Fig. 15.1
Solitary sessile squamous papilloma of the bulbar conjunctiva. Clinical appearance (a). Histopathology shows papillomatous fronds of acanthotic nonkeratinized squamous epithelium with central fibrovascular cores (b; hematoxylin and eosin, original magnification ×4)
Adulthood Papilloma
In adults, conjunctival squamous papilloma usually appear as single and unilateral lesions, commonly arising close to the limbal area or bulbar conjunctiva. They are usually flat with a broad base, may be large and cover a large area of the conjunctiva, and may cover the cornea and interfere with vision. Sometimes it may be difficult to differentiate them clinically from squamous cell carcinoma.
15.2.1.2 Histopathologic Features
Histologically, the squamous papilloma of childhood is composed of epithelial projections covered by nonkeratinized acanthotic stratified squamous epithelium, which may have goblet cells, and have a fibrovascular core in which acute and chronic inflammatory cells are often found (Fig. 15.1b). The basement membrane is always intact. Human papilloma virus has been demonstrated in these papillomas by various immunohistochemical and molecular techniques [5, 6].
In adults, the squamous papilloma usually has a broader base, and its acanthotic epithelium may show varying degree of epithelial pleomorphism, and even dysplasia can occur, albeit generally mild. Although the lesions are usually nonkeratinized, moderate keratinization may be present. The basement membrane is typically intact.
15.2.1.3 Treatment
Small papilloma in children can be observed, as there usually is a slow spontaneous resolution. However, larger papillomas should be treated by complete surgical excision, preferably by the “no-touch technique” in order to avoid spreading the papilloma-related virus [3]. Cryotherapy is often used in conjunction with surgical excision, either to the conjunctiva around the excised lesion or to the lesion itself that is then excised in frozen state. Sometimes cryotherapy may be performed without excision, letting the lesion slough off the conjunctival surface later.
Conjunctival papillomas tend to recur often, usually when multiple lesions are caused by papillomavirus. Such lesions may be treated by adjuvant interferon alpha-2B locally or systemically [7, 8] or topical mitomycin C [9]. Others have used carbon dioxide laser vaporization [10], and there is one report of effective treatment of recurrent conjunctival papillomas with oral cimetidine [11].
15.2.2 Inverted Papilloma (Inverted Follicular Keratosis)
The lesions derive their name from the propensity to invaginate inward into the underlying conjunctival substantia propria, instead of growing in an exophytic manner outward like the other conjunctival papillomas. Some of the lesions may show a mixed inverted-exophytic papilloma [12].
15.2.2.1 Clinical Features
These are rare lesions that appear as solid or cystic solitary nodules in the conjunctiva. They have been reported to appear in the limbal area, plica semilunaris, and tarsal conjunctiva.
15.2.2.2 Histopathologic Features
Lobules of proliferating epithelium without keratinization or inflammation invaginate the underlying connective tissue. Mucus-producing goblet cells are scattered throughout the lesions, and mucoid material, when it exists, is found in the wall of the cyst.
Unlike inverted papillomas in other sites, such as the nose, paranasal sinuses, and lacrimal sac, conjunctival inverted papilloma does not exhibit locally aggressive behavior, does not involve extensive segments of the conjunctival epithelium, and does not display diffuse spread or multicentricity. Therefore, it is suggested that a clear distinction is made from inverted squamous papillomas of the nasal cavity and sinuses [13]. However, complete removal of these lesions is still recommended.
15.2.3 Seborrheic Keratosis
Seborrheic keratosis of the conjunctiva is extremely rare, and only a very few case reports are found in the medical literature [14]. They mostly appear as a pigmented conjunctival lesion and may be misdiagnosed clinically as conjunctival melanoma. The typical basaloid cell acanthosis and keratin-filled pseudocysts confirm the diagnosis.
15.2.4 Reactive Epithelial Hyperplasia (Pseudoepitheliomatous Hyperplasia and Pseudocarcinomatous Hyperplasia)
This conjunctival lesion is secondary to irritation by concurrent or preexisting stromal inflammation [1–3].
15.2.4.1 Clinical Features
It appears as an elevated leukoplakic pink lesion in the limbal area.
15.2.4.2 Histopathologic Features
Acanthosis, hyperkeratosis or parakeratosis, and subepithelial inflammation are observed. Mitotic figures may be present, but cytologic atypia is generally lacking. Due to the possible clinical and histological difficulty in differentiating such lesions from conjunctival squamous cell carcinoma, it should be completely excised and additional cryotherapy may be considered.
