Category
Subtype
Etiology
Congenital
Ocular melanosis
Developmental episcleral hyperpigmentation
Oculodermal melanosis
Acquired
Racial
Normal pigmentation in darker races
Primary
Idiopathic
Secondary
Localized
Post-inflammatory
Posttraumatic
Foreign body
Drug deposition
Systemic
Addison’s disease
Ochronosis
Syndromic
Carney complex
Peutz-Jeghers syndrome
The terminology – primary acquired melanosis or PAM – may be used by the ophthalmologist in a clinical setting to describe any form of flat acquired conjunctival pigmentation that cannot be attributed to a secondary influence. This identification should trigger a biopsy that will allow the pathologist to determine if melanocytic atypia is present (PAM with atypia) or represents just conjunctival pigmentation without any melanocytic atypia (PAM without atypia). The designation of atypia is reserved for the pathologist because it is not possible to predict melanocytic atypia on the basis of clinical criteria alone.
Most recently, Damato and Coupland suggested that the term “PAM” be reserved only to clinical diagnosis and offered the term “conjunctival melanocytic intraepithelial neoplasia (C-MIN) with or without atypia” for the histological terminology of these lesions, with more severe changes regarded as “melanoma in situ.” [8] The authors of this chapter consider that the hybrid nomenclature – one term for the ophthalmologist and another for the pathologist – neither adds value to the classification of the disorder nor does it improve the management. For the remainder of the chapter, therefore, the terminology PAM will be used in a clinical context and PAM with and without atypia when discussing pathology.
The prevalence and natural behavior of PAM are controversial. One study [9] reported the prevalence of PAM in Caucasians with no known non-European ancestry to be 36 %. This number is exceptionally high compared with other studies. It is important to consider that the authors of this study included lesions that were detectable only by slit-lamp high magnification, and some lesions were so small that they would not have been detected on routine clinical examination. Furthermore, there was no histological confirmation of the diagnosis in this series.
17.2 Etiology
PAM is more prevalent in fair-complexioned individuals than in patients with dark skin tones and is almost always unilateral. If bilateral conjunctival pigmentation is encountered, the ophthalmologist should first consider either complexion-associated conjunctival pigmentation or a systemic condition associated with bilateral conjunctival pigmentation.
17.2.1 Sunlight Exposure
The importance of sun exposure in the development of PAM is not clear. However, in one study [9], those who lived south of Washington, DC, for 5 or more years had a significantly greater prevalence of PAM lesions of their exposed intrapalpebral conjunctiva than those who did not. Also, patients with pinguecula or pterygium had higher prevalence of PAM. Silvers et al. [5] noted a high incidence of solar elastosis in biopsy specimens from patients with conjunctival pigmented lesions. These facts suggest a possible role of sunlight exposure, but while they might explain PAM arising in the bulbar conjunctiva in the interpalpebral fissure, they do not explain cases in which PAM originates in the fornices and the palpebral conjunctiva.
17.2.2 Relationship to Nevi and Dysplastic Nevus Syndrome
The prevalence of PAM was shown to increase significantly as the number of facial nevi increases [9]. Seregard et al. [10], in a case–control study, observed that ocular melanocytic lesions, including PAM, are not more common in individuals with dysplastic nevus syndrome than in the general population.
17.2.3 Cigarette Smoking
Cigarette smoking and hypertension have been observed as significant independent factors in the development of PAM [9]. No other etiological factors have been implicated in the development of PAM.
