthamoeba keratitis include diamidines (propamidine, hexamidine), biguanides (poly- hexamethylene biguanide, chlorhexidine), ami-noglycosides (neomycin, paromomycin), and imidazoles/triazoles (miconazole, clotrimazole, ketoconazole, itraconazole). Most of these agents are effective against the free-living trophozoite form of the organism but have reduced efficacy in killing cysts.
6. b. This is essentially the morphologic definition of a conjunctival papilla. Conjunctival papillae form whenever there is conjunctival swelling of any cause in certain areas. The tarsal and limbal conjunctiva are unique because their subepithelial substantia propria contains fibrous tissue septa that interconnect to form polygonal lobules with a central vascular bundle. Any inflammation in these regions will result in papillae. Papillae <1 mm in diameter are entirely nonspecific. When papillae are >1 mm in diameter (giant papillae), they are more specific. Conjunctival follicles represent focal lymphoid aggregates in the substantia propria. These are also more specific than papillae. Chemosis represents subepithelial edema and is nonspecific.
7. c. Most young people with healthy eyes will have small conjunctival papillae along the superior margin of the upper tarsus (on lid eversion, this will be the lower edge of the tarsus).
8. b. The four disorders associated with true giant papillae are vernal and atopic keratoconjunctivitis, and contact lens–related and prosthesis-related GPC. Trachoma has a more pronounced follicular response (although papillae may be seen as a nonspecific sign).
9. d. See answer 10 for explanation.
10. a. Horner-Trantas dots are pathognomic for vernal keratoconjunctivitis. Herbert’s pits are punched-out limbal lesions representing necrotic limbal follicles associated with trachoma. von Arlt’s line is linear subconjunctival scarring seen on the upper tarsus in “burned-out” trachoma. Fuchs’ spots are areas of punched-out chorioretinal atrophy in the maculae of high myopes. Cogan’s patches are focal areas of scleral compaction (dellen) anterior to horizontal rectus insertions in the elderly.
11. d. Itching and discharge may be seen in both contact lens-related GPC and viral conjunctivitis. Likewise, in both cases, the bulbar conjunctiva may be mildly to severely injected. In GPC, the inferior fornix is generally the least involved, whereas in viral conjunctivitis, it tends to be the most severely involved.
12. c. Trachoma is nearly always a disease of the superior conjunctiva. This is in stark contrast to inclusion conjunctivitis, another chlamydial disease, which is more severe inferiorly. Toxic follicular conjunctivitis secondary to medications and viral keratoconjunctivitis are also more severe inferiorly.
13. c. Trachoma is generally insidious. By the time the patient is seen by the ophthalmologist, there is usually a history of red eyes for several months (or of several recurrences). The complications of trachoma are due to scarring and cicatrization of the ocular surface.
14. a. Although the subepithelial keratitis may last for several months, the “red eye” (conjunctivitis) of EKC is nearly always gone after 3 to 4 weeks.
15. c. Neonatal inclusion conjunctivitis may be pseudomembranous or membranous, but this is rare in adults. A pseudomembrane or membrane is a plaque of inflammatory debris—that is, mucus, fibrin, inflammatory cells, and/or hemorrhage— which can be stripped off of a mucosal surface. The distinction between a true membrane and a pseudomembrane is that, when a true membrane is stripped, there is bleeding. This is because a true membrane is fused with and incorporated into the mucosal epithelium. Clinically, pseudomembranes and true membranes have similar appearances with a nearly identical differential diagnosis.
16. d. This is a feature that may help in differentiating between the two type I hypersensitivity causes of GPC. Atopic keratoconjunctivitis rarely comes with a (pseudo)membrane, whereas vernal keratoconjunctivitis may.
17. c. The depositions that form the horizontal band across the exposed portions of the cornea generally start peripherally and proceed centrally, but this is not invariable. The material that forms the deposit is most often calcium salts but also may be composed of urate salts.
18. b. Note that “granulomatous” KPs may have a characteristic greasy, mutton fat appearance without actually being granulomas themselves. Epithelioid histiocytes are responsible for the clinical appearance.
19. c. Endophthalmitis and corneal perforation rates are higher with LASIK than with PRK. LASIK does offer a reduced incidence of stromal haze and more rapid epithelial healing. PRK can have significant postoperative pain.
20. a. On Gram’s stain, mycobacteria may resemble corynebacteria—small pleomorphic grampositive rods resembling Chinese characters. Acid-fast (Ziehl-Neelsen) staining will highlight the mycobacteria, not diphtheroids.
21. d. Therapy of ocular mycosis is heavily dependent on geographic locale.
22. b. Think “Candida in Canada” and “Fusarium in Florida.
23. c. Fungi may be classified into three groups: (a) molds, or filamentous fungi (e.g., Fusarium, Penicillium); (b) yeasts (e.g., Candida); and (c) dimorphs (may exist as either mold or yeast, depending on environment).
24. c. Cryptococcal keratitis is distinctly uncommon.
25. b. Fungi are typically hearty.
26. d. There are five anti-EBV antibodies: (a) VCA-IgG, (b) VCA-IgM, (c) EA-D, (d) EA-R (early antigen–restricted), and (e) EBNA. Only EBNA does not peak in the first 6 to 8 weeks of infection. VCA-IgG and EBNA provide lifelong evidence of EBV infection.
