 Conjunctival and Epibulk Choristomas
Conjunctival and Epibulk ChoristomasConjunctival Dermoid
General Considerations
Most congenital tumors of the conjunctiva are choristomas, which are tumorous malformations composed of tissues not normally present at the involved site (1). A simple choristoma contains one type of tissue; a complex choristoma has more than one type. The main choristomatous tissues that occur in the conjunctiva include skin, bone, lacrimal gland, and cartilage. Most conjunctival choristomas are sporadic and nonhereditary. Both dermoid and dermolipoma are often part of Goldenhar’s syndrome, which also includes auricular and vertebral anolmalies. Dermoid is the second most common epibulbar choristoma, following dermolipoma (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17). In the authors’ clinical series of 1,643 conjunctival tumors, there were 10 dermoids, accounting for 25% of all epibulbar choristomas and for ,1% of all 1,643 lesions (2).
Clinical Features
Small dermoids are often asymptomatic, but larger lesions can cause irritation, astigmatism, and inadequate eyelid closure (6,12). It appears as a variably sized, yellow-white limbal mass inferotemporally but it can appear in other meridians (2,3,4,5,6,7,8,9,10,11). It may range from 2 to 15 mm in diameter and 0 to 10 mm in thickness. Fine white hairs often protrude from the lesion. There is often a yellow-white lipid line in the adjacent corneal stroma. A conjunctival dermoid can show extensive corneal involvement with little involvement of the adjacent conjunctiva (13). It can rarely arise from the caruncle (14). An unusual variant (ring dermoid syndrome) is bilateral, straddles the corneoscleral limbus for 360 degrees and has an autosomal-dominant mode of inheritance (15).
Pathology
Histopathologically, dermoid is lined by stratified squamous epithelium. Deep to the epithelium is dense collagenous tissue in which pilosebaceous units, sweat glands, and fat are often identifiable (2). In rare instances, bone can be present within the dermoid (complex choristoma) (16). It is possible that dermoid develops secondary to faulty eyelid fold closure embryologically with secondary entrapment of skin and mesenchyme.
Management
Smaller asymptomatic dermoids can be observed and larger lesions may require excision (17). Reasons for surgical removal include amblyopia, secondary astigmatism, encroachment on the visual axis, dellen formation, inadequate eyelid closure, and cosmetic considerations. Early removal is advocated for symptomatic lesions to achieve a better cosmetic outcome. However, it is believed that early removal does little to change the astigmatism that was present preoperatively (12). Removal can be achieved by superficial shaving or by deeper excision with lamellar keratoplasty for deeper lesions (12,17).
Selected References
1. Shields JA, Shields CL. Systemic hamartomatoses (“phakomatoses”). In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:536.
2. Shields CL, Demirci H, Karatza E, et al. Clinical survey of 1643 melanocytic and nonmelanocytic tumors of the conjunctiva. Ophthalmology 2004;111:1747-1754.
3. Cunha RP, Cunha MC, Shields JA. Epibulbar tumors in childhood. A survey of 282 biopsies. J Pediatr Ophthalmol 1987;24:249-254.
4. Shields CL, Shields JA. Overview of tumors of the conjunctiva and cornea. In: Foster CS, Azar DT, Dohlman CL, eds. Smolin and Thoft’s The Cornea. 4th ed. Philadelphia: Lippincott, Williams & Wilkins; 2005:735-755.
5. Spencer WH. Conjunctiva. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:38-125.
6. Farah S, Baum TD, Conlon MR, et al. Tumors of the cornea and conjunctiva. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology. 2nd ed. Philadelphia: WB Saunders; 2000:1002-1019.
7. Shields CL, Shields JA. Tumors of the conjunctiva and cornea. Surv Ophthalmol 2004;49:3-24.
8. Elsas FJ, Green WR. Epibulbar tumors in childhood. Am J Ophthalmol 1975;79:1001-1007.
9. Dailey EG, Lubowitz RM. Dermoids of the limbus and cornea. Am J Ophthalmol 1962;53: 661-665.
10. Oakman JH, Lambert SR, Grossniklaus HE. Corneal dermoid: case report and review of classification. J Pediatr Ophthalmol Strabismus 1993;30: 388-391.
11. Burillon C, Durand L. Solid dermoids of the limbus and cornea. Ophthalmologica 1997;211:367-372.
12. Robb RM. Astigmatic refractive errors associated with limbal dermoids. J Pediatr Ophthalmol Strabismus 1996;33:241-243.