15.2.5 Keratoacanthoma
This is a variant of conjunctival reactive epithelial hyperplasia that does not show spontaneous regression [1, 3, 15].
15.2.5.1 Clinical Features
Keratoacanthoma appears as a benign, solitary, gelatinous, or leukoplakic rapidly-growing nodule on the bulbar conjunctiva surrounded by dilated blood vessels [1, 3, 14]. In some cases, an umbilicated center is observed (Fig. 15.2a).
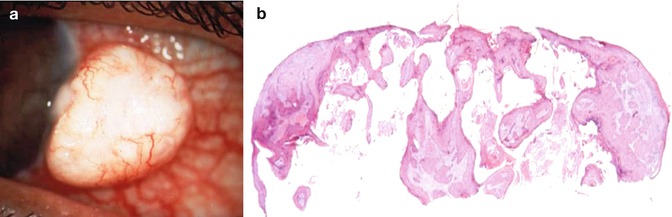
Fig. 15.2
A rapidly growing keratoacanthoma of the bulbar conjunctiva at the limbus. Clinical appearance (a). Histopathology of the lesion in demonstrates squamous epithelium with invasive acanthosis and hyperkeratosis (b; hematoxylin and eosin, original magnification ×2) (Reproduced with permission from Munro et al. [15])
15.2.5.2 Histopathologic Features
The lesion shows marked invasive acanthotic epithelium with keratin-filled pseudocysts, hyperkeratosis, and parakeratosis (Fig. 15.2b). Usually there is minimal cytologic atypia. In cases with marked degree of atypia, it may be difficult to distinguish the lesion from well-differentiated squamous cell carcinoma.
15.2.5.3 Treatment
Therefore, conjunctival keratoacanthoma should be treated by complete excision, and additional cryotherapy should be considered.
15.2.6 Hereditary Benign Intraepithelial Dyskeratosis (HBID)
HBID is an autosomal dominant disorder with a high degree of penetrance occurring in descendants of an inbred isolate of European, African-American, and Native American (Haliwa Indian) origin in northeastern North Carolina. HBID has been subsequently detected in other parts of the United States. Using genetic linkage analysis, the HBID gene was localized to chromosome 4 (4q35) [16].
15.2.6.1 Clinical Features
HBID is characterized by bilateral elevated fleshy plaques on the nasal or temporal perilimbal bulbar conjunctiva, with dilated conjunctival vessels around it, causing the eye to appear red [1, 3] (Fig. 15.3a). In mild cases the patients are asymptomatic, but in severe cases most of the bulbar conjunctiva and cornea are involved, causing corneal opacification and vascularization leading to loss of vision. Patients may complain of foreign body sensation, photophobia, and tearing, especially in the spring. Similar lesions may occur in the buccal mucosa.
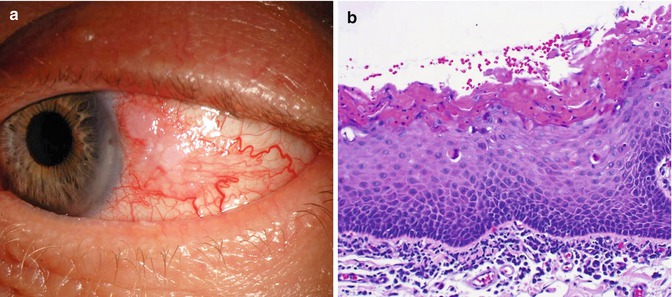
Fig. 15.3
Hereditary benign intraepithelial dyskeratosis. Typical clinical appearance is of a white lesion of the temporal conjunctiva with dilated conjunctival vessels around it (a). Histopathology showing acanthosis, hyperkeratosis, dyskeratosis, and marked chronic inflammation in the stroma beneath the intact basement membrane (b; hematoxylin and eosin, original magnification ×20) (Courtesy of Gordon Klintworth, MD)
15.2.6.2 Histopathologic Features
The lesions are characterized by acanthosis, prominent dyskeratosis in the surface and deep epithelium, and severe chronic inflammation in the stroma (Fig. 15.3b). The basement membrane is intact. The lesions do not have malignant potential.
15.2.6.3 Treatment
HBID usually does not require aggressive treatment. Mild cases can be treated by ocular lubricants, and, if needed, by topical corticosteroids. Larger lesions can be treated by local excision. Mucous membrane grafting can be used when the excision is wide. Recurrence of HBID lesions is common.