27. d. The rates of corneal haze are similar to LASIK. All of the other answers are true. PRK with the concomitant use of mitomycin C also appears to reduce the incidence of postoperative corneal haze.
28. d. Like bacteria (and unlike viruses), chlamydiae have both DNA and RNA, replicate via binary fission, have lipopolysaccharide cell walls, and respond to certain antibiotics. Unlike bacteria, chlamydiae do not possess all organelles and require a host cell for replication.
29. a. More than 50% of flap folds occur within the first day, and more than 90% of flap folds occur within the first week postoperatively. Not all folds need to be repaired, but visually significant folds should be repaired within 24 hours.
30. a. Only Phthirus pubis (crab) has been associated with lash infestation. Pediculus capitis (head louse) resides only in the scalp. Therefore, ocular “pediculosis” is a misnomer (the better term is “phthiriasis”).
31. a. This is useful for suspected chlamydial disease.
32. d. Topical acyclovir is available in Europe for HSV keratitis.
33. c. Radial incisions have a greater effect as they move closer to the visual axis. These incisions can sometimes be used to correct postoperative astigmatism.
34. b. The hypersensitivity reaction to idoxuridine is so strong that it may induce lymphadenopathy.
35. d. Topical natamycin is the drug of choice for presumed filamentous keratomycosis.
36. a. Clotrimazole is the drug of choice for Aspergillus keratitis.
37. c. Polyenes are insoluble in water and have systemic toxicity via binding to renal tubular cells and erythrocytes.
38. b. Liver enzymes should be monitored during long-term ketoconazole therapy.
39. c. PMNs release hydrolytic enzymes that denature protein and cause tissue necrosis.
40. c. Intracorneal rings are currently being used for the treatment of low myopia. They are also being studied as a potential treatment for keratoconus. Corneal perforation is a potential complication of the procedure, but occurs less frequently than decreased corneal sensation.
41. c. Although drug levels in the cornea do not necessarily correlate with antiinflammatory activity, studies involving rabbit corneas indicate that prednisolone acetate has the greatest antiinflammatory activity.
42. a. An anaphylactoid reaction is rapid in onset with itching, conjunctival erythema, and chemo-sis and is usually caused by penicillin, bacitracin, sulfacetamide, or anesthetics.
43. d. Allergic contact reactions (type IV) are slow and gradual in onset and characterized by itching with eczematoid dermatitis and conjunctival injection.
44. d. The most common cause of phlyctenulosis is Staphylococcus, followed by active or latent tuberculosis.
45. d. It is important to recognize and treat hyperacute purulent conjunctivitis; untreated, it can rapidly progress to corneal ulceration and perforation.
46. d. This is the only bacterial conjunctivitis that routinely causes preauricular adenopathy.
47. a. Doxycycline (or tetracycline) is added to treat potential chlamydial infection (sexually transmitted diseases tend to run together).
48. c. Removal of the lesions is curative.
49. d. Pharyngoconjunctival fever is typically caused by adenovirus types 3 and 7.
50. a. Adenoviral conjunctivitis is highly contagious, and infection can be transferred by fomites several weeks after onset. Epidemic keratoconjunctivitis may produce a hemorrhagic or membranous conjunctivitis.
51. d. Personal contacts must be examined and treated because of the venereal nature of the disease.
52. a. The follicular response of inclusion conjunctivitis is rarely seen in the neonatal form. Although neonatal inclusion conjunctivitis usually responds to topical therapy, systemic erythromycin is recommended because of associated chlamydial infections, such as otitis media and pneumonitis.
53. a. Seasonal allergic conjunctivitis is ideally treated with topical antihistamines.
54. c. Topical antihistamines do not work well in atopic keratoconjunctivitis; systemic antihista-mines are critical for its control.
55. d. Although conjunctival scraping in atopic disease usually reveals fewer eosinophils than in vernal keratoconjunctivitis, their mere presence is not a useful differentiating factor.
56. d. By definition, atopic keratoconjunctivitis is an IgE-mediated process that occurs in patients who have atopic dermatitis (eczema).
57. c. This history is classic for the floppy eyelid syndrome. Spontaneous eyelid eversion occurs during sleep with minimal pillow (or bedsheet) contact. The condition is treated by mechanically protecting the involved eye (taping, shield). If these conservative measures fail, horizontal lid tightening procedures may be attempted.
58. c. Trachoma is the most common cause of irreversible blindness in the world, but not in the United States.
59. b. Type 2 herpes usually resides latently in spinal ganglia. The gasserian (or trigeminal) ganglion, located in Meckel’s cave, contains the cell bodies of the trigeminal nerve.
60. d. Vesicular blepharitis may occur in either primary or recurrent HSV infection. Dendrites are fleeting in primary infection. Lymphadenopathy is rare in secondary disease.
61. d. Overtreatment with topical antivirals is common and should be avoided. Bacterial superinfection is not a complication of overtreatment.
62. a. This ulcer is typical of a “metaherpetic” lesion and does not reflect epitheliitis. Corneal epithelial healing is impaired by decreased sensation, stromal inflammation, and antiviral toxicity.
63. b. Peripheral anterior synechiae occur commonly following anterior uveitis due to HSV but are not usually seen with disciform keratitis.