13. Shields JA, Laibson PR, Augsburger JJ, et al. Central corneal dermoid. A clinicopathologic correlation and review of the literature. Can J Ophthalmol 1986;21:23-26.
14. Ghafouri A, Rodgers IR, Perry HD. A caruncular dermoid with contiguous eyelid involvement: embryologic implications. Ophthal Plast Reconstr Surg 1998;14:375-377.
15. Mattos J, Contreras F, O’Donnell FE Jr. Ring dermoid syndrome. A new syndrome of autosomal dominantly inherited, bilateral, annular limbal dermoids with corneal and conjunctival extension. Arch Ophthalmol 1980;98:1059-1061.
16. Ferry AP, Hein HF. Epibulbar osseous choristoma within an epibulbar dermoid. Am J Ophthalmol 1970;70:764-766.
17. Mader TH, Stulting D. Technique for the removal of limbal dermoids. Cornea 1998;17:66-67.
Conjunctival Dermoid
Conjunctival dermoid can occur as an isolated lesion or it can be a component of Goldenhar syndrome.
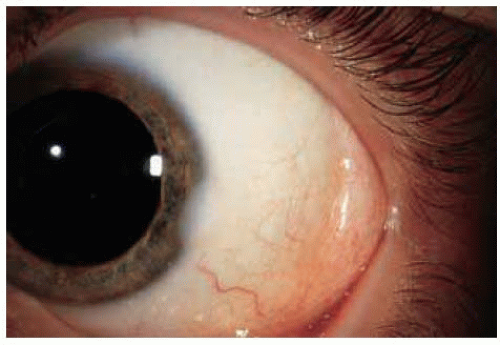 Figure 16.1. Typical round conjunctiva at the corneoscleral lim bus inferotemporally. |
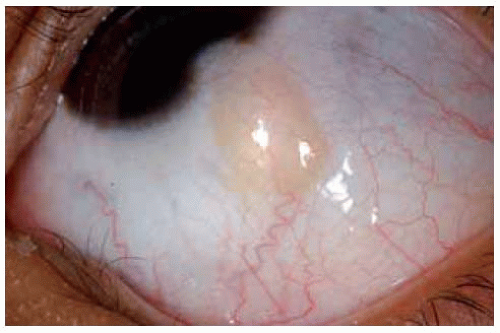 Figure 16.2. Ovoid conjunctival dermoid at limbus inferotemporally in a 12-year-old girl. |
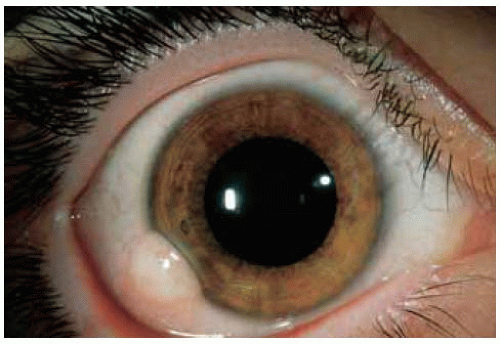 Figure 16.3. Inferotemporal conjunctival dermoid with fine hairs and telangiectasia. |
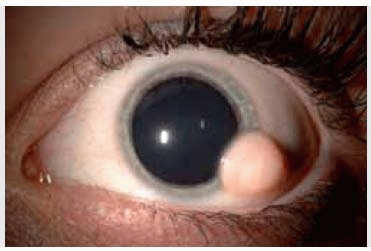
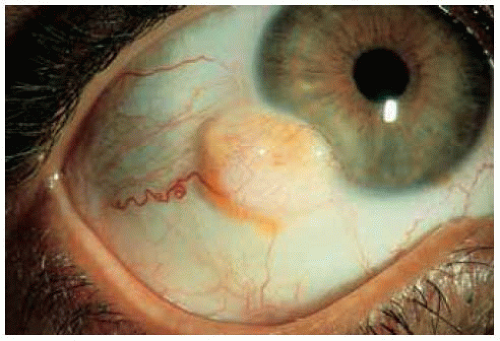 Figure 16.4. Larger limbal dermoid with a dilated blood vessel in a 47-year-old woman with Goldenhar syndrome. |
 Figure 16.5. Preauricular skin appendages in the patient showing in Figure 16.4. The patient also had hearing loss, consistent with Goldenhar syndrome. |
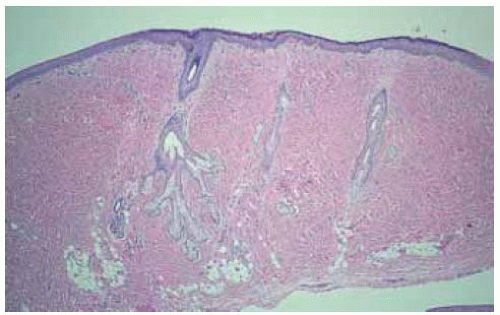 Figure 16.6. Histopathology of limbal dermoid showing several pilosebaceous units in dense collagenous tissue and foci of lipid. (Hematoxylin-eosin 310.) |
Conjunctival and Corneal Dermoids
Dermoids and related choristomas can assume a variety of configurations and management varies with the type and extent of the lesion.