15.2.7 Dacryoadenoma
Dacryoadenoma is a rare conjunctival tumor that occurs in children and young adults. It appears as translucent pink lesion in the bulbar, forniceal, or palpebral conjunctiva [3]. It is uncertain whether the lesion is congenital or acquired. Histologically it is a benign epithelioid cell proliferation forming glandular lobules, similar to the lacrimal gland. In one reported case, scattered myoepithelial cells were associated with acinar-type epithelium, and goblet cells were intermixed [17]. The lesions are treated by simple excision.
15.2.8 Oncocytoma
Oncocytoma, known also as oxyphilic cell adenoma, is a rather common lesion of the lacrimal gland. It often arises in the caruncle or adjacent plica semilunaris and canthal conjunctiva as a slowly-growing benign yellow-tan or reddish lesion in older individuals, mostly women [2, 18]. Histologically, large cells with eosinophilic granular cytoplasm are arranged in nests, cords, or sheets and may form glandular or ductal structures. Ultrastructurally, the cytoplasm is laden with mitochondria. The lesion is treated by simple excision. Rarely, the tumor may undergo carcinomatous transformation.
15.2.9 Epithelial Cysts
Conjunctival cysts are common and may be congenital or acquired. The acquired cysts are more common and are mostly epithelial inclusion cysts that can occur spontaneously or following surgical or nonsurgical trauma [1, 3] (Fig. 15.4). Other common cysts are ductal cysts, usually of accessory lacrimal gland origin (Fig. 15.5).
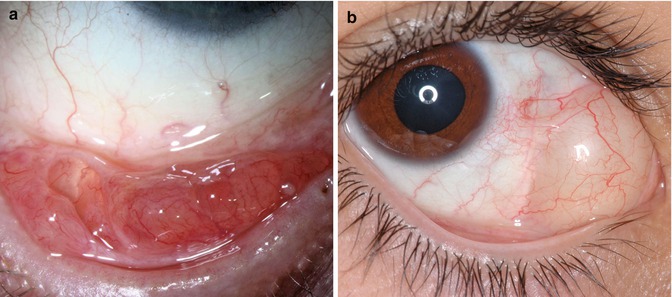
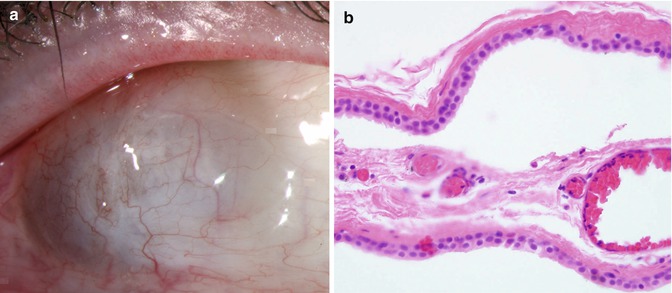
Fig. 15.4
Epithelial inclusion cyst. Multiple cysts in the inferior fornix (a). A large conjunctival cyst in the nasal bulbar conjunctiva that occurred after strabismus surgery (b)
Fig. 15.5
Ductal cyst. Bluish cyst in the temporal bulbar conjunctiva. Posterior margin of the cyst cannot be visualized (a). The cyst lined by two cell layers, with luminal cells showing apical snouts, consistent with apocrine differentiation. The double cell lining is consistent with a ductal-type cyst, possibly from an accessory lacrimal gland. Apocrine differentiation may be metaplastic (b, hematoxylin and eosin stain, 40× magnification) (Reproduced with permission from Aponte et al. [31])
15.2.9.1 Clinical Features
The conjunctival cyst is a smooth translucent lesion that contains clear fluid, although the fluid may be turbid or contain epithelial debris in the lumen that is layered like pseudohypopyon. In dark-skinned patients, the cyst can be pigmented.
15.2.9.2 Histopathologic Features
The epithelial inclusion cyst is lined by conjunctival epithelium. The lumen can be clear or it can contain mucinous material, epithelial debris, and occasionally keratin. Ductal cysts are lined by two layers of epithelium and may contain PAS-positive material.
15.2.9.3 Treatment
The cyst can be stable and asymptomatic or can enlarge and become symptomatic, necessitating excision. In most cases, over the long-term follow-up, the cyst eventually undergoes spontaneous resolution.
15.2.10 Keratotic Plaque
This is a leukoplakic lesion that may develop in the limbal or bulbar conjunctiva, usually in the interpalpebral region [1, 2]. Histologically there is a focal thickening of keratin and epithelial layer, characterized mainly by acanthosis, hyperkeratosis, or parakeratosis. No dyskeratosis is seen. These lesions have little or no potential for carcinomatous changes.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