64. a. The phenomenon is identical to the immunoprecipitate formed in the Ouchterlony gel.
65. a. Herpes zoster “dendrites” (pseudodendrites) are typically smaller and less branching than their simplex counterparts.
66. d. Drug abuse, particularly crack cocaine smoking, is associated with contamination and damage of corneal epithelium. Diabetes mellitus is associated with defective epithelial adherence, as is aging (which also comes with relative hypesthesia).
67. b. Fortunately, herpetic keratitis does not appear to increase the risk of subsequent fungal keratitis.
68. b. Leprosy is a cause of IK worldwide, but is uncommon in the United States.
69. a. Patients are also at risk of aortitis with dissecting aneurysms.
70. b. The conjunctiva is usually normal in Thygeson’s disease.
71. b. About one-half of patients with SLK have some form of thyroid disease. Treatment of the thyroid disorder, however, has little effect on the SLK. A recent study suggests that orbital decompression for thyroid optic neuropathy is required more frequently in patients with thyroid-associated SLK.
72. d. Alkali injury has the potential to cause the most long-term damage as these agents have the potential to significantly penetrate ocular tissue. Alkaline substances saponify cell membranes. For any chemical burn, the ocular surface must be irrigated until pH is normal (6.8 to 7.2). Corneal epithelial loss, clarity, and limbal ischemia (whitening) are critical early prognostic factors.
73. c. Retained foreign bodies represent a hazardous depot of alkaline material. These must be removed immediately upon detection.
74. d. Epithelial continuity is essential for the prevention of infections, inflammation, and scarring. Unfortunately, severe chemical injuries retard healing. Avoiding drugs that are toxic to the epithelium (e.g., neomycin, tobramycin, gentamicin) is very important, as these agents will inhibit corneal epithelial healing. If corticosteroids are to be used, they should be restricted to the first 5 to 10 days. They are useful in reducing corneal and intraocular inflammation and helpful in combating the formation of symblepharon. However, corticosteroids may enhance collagenase-induced corneal melting, which often begins 1 to 2 weeks after the injury.
75. d. Episcleritis is a recurrent, transient, self-limited, and usually nonspecific disease of young adults. Simple episcleritis is sectoral in 70% and generalized in 30% of cases. Pingueculae may show a distinct form of episcleritis with local superficial inflammation similar to nodular episcleritis. Episcleritis rarely progresses to scleritis; however, episcleritis nearly always accompanies scleritis. Two-thirds of patients with episcleritis have recurrences, and the condition is usually self-limited without treatment. The condition can be treated with topical steroids and/or oral nonsteroidal agents.
76. a. Diffuse anterior scleritis is the most benign form of scleritis and is associated with the least severe systemic conditions.
77. c. Necrotizing scleritis with inflammation is the most destructive form of scleritis. Sixty percent of affected patients develop complications (in addition to scleral thinning), and 40% suffer visual loss. These patients are at risk for mortality, secondary to associated autoimmune disease.
78. d. Patients with scleromalacia perforans (necrotizing scleritis without signs of inflammation) often have long-standing rheumatoid arthritis.
79. a. Scleritis can occur in association with various systemic infectious diseases, including leprosy, tuberculosis, herpes zoster, and syphilis. Metabolic diseases such as gout also may be associated with scleritis. Approximately one-half of patients with scleritis have an associated systemic disease. Scleritis is frequently associated with autoimmune connective tissue diseases such as systemic lupus erythematosus, rheumatoid arthritis, polyarteritis nodosa, or Wegener’s granulomatosis. Inflammatory bowel disease also has been reported in conjunction with peripheral ulcerative keratitis.
80. c. Subtenon’s injections of corticosteroids are relatively contraindicated in patients with auto-inflammatory sclerokeratitis because these drugs may result in scleral thinning and increased potential for perforation.
81. c. Acute dacryoadenitis is most often caused by ascending staphylococcal infection, often in patients who suffer from dehydration, and is associated with a purulent conjunctival discharge. Viral dacryoadenitis is frequently painless.
82. a. Chronic dacryoadenitis is usually associated with systemic disease such as lymphoma, sarcoidosis, syphilis, or tuberculosis. Sarcoidosis is the most common cause of painless bilateral enlargement of the lacrimal gland.
83. b. Chronic dacryoadenitis is sometimes accompanied by inflammation and swelling of the salivary glands, which is referred to as Mikulicz’s syndrome. Biopsy may be required for diagnosis.
84. c. Actinomyces israelii is usually found with expression or curettage of the canaliculus.
A. israelii is a gram-positive, branching, filamentous bacterium. Canaliculitis occurs more frequently in females.
85. d. A lacrimal sac abscess has formed and is not responsive to oral antibiotics. It should be drained.
86. a. Congenital obstruction of the nasolacrimal system usually produces epiphora. The lumen of the nasolacrimal duct is blocked near the lower ostium (valve of Hasner) by epithelial debris or a mucosal membrane. The ostium will open spontaneously in 90% during the first 9 months of life. Gentle probing and irrigation of the nasolacrimal system are performed by 6 to 9 months of age, if the system does not open spontaneously. If probing is unsuccessful, silicone tube intubation should be considered.