Shields JA, Laibson PR, Augsburger JJ, Michon CA. Central corneal dermoid. A clinicopathologic correlation and review of the literature. Can J Ophthalmol 1986;21:23-26.
 Figure 16.7. Limbal dermoid with subtle corneal lipid line. |
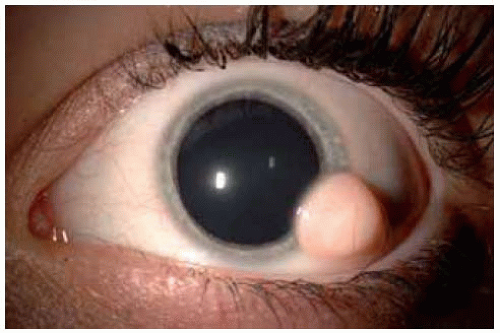 Figure 16.8. Inferotemporal limbal dermoid with a prominent hair. |
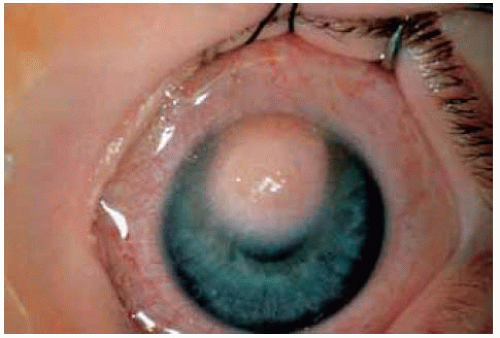 Figure 16.9. Corneal dermoid with minimal limbal involvement superiorly. |
 Figure 16.10. Appearance of patient shown in Figure 16.9 after penetrating keratoplasty. A lamellar keratoplasty was originally planned but it was found at the time of surgery that the lesion extended for full thickness of the corneal stroma. |
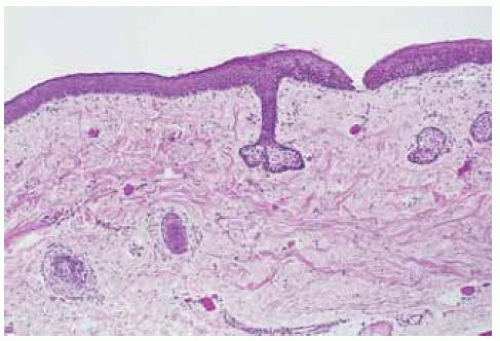 Figure 16.11. Photomicrograph of lesion shown in Figure 16.9 demonstrating pilosebaceous units. (Hematoxylin-eosin 320.) |
 Figure 16.12. Photomicrograph of lesion shown in Figure 16.9 demonstrating pilosebaceous unit in a collagenous stroma within the disorganized corneal stroma. (Hematoxylin-eosin 350.) |
Conjunctival and Corneal Dermoids: Atypical Variations
Sometimes an epibulbar dermoid is more atypical and can have other tissues in addition to dermal elements, meeting criteria for a complex choristoma. Epibulbar dermoid is also known to extend through the limbus into the anterior chamber.
Oakman JH, Lambert SR, Grossniklaus HE. Corneal dermoid: case report and review of classification. J Pediatr Ophthalmol Strabismus 1993;30:388-391.