17.3 Clinical Features
Primary acquired melanosis appears clinically as a flat and variably brown conjunctival lesion, ranging from golden brown to dark chocolate in color (Figs. 17.1 and 17.2) [7]. There are no published size criteria for the clinical diagnosis of PAM [9], although in one large series [11] PAM extended for a mean of 3 clock hours, ranging from 1 to 12 clock hours. PAM is usually monocular, although binocular cases may occur. The lesion may involve any area of the conjunctiva in a contiguous or multispotted pattern, necessitating eversion of the eyelids to examine both the upper and lower palpebral zones. PAM develops most commonly at the limbus and epibulbar intrapalpebral region and may extend into the corneal epithelium (Fig. 17.3). According to Shields et al.’s experience with 311 eyes [11], the conjunctival quadrants affected by PAM were temporal, 57 %; inferior, 45 %; nasal, 42 %; and superior, 37 %. In the same study the anatomic locations of PAM included bulbar conjunctiva in 91 %, limbal conjunctiva in 55 %, cornea in 23 %, forniceal conjunctiva in 13 %, palpebral conjunctiva in 12 %, and caruncle in 11 %. In some patients with widespread lesions, the eyelid epidermis may also be involved [7]. PAM occurs typically in middle-aged or elderly white patients, although it may appear also in young adults, but typically not in children. In one study [12] the mean age at the time of diagnosis was 45 years and in another study 62 years [9]. There is no significant difference in the prevalence of PAM between males and females [9], although in one large study [11] 62 % of patients with PAM were female.

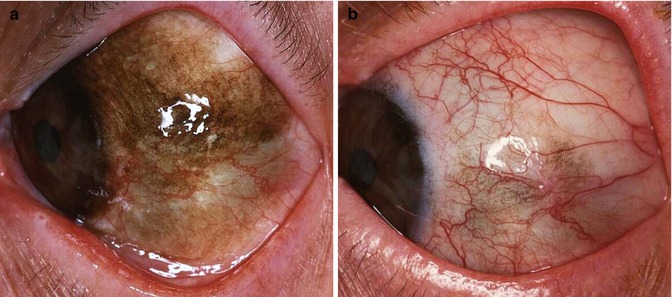
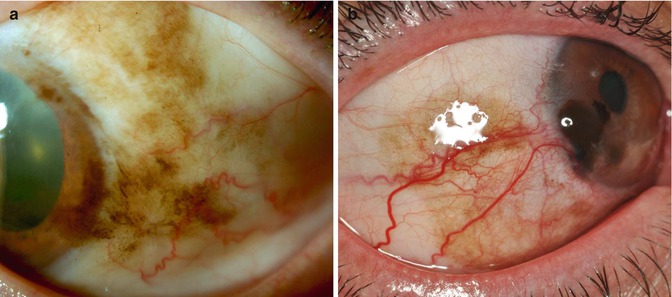
Fig. 17.1
PAM without atypia. Would the lesion be enough to make the diagnosis of PAM and justify a biopsy?
Fig. 17.2
Diffuse PAM with atypia covering the entire temporal part of the bulbar conjunctiva (a). After treatment with topical mitomycin C. Some pigmentation, probably PAM without atypia, has remained unchanged for 6 years (b)
Fig. 17.3
Conjunctival PAM with atypia, with corneal involvement (a). Another case that has progressed to corneo-limbal melanoma (b)
Primary acquired melanosis lesions may remain stable for long periods of time or may grow in size. A “waxing and waning” phenomenon in which areas in the lesions darken or lighten is well known [7]. Parts of, or rarely the entire, PAM lesion can be amelanotic (sine pigmento); thus, the borders of the lesion often cannot be identified, and the clinically identified borders are misleading [12].
17.4 Histopathologic Features
Histologically, PAM is divided into two major groups: PAM without atypia and PAM with atypia. Most conjunctival melanomas arise in the context of PAM with atypia. PAM with atypia is confined to the epithelium and is called by some pathologists “melanoma in situ” [1] and is thus not associated with any risk of metastasis. However, 11–46 % transform to conjunctival melanoma [11, 12]. The mortality of conjunctival melanoma is approximately 25 %. Therefore, a particularly effective treatment for conjunctival melanoma is through prevention by completely extirpating lesions showing histological evidence of PAM with atypia. The lesion designated as PAM without atypia does not evolve into melanoma. As mentioned above, it is important to remember that there are no clinical criteria by which ophthalmologists can anticipate the histological diagnosis. For that reason, an ophthalmologist who encounters a fair-complexioned patient with a unilateral, acquired, flat patch of brown pigmentation should subject the lesion to biopsy to allow the pathologist to classify the lesion as PAM without atypia or PAM with atypia.