87. b. Because of the patient’s age, probing and irrigation should be performed; few blocked ducts will open spontaneously after 12 months of age.
88. d. Eyes without any astigmatism will not have any wavefront aberration. Wavefront analysis is used to analyze irregular astigmatism. An eightleaf clover will be produced with a PKP using eight interrupted sutures (and a four-leaf clover will be produced using four interrupted sutures). Spherical aberration occurs when peripheral rays focus in front of central rays, leading to night myopia in postoperative LASIK patients.
89. d. Lamellar keratoplasty does not effectively treat conditions with damaged corneal endothelium.
90. a. Munnerlyn’s formula estimates the ablation depth needed centrally to perform photore-fractive keratectomy. It is most useful with low amounts of correction (<7 D). Note that the amount of ablation needed is directly proportional to the square of the optical zone, so a larger optical zone requires more ablation.
91. d. These benign tumors demonstrate hyperkeratosis, parakeratosis, and epidermidalization, in addition to lobular acanthosis surrounding vascular cores. Papillomas of the eyelid in young people are often caused by the human papillomavirus.
92. c. Keratoacanthoma is a reactive tumor that develops rapidly over 4 to 8 weeks. It is a large, elevated, and round cutaneous tumor that contains a central core of keratin. Although acanthosis, hyperkeratosis, and dyskeratosis may be extreme, dysplasia is often absent. Inflammation is prominent because keratoacanthoma is a type of pseudoepitheliomatous hyperplasia. Keratoacanthoma is likely a low-grade squamous cell carcinoma. The other lesions listed in the question are primarily disorders of the elderly.
93. c. Seborrheic keratoses are usually verrucoid and “greasy” looking.
94. d. This is an example of basal cell carcinoma, a slowly growing tumor of the skin. Conjunctival involvement is rare, and lesions are most commonly found on the lower lid.
95. a. The fibrotic type is also known as morpheaform. This pattern features strands of tumor cells infiltrating out from the central, clinically apparent lesion. Thus, it is much more difficult to define the margins of the lesion. They are also less responsive to radiation therapy. The other forms listed tend to be more localized.
96. d. Tumors here tend to be more deeply invasive, and the involved structures are more difficult to free of tumor.
97. b. Distant metastases of any kind are very rare for this tumor. Its invasive, burrowing nature is reflected in its historical pseudonym, “rodent ulcer.”
98. a. These lesions tend to be slow growing.
99. a. The histopathology indicates a sebaceous cell carcinoma of the eyelid, a disorder of later life. Only prompt recognition of the diagnostic possibility with prompt resection offers hope for complete cure. All too often, chalazia are repeatedly drained, with no pathologic review to exclude this critical diagnosis. Because of this tumor’s tendency to produce “skip” lesions (discontinuous areas of diseased tissue), Mohs’ techniques may leave residual tumor behind. Map biopsies are generally necessary. Potential sites of origin of sebaceous cell carcinoma are glands of Zeis, glands of the caruncle, and meibomian glands: all sebaceous type glands. Moll’s glands are apocrine sweat glands.
100. d. Frozen section techniques allow for preservation of tissue lipid, staining for which (oil-red O stain) plays a role in diagnosing sebaceous cell carcinoma.
101. a. The syringoma is derived from sweat gland tissue.
102. d. An alternate name for pilomatrixoma is the “calcifying epithelioma of Malherbe.”
103. b. The opposite is true. They tend to move deeper into the subepithelial space, migrating into the dermis (or conjunctival substantia propria).
104. d. Radiation therapy is a very important and effective modality for treating these lesions.
105. c. Xanthelasma tend to be flat, plaquelike lesions, as opposed to nodules.
106. d. Oral mucosal leukoplakic lesions are the other common finding in benign hereditary intraepithelial dyskeratosis—an obscure, dominantly inherited condition found in a paucity of North Carolinians.
107. c. The grading of epithelial dysplasia is identical, as is the acronym (CIN: conjunctival, cor-neal, or cervical intraepithelial neoplasia).
108. b. Clear lens exchange is the same procedure as phacoemulsification with posterior chamber lens implantation. However, patients with high myopia are already at risk for retinal detachment, and intraocular surgery can increase this risk further. Also, if posterior capsular opacification develops, an Nd:YAG capsulotomy will also increase the risk of retinal detachment. Ptosis is also a risk of cataract surgery. Flap dehiscence does not occur with clear lens exchange, because unlike LASIK, there is no stromal flap created.
109. c. The same is true for conjunctival neoplasms.
110. b. By definition, the neoplasia of the corneal epithelium is not invasive until it has begun to penetrate Bowman’s layer.
111. a. Although the conjunctiva does not have a dermal layer, subepithelial conjunctival nevi occur and are equivalent to dermal nevi of the skin. The nevus cells, with time, migrate down into the substantia propria.
112. d. Ocular melanocytosis is a congenital blue nevus of the episclera and is most common in Caucasians. When ocular melanocytosis occurs in combination with periocular cutaneous mela-nosis (nevus of Ota), it is termed oculodermal melanocytosis. This is more common in African Americans and Asians and is nearly always unilateral. Malignant transformation is rare, but it seems to occur almost exclusively in Caucasians.
