 Conjunctival Benign Epithelial Tumors
Conjunctival Benign Epithelial TumorsConjunctival Papilloma of Childhood
General Considerations
Conjunctival papilloma is a virus-induced lesion that generally affects children and young adults (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26). We prefer to use the term “childhood papilloma” to distinguish it from the adult form that usually occurs in the elderly and generally has somewhat different clinical characteristics. In the authors’ clinical series of 1,643 conjunctival tumors, there were 5 childhood papillomas, accounting for 13% of benign epithelial lesions, and 1% of the 1,643 lesions (2).
Clinical Features
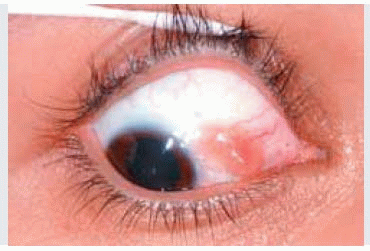
Childhood conjunctival papilloma can be solitary or multiple and may assume a sessile or pedunculated configuration. In extreme cases, several lesions may become confluent, producing massive papillomatosis. Childhood conjunctival papilloma has a fleshy red appearance owing to the numerous fine vascular channels that ramify through the stroma beneath the epithelial surface of the lesion (1,2,3,4,5,6,7,8,9). It most often occurs in the inferior fornix or on the bulbar conjunctiva and rarely encroaches on the cornea (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26). Occasionally, conjunctival papilloma can be pigmented and simulate a melanoma (7). This is more likely to occur in the adult form, which will be discussed in the next section. Conjunctival papilloma of childhood appears to have no malignant potential.
Pathology and Pathogenesis
Histopathologically, childhood conjunctival papilloma shows numerous vascularized papillary fronds lined by acanthotic epithelium, with minimal or no keratinization. The features of the conjunctival papilloma of adulthood are considered in the next section.
Management
The management of childhood conjunctival papilloma has been the subject of considerable interest (17,18,19,20,21,22,23,24,25). Incompletely excised lesions can recur with aggressive behavior owing to surgically induced liberation of virus particles into the surrounding tissues. Double freeze-thaw cryotherapy can be an effective adjunct in eradicating childhood papilloma (18). For fairly circumscribed pedunculated lesions, we have employed cryotherapy to the lesion, lifting and freezing the entire lesion, and immediately cutting the normal conjunctival tissue at its base, followed by closure with absorbable sutures. Larger lesions may require surgical excision with complete removal of the mass and primary closure. A meticulous “no-touch” technique should be attempted, handling only the adjacent, clinically normal tissues. In the rare case where the conjunctival defect cannot be closed primarily, a mucous membrane or amniotic membrane graft may be necessary. Other reported methods include laser treatment (19,20), dinitrochlorobenzene immunotherapy (21), a-interferon (22), and topical mitomycin chemotherapy 0.02% (23,24,26). We have observed dramatic response to recurrent papilloma to oral cimetidine (Tagamet) (25).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