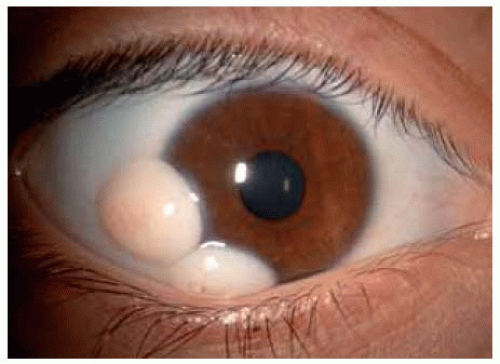 Figure 16.13. Bilobed corneal dermoid. The lesion was present at birth and the patient underwent surgical removal at 15 years of age. (Courtesy of Hans Grossniklaus, MD.) |
 Figure 16.14. Bilobed larger corneal dermoid obscuring the visual axis. The affected eye was enucleated elsewhere because the child was having severe psychosocial problems. (Courtesy of Hans Grossniklaus, MD.) |
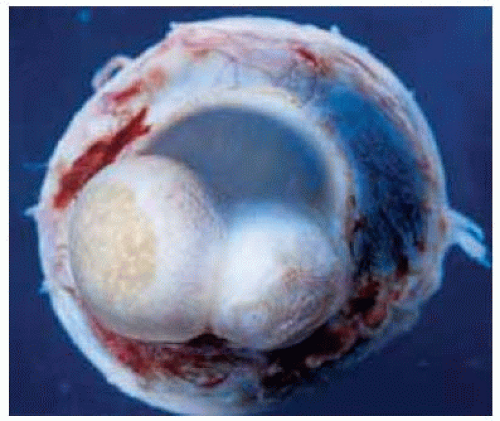 Figure 16.15. Gross appearance of enucleated eye from Figure 16.13 showing the bilobed yellow-white mass on the cornea. (Courtesy of Hans Grossniklaus, MD.) |
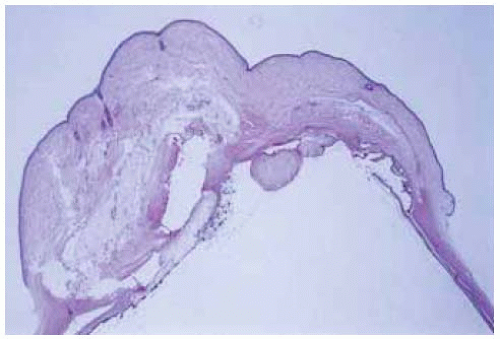 Figure 16.16 Photomicrograph of cornea from Figure 16.13 showing bilobed comeal mass. The lobes were separated by an adherent iris leaflet. (Hematoxylin-eosin 34.) |
 Figure 16.17 Both eyes of a baby at time of examination under anesthesia, showing atypical demoid at the comeoscleral limbus inferiorly. |
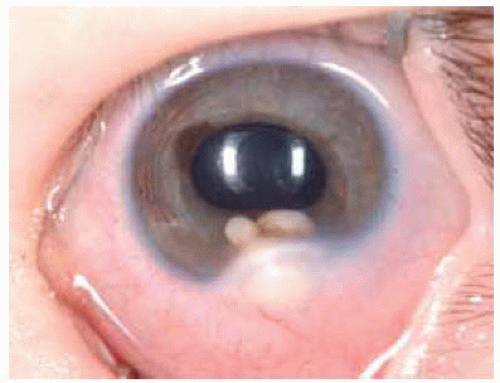 Figure 16.18. Closer view of left eye of child shown in Figure 16.17. The nodules in the anterior chamber were aspirated and they partially collapsed, a finding compatible with a cyst associated with the presumed solid dermoid. Cytopathology showed epithelial cells. |
Conjunctival/Orbital Dermolip
General Considerations
In contrast to a dermoid, dermolipoma (lipodermoid) is less well defined and most often located in the superotemporal conjunctiva, often with extension posteriorly into the orbit (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18). It can occasionally be atypical and even pedunculated. Like dermoid, it is frequently associated with Goldenhar’s syndrome. It can also be a component of the organoid nevus syndrome (18). In the organoid nevus syndrome, the lesion usually has other heterotopic elements, most often cartilage and ectopic lacrimal gland tissue. Dermoid is the second most common epibulbar choristoma, following dermolipoma. In the authors’ clinical series of 1,643 conjunctival tumors, there were 23 dermolipomas, accounting for 58% of all epibulbar choristomas and for 1% of the 1,643 lesions (2).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