113. d. Primary acquired melanosis is most frequently found on the bulbar conjunctiva or in the fornices. Nodular thickening is an indication for excisional biopsy.
114. c. Although the anterior segment dysgenesis anomalies were once felt to be a result of meso-dermal dysgenesis, it is now believed that the affected tissues are of neural crest origin.
115. a. Posterior embryotoxon is a centrally displaced Schwalbe’s line that is visible without gonioscopy.
116. b. Axenfeld-Rieger syndrome is a spectrum of anterior segment defects characterized by an anteriorly displaced Schwalbe’s line. Patients may have glaucoma, developmental defects of facial bones and teeth. It is most commonly inherited in an autosomal dominant pattern. In the past, “Rieger’s anomaly” was defined as the components of “Axenfeld’s anomaly” plus atrophy of the iris stroma. “Rieger’s syndrome” was defined as “Rieger’s anomaly” with additional findings of skeletal, dental, or craniofacial abnormalities. However, the term Axenfeld-Rieger syndrome is now more appropriate given the high incidence of overlapping findings, rather than rigidly defining each syndrome/anomaly.
117. a. An anterior cataract or dislocated lens may be present but is not necessary for the diagnosis. Peters anomaly is bilateral in two-thirds of cases.
118. b. Congenital glaucoma can be distinguished from birth trauma by the presence of increased intraocular pressure and horizontal (as opposed to vertical) breaks in Descemet’s membrane. In corneal birth trauma, residual hypertrophic ridges in Descemet’s membrane are often visible even after the corneal edema clears.
119. b. The actinic damage seen in pingueculae results in changes in the subepithelial collagen. Although these fibers stain with some elastin stains, the fibers are not true elastin and will not be degraded by elastase. This finding is known as “elastosis.”
120. a. Pterygia invade the cornea down to Bowman’s layer, producing fibrovascular ingrowth at this layer. Because excised pterygia can recur with vigor, surgery is indicated only when the visual axis has been obscured or if there is extreme irritation. Pterygia are assicated with iron lines, often referred to as Stocker’s lines.
121. d. Mitomycin C, beta-irradiation with strontium 90, and conjunctival autotransplantation all have been shown to reduce the recurrence rate of pterygia.
122. b. Amyloid exhibits dichroism and birefringence when stained with Congo red.
123. d. Note that only one polarizing filter is required to elicit dichroism.
124. a. Primary localized amyloidosis consists of conjunctival amyloid plaques, which occur without systemic involvement and without a local cause.
125. b. Primary systemic amyloidosis produces ecchymotic, waxy eyelid papules. Other ocular structures also may be infiltrated, including vitreous and uveal tract.
126. a. The white limbal girdle of Vogt consists of white flecklike deposits at the nasal and temporal limbus. It consists of subepithelial elastotic degeneration and is sometimes accompanied by calcium deposition. Meretoja’s syndrome is a form of systemic amyloidosis combined with corneal lattice dystrophy.
127. a. The lipid deposition in arcus senilis tends to occur at the superior and inferior poles (where the local temperature is highest) and then spreads into the palpebral fissure. In the setting of high-grade carotid stenosis, the ipsilateral eye is protected from lipid deposition. There is an increased incidence of arcus in African Americans.
128. c. Cornea farinata is a condition that is characterized by asymptomatic tiny deep stromal opacities that are best viewed by retroillumination. Corneal guttae are at the level of the corneal endothelium. Hassall-Henle bodies are normal aging changes found in the peripheral cornea.
129. d. Band keratopathy starts at the horizontal periphery. It may spread centrally to form a horizontal band. Occasionally, it starts paracentrally. It is always in Bowman’s layer.
130. c. The urate form is much less common and may be associated with gout or hyperuricemia.
131. d. Salzmann’s nodular degeneration, spheroidal degeneration, and Coats’ white ring are corneal degenerations that typically do not involve neovascularization. (However, if located peripherally, each of the three may have surface neovascularization.)
132. b. The variety of Mooren’s ulcer that occurs in young men of African anscestry is usually more aggressive and responds poorly to medical or surgical management. Perforation is more common in this group. It is felt that some patients in this group may have developed the corneal ulceration as a result of antigen–antibody reactions to helminthic toxins. The toxins may get deposited during the blood-borne phase of certain parasitic infections.
133. b. Both congenital and acquired (degenerative) forms of map-dot-fingerprint dystrophy may be seen. The latter may develop in the setting of recurrent erosions associated with trauma, contact lens use, or chronic blepharoconjunctivitis. Reis-Bückler dystrophy involves Bowman’s zone, whereas lattice and central cloudy dystrophies are stromal dystrophies.
134. c. Dots seen in anterior membrane dystrophy are clumps of degenerated epithelial cells and basement membrane material within the epithelium. They are also known as microcysts. Cogan’s microcystic edema is the eponym for the pure “dot” form of this disorder.
135. d. Successful treatment is generally targeted toward stimulating production of new, healthier basement membrane material via epithelial removal or stimulation (debridement or puncture), occlusion therapy (patching, contact lenses, lubrication), and/or epithelial dehydration (for recurrent erosions).