17.4.1 Light Microscopy
Histologically, the detection of conjunctival epithelial pigmentation with or without melanocytic hyperplasia – but, without melanocytic atypia – qualifies a lesion to be designated as PAM without atypia (Fig. 17.4). One might think conceptually of such a lesion as an “ephilis” (freckle) or lentigo (despite the fact that there are no rete structures in the normal conjunctiva and therefore “lentigo” is difficult to identify in this location). Histologically, the detection of atypical melanocytes within the epithelium qualifies the lesion to be designated as PAM with atypia.
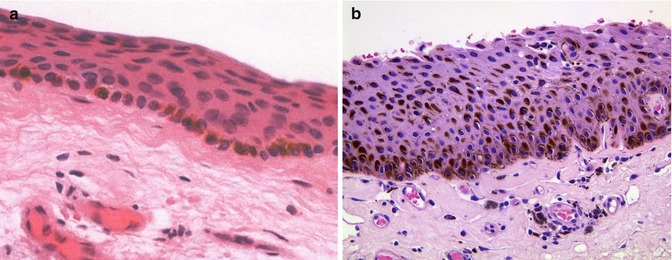
Fig. 17.4
Histologic picture of conjunctival PAM without atypia, with pigmented melanocytes only along the basal layer of the epithelium (a, hematoxylin and eosin, ×20). In this case, melanin pigmentation is distributed throughout the conjunctival epithelium, yet there is no evidence of melanocytic hyperplasia or atypia. This lesion would therefore be designated histologically as conjunctival PAM without atypia (b, hematoxylin and eosin, ×20)
In rendering a diagnosis of PAM with atypia, the pathologist should take note of both cytological and architectural features. Melanocytic atypia is identified through the detection of melanocytes of different sizes and shapes that appear to have a “disregard” (i.e., they are spatially separated from) adjacent epithelial cells (Fig. 17.5). These atypical cells may be small and round, spindled, or even epithelioid. Architecturally, the atypical melanocytes may be distributed along the epithelial basement membrane (basilar hyperplasia pattern), may be segregated into nests that appear to be anchored along the basement membrane, or may be dispersed upward into the epithelium, either individually or as intraepithelial nests (pagetoid spread). In some areas, the atypical melanocytes may completely replace the epithelium. PAM with atypia that extends into pseudoglands of Henle should not be mistaken for invasion (the lining of the pseudoglands is considered to be contiguous with the epithelium).
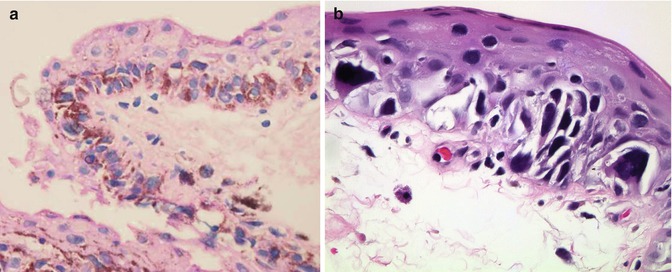
Fig. 17.5
Histologic picture of conjunctival PAM with atypia, showing atypical melanocytes in the basal layers (a, hematoxylin and eosin, ×20). Highly atypical melanocytes populate the conjunctival epithelium singly and in nests. Note the lack of contact between these cells and the epithelium. This lesion should be designated as PAM with atypia (b, hematoxylin and eosin, ×40)
It is important for both pathologists and ophthalmologists to understand that junctional nevi of the conjunctiva are exceptionally rare – even in children. Therefore, the diagnosis of “junctional nevus” when rendered by a pathologist who is not experienced in ophthalmic pathology, especially if the lesion is not taken from a young child, should prompt a review: the lesion is likely to represent PAM with atypia. The histological identification and differential diagnosis of PAM with atypia is among the most difficult in the practice of surgical ophthalmic pathology. In two studies the researchers graded the cellular changes in PAM with atypia and showed higher rates of recurrence [13] and transformation to melanoma [14] in the highly-graded lesions. A detailed description of the histological differential diagnosis is beyond the scope of this chapter, and the reader is referred to a more specialized discourse for details [15].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