136. b. Epithelial cysts are seen in both map-dot-fingerprint and Meesman dystrophies. The cysts in the former are translucent or opaque and represent degenerated epithelial cells and basement membrane. Those of Meesman dystrophy are transparent and are filled with PAS-positive material known as “peculiar substance.” Fibrocellular invasion of Bowman’s zone (pannus) is typical of Reis-Bückler dystrophy; hyaline stromal deposits are seen in granular dystrophy. Congophilic stromal deposits are the hallmark of lattice dystrophies.
137. b. Recurrent erosions and anterior corneal scarring lead to visual loss in Reis-Bückler dystrophy sooner and to a greater degree than in the others. Pre-Descemet’s dystrophy is usually clinically silent, like central cloudy dystrophy.
138. c. In granular dystrophy, recurrent erosions are seen, but much less commonly than for the anterior dystrophies or lattice dystrophy. Transmission is autosomal dominant. Visual acuity is generally affected, but not until later in life (fifth decade or later). Stromal deposits of hyaline are diagnostic and may be associated with amyloid deposits in certain subtypes (Avellino variant).
139. b. Macular dystrophy may have focal stromal deposits but differs from granular dystrophy in several ways. First, the intervening stroma is cloudy. Second, the peripheral cornea is involved much earlier in macular dystrophy. Third, macular dystrophy is inherited recessively, so that parents or offspring are unlikely to be involved, whereas siblings are likely to be involved. Patients with macular dystrophy have a deficiency in enzymatic synthesis of keratan sulfate, and serum levels are typically depressed. The mnemonic for stromal dystrophies (dystrophy, deposit, stain) is Marilyn Monroe Always Gets Her Man in Los Angeles County. Marilyn Monroe Always (Macular/Mucopolysaccharide/ Alcian blue) Gets Her Man (Granular/Hyaline/ Masson trichrome) in Los Angeles County (Lattice/Amyloid/Congo red).
140. c. Lattice dystrophy also may have granular deposits but also features linear, branching (lattice) deposits. Both types of deposits are amyloid and will demonstrate birefringence and dichroism when stained with Congo red. In type I, as in this patient, the deposits are randomly distributed, greater centrally. This form is localized. In type II, the deposits are along the course of the corneal nerves, so they are denser peripherally. Type II is seen only in familial amyloidotic polyneuropathy type IV (Meretoja’s syndrome) and is associated with cranial nerve palsies and dry, redundant skin. Like granular dystrophy, lattice dystrophies are inherited dominantly. This is the stromal dystrophy most likely to be associated with recurrent erosions.
141. b. Central crystalline dystrophy of Schnyder represents intrastromal accumulation of cholesterol crystals. Like xanthelasma and corneal arcus, a minority of patients have systemic hyperlipidemia.
142. c. This disorder may be highly asymmetric or unilateral and associated with a wide range of ocular or systemic disorders. Tiny flecks are visible in corneal stroma. Vision is not affected.
143. d. Central cloudy dystrophy is nearly always clinically silent.
144. b. Symptoms of Fuchs’ dystrophy are typically worse in the morning, when the corneal epithelium is more hydrated. Mild corneal stro-mal edema may be silent in the setting of visually significant cataract, so that triple procedures (penetrating keratoplasty, cataract extraction, intraocular lens placement) may be indicated despite asymptomatic corneal changes (with preexistent corneal edema, further decompensation is almost certain). If there are no signs (as opposed to symptoms) of corneal decompensation (stromal or epithelial edema), then cataract extraction and intraocular lens implantation may be undertaken alone.
145. a. In the setting of normal corneal diameters, glaucoma is less likely. Congenital hereditary endothelial dystrophy presents like congenital glaucoma, except the corneal diameters and IOP are normal. In congenital hereditary stromal dystrophy, the clinical appearance is similar, except the stroma has normal thickness (but diffusely hazy), and the epithelium is spared. This disorder reflects an abnormality in neural crest cell migration or differentiation.
146. b. This bilateral disorder presenting in a young man is less likely to be ICE than posterior polymorphous dystrophy (PPMD). Transmission is autosomal dominant, but expression is highly variable and asymmetric. Clinical findings may be similar to those of ICE. Histopathologically, the disorder may simulate epithelial downgrowth, but the cell of origin is the corneal endothelial cell.
147. d. The earliest stage of keratoconus is progressive myopia with high astigmatism. Exactly when an eye may be declared to have keratoconus is a matter of opinion.
148. b. Corneal thinning, myopia, and astigmatism are most likely to progress significantly during adolescence, although progression can occur at any time.
149. a. Acute hydrops reflects sudden stromal edema associated with an acute break in Descemet’s membrane. Pain may be severe, but frequently the only symptom is blurry vision. Once the break in Descemet’s membrane spontaneously seals (in 6–10 weeks), the stromal edema clears. Residual scarring may or may not require penetrating keratoplasty.
150. c. Rigid gas permeable (RGP) contact lenses are the optical correction of choice in keratoconus because these lenses are the most successful at eradicating irregular astigmatism.
151. c. Higher corneal protrusion above the area of corneal thinning makes fitting very difficult in pellucid degeneration. Scleral contact lenses have been tried with some success.
152. c. Diffuse lamellar keratitis, also known as “Sands of the Sahara,” typically manifests itself within the first week after LASIK surgery. If it is diagnosed early, topical steroid treatment usually provides for an excellent prognosis. However, later stages (clumping of white blood cells in the central visual axis) usually require flap lifting, irrigation, intense topical steroids, and occasionally systemic steroids.
153. b. Typically, tear volume is deficient in dry eye syndrome (inadequate aqueous phase), but an important subset of patients have problems with surface wetting due to deficiencies of the other phases (mucus problems in keratinizing disorders, lipid problems in blepharitis). Schirmer’s testing in these cases may be normal or supranormal despite a history and examination suggestive of dry eye. Tear breakup time is frequently the important clue.
154. a. Schirmer’s testing in these cases may be normal or supranormal despite a history and examination suggestive of dry eye. Tear breakup time is frequently the important clue.
155. b. The most frequent association is classic rheumatoid arthritis.
156. d. A variety of autoimmune diseases have been reported to develop following chronic primary Sjögren’s syndrome. There is no known association with epithelial lacrimal gland neoplasms.
157. c. Punctal occlusion is safe and effective therapy for severe dry eye syndrome. Epiphora is the most likely adverse effect, so a graded, stepwise approach is generally taken. Temporary occlusion of inferior puncta allows assessment of response prior to permanent occlusion.
158. c. The combination of corneal hypesthesia and exposure/lagophthalmos is nearly always disastrous for the corneal surface. Lateral tarsorrhaphy is advisable before irreversible, destructive changes can commence.
159. b. Comedones are not a feature of rosacea dermatitis. This differentiates acne rosacea from acne vulgaris. Demodex folliculorum may play an adjuvant role in what is primarily a type IV hypersensitivity reaction to unknown stimuli.
160. b. Potent steroids may precipitate melting in eyes with rosacea keratitis. Any steroid preparation should probably be avoided in the setting of frank corneal ulceration. Once epithelial continuity has been restored and secondary infection adequately treated (hygiene, antibiotic ointments, oral tetracycline), mild steroid preparations are probably safe but must be used with adequate surveillance.
161. b. Oral and conjunctival epithelia are the most frequently involved, with a slight preponderance of the latter.
162. d. The inferior fornix is generally the most rewarding area of the eye to examine in OCP. Here, subepithelial fibrosis and fornix foreshortening may be seen to precede symblepharon formation. The superior tarsus may show subconjunctival scarring. For treatment, dapsone is an acceptable first choice in mild to moderate cases in patients with no evidence of glucose-6-phosphate dehydrogenase deficiency (in whom dapsone can cause a fatal hemolytic anemia). The most reliable prognostic indicator for long-term outcome in OCP is the severity and rapidity of active inflammation. Thus, severe cases should be treated with more potent immunosuppressive agents from the outset, such as cyclophosphamide.
163. a. This is in distinction to pemphigus, in which epithelial acantholysis and intraepithelial bullae are characteristic features.
164. d. Areas of metaplastic keratinization of the conjunctiva within the exposure zone are known as Bitot’s spots. Secondary infection by xerosis bacilli (Corynebacterium xerosis) is common. A peripheral retinopathy of minimal functional significance also has been described. Keratomalacia, diffuse corneal necrosis and melting, is the most disastrous of manifestations.
165. d. Any deficiency of fat absorption may lead to hypovitaminosis A. Chronic alcoholics with very poor nutrition should be suspected of relative hypovitaminosis A and undergo serum vitamin A level testing in the setting of bilateral dry eye or corneal ulceration.
166. d. The history is most compatible with recurrent erosion syndrome. Predisposing factors are numerous and include previous corneal abrasion, particularly recalcitrant ones; contact lens use; anterior corneal dystrophies (map-dot-fingerprint, Reis-Bückler); and diabetes mellitus (defective basal epithelial adherence).
167. b. Hypertonic saline may be useful in maintaining epithelial deturgescence and enhancing adherence but must be used for several (4–6) months if it is to have long-term effect.
168. d. Type III (Sanfilippo’s syndrome) is virtually never associated with corneal clouding. Type II (Hunter’s syndrome) is rarely associated with corneal clouding (only adults with the milder variety). Type II is inherited on an X-linked– recessive basis.
169. c. The findings are indistinguishable from medication-induced vortex keratopathy.
170. b. Fabry’s disease is an X-linked recessive disorder featuring accumulation of cerebrosides in the cardiovascular system and kidneys. Affected male patients develop renal failure, but female carriers do not.
171. c. Three forms of cystinosis are recognized. The infantile form is the most severe, followed by the juvenile or adolescent form. Renal failure is expected in both. The adult form is mild (renal failure is unusual). Monoclonal gammopathies may be associated with corneal crystals, with immunoglobulin deposits in the peripheral cornea. PUD is not associated with cystinosis or myeloma. Bietti’s crystalline dystrophy features crystalline keratopathy and a pigmentary retinopathy.
172. b. In tyrosinemia, elevated serum tyrosine levels lead to lysosomal instability with dermal and ocular inflammation, as well as mental retardation. Nonstaining pseudodendrites may recur and be misdiagnosed as HSV.
173. c. Of the agents known to cause vortex keratopathy, only chlorpromazine is associated with pigmentary retinopathy. The two are generally independent. (Chloroquine can cause a bull’seye maculopathy as well.)
174. c. The earliest sign of copper deposition in Descemet’s membrane (Kayser-Fleischer ring) is detectable only at the far periphery with gonioscopy. Slit-lamp examination alone is insufficient.
175. c. After corneal transplant, there is often rapid loss of endothelial cells over the first postoperative year, slow loss of endothelial cells over the next 10 to 15 years, with stable cell counts after 15 years.
176. b. Bullous keratopathy following cataract extraction is the most frequent indication for corneal transplant.
177. d. Other favorable factors include lack of neovascularization, lack of inflammation, and no history of previous graft failure. Unfavorable factors include stromal vascularization, tear defi-ciency state, corneal hypesthesia, youth, larger grafts, and glaucoma.
178. c. Most IOLs capable of causing corneal decompensation also can cause chronic intraocular inflammation and secondary cystoid macular edema.
179. a. Smaller-than-host donor buttons tend to be flatter and thus more hyperopic than the larger-than-host buttons. This effect helps to neutralize part of the high myopia seen in eyes with keratoconus.
180. a. Interrupted sutures, without a running suture, induce the greatest amount of irregular astigmatism.
181. c. Keratoscopy gives qualitative information regarding corneal topography when the surface is too irregular to permit quantification with keratometry.
182. d. In the setting of corneal edema and cataract, the triple procedure is probably advisable. Guttae alone are not a sufficient indication for this procedure. There should be stromal or epithelial edema before it is undertaken.
183. b. Ocular surgery may precipitate increased disease activity in OCP. Once the other disorders have become quiescent, they typically remain so.
184. c. Preexistent epithelial and/or surface disorders predispose the graft to chronic epithelial defects. Keratoconus has an excellent prognosis after PK.
185. d. Unless the donor endothelium is unhealthy or damaged at the time of transplantation (primary graft failure), the findings of Fuchs’ dystrophy do not recur. Primary failure is different than true recurrence, which has been reported numerous times for each of the other disorders.
186. c. This complication can frequently be controlled with selective suture removal, but in some cases refractive surgery is necessary.
187. c. Frequently, prolonged topical and systemic antibiotic therapy is necessary, with or without surgical therapy (lamellar or penetrating excision). This infectious crystalline keratopathy (IKC) is closely associated with keratoplasty and topical steroid use.
188. d. Immunologic graft failure never presents within 24 hours of transplantation.
189. b. Epithelial rejection is typically mild and of no long-term significance because host epithelium quickly populates the donor surface. Endothelial rejection is of far greater visual significance and may be precipitated by seemingly innocuous events, all of which stimulate ocular inflammation. Endothelial graft rejection should be treated as an emergency with intensive topical and systemic steroids.
190. c. Lattice dystrophy typically involves the deeper stroma, so lamellar surgery is not definitive.
191. c. The absence of significant heat release makes adhesives safer and more reliable.
192. a. A conjunctival flap will not provide an adequate seal over an underlying fistula or perforation. The “hole” must be closed with a tectonic graft (full-thickness or lamellar, with sclera or cornea) before a flap may be advanced.
193. d. The Herpetic Eye Disease Study has answered several questions regarding the utility of topical steroids in herpes simplex stromal keratitis. Topical steroids reduced persistence or progression of stromal keratitis compared with placebo. Delayed initiation of steroid therapy slowed resolution but did not affect long-term (6 months) visual outcome. Recurrences following steroid taper responded well to a more gradual taper. Topical trifluridine was used in both treatment arms of the study to help lower the incidence of epithelial keratitis. A large proportion of patients treated with trifluridine and placebo suffered significant progression of herpetic inflammation, implying that trifluridine alone does not exert a significant beneficial effect for stromal keratitis.
194. c. Azithromycin and clarithromycin are among the class of bacterial ribosomal inhibitors known as azalides. They are related chemically to erythromycin but are much more rapidly distributed to tissues with better absorption, bioavailability, and higher intracellular penetration. Azithromycin’s tissue half-life is also quite long, 2 to 4 days, rendering it useful as a singledose agent. This enhances compliance relative to the traditional prolonged topical treatment and also offers the advantage of treating extraocular reservoirs of chlamydia.
195. c. Following incisional keratotomy, radial corneal wounds regain up to 50% of unincised corneal tensile strength.
196. b. Keratoconus is not considered a risk factor for the development of bacterial keratitis.
197. d. Diabetes is not associated with keratoconus.
198. b. These are probably due to precipitation of drug, which requires low pH for solubility. Ofloxacin may not be subject to this complication.
199. b. This patient has contact lens associated bacterial keratitis. In order to better direct antibiotic therapy, appropriate laboratory analysis should be performed including gram staining, culture, and sensitivity of the organism. PK is indicated if there is significant corneal perforation. Vitreous tap and inject is utilized if endophthalmitis is suspected (unlikely if there is no vitreous cell). This patient’s cultures demonstrated Pseudomonas resistant to beta-lactams.
200. c. With a large, purulent ulcer, topical fortified antibiotics every hour should be the initial management of choice. Topical moxifloxacin is easier to obtain but should be reserved for smaller, noncentral ulcers. Steroids should be avoided as initial management but may play a role in minimizing corneal scarring later in the treatment regimen. Topical chlorhexidine is used in cor-neal ulcers from acanthamoeba and would not be used initially in this clinical scenario.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


