 Conjunctiva Melanocytic Lesions
Conjunctiva Melanocytic LesionsConjunctival Melanocytic Nevus
General Considerations
Nevus is the most common melanocytic conjunctival tumor (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34). In the authors’ clinical series of 1,643 conjunctival tumors, there were 454 nevi, accounting for 52% of conjunctival melanocytic lesions and for 28% of the 1,643 lesions (3).
There is controversy as to whether conjunctival nevi are congenital or acquired (1). It generally becomes clinically apparent in the first or second decade of life (1,2,3,4,10). The nevus begins as a small nest of melanocytes in the basal layer of the epithelium, at which stage it is called a “junctional” nevus. In the second to third decade of life, the cells gradually migrate into the underlying stroma to form a “compound” nevus. At this stage, characteristic pseudocysts form in the lesion. By the third to fourth decade, the lesion has migrated to reside entirely in the stroma, forming a “subepithelial” nevus (1). It is helpful to consider these three types as stages in the evolution of a nevus, rather than distinct types (1).
Melanocytic nevus of the conjunctiva is generally sporadic with no systemic associations. However, lentigines and nevi are rarely associated with Carney complex and the dysplastic nevus syndrome (DNS) (22). Carney complex is also mentioned in the sections on eyelid and conjunctival myxomas in this atlas. The DNS is an autosomal-dominant entity characterized by numerous dysplastic cutaneous nevi and a high incidence of cutaneous melanoma. There may be an increased incidence of conjunctival nevi (and melanoma) in association with DNS (20).
Clinical Features
A recent study of 410 consecutive cases of conjunctival nevi seen by the authors revealed that 89% occurred in Caucasians, 6% in African Americans, and 5% in Asian, Hispanic, or Indian subjects (4). It contained clinically evident pigment in 84% and was clinically amelanotic in 16%. It was located in the bulbar conjunctiva in 72%, caruncle in 15%, semilunar fold in 11%, and fornix, tarsus, and cornea in 1% each. About 90% were located in the interpalpebral area with relative equal distribution nasally and temporally (2). Malignant transformation was estimated to be less than 1%, a finding that is similar to other series (18).
Conjunctival nevus is usually a discrete, mobile lesion on the bulbar conjunctiva, most often in the interpalpebral area. It can range from deeply pigmented to amelanotic. It may become more pigmented with time and this change is misinterpreted by the patient, and sometimes by the physician, as malignant transformation. However, true increase in size sometimes occurs in young children and such enlargement does not necessarily mean malignant transformation into melanoma (34). When it is not pigmented, the presence of multiple, clear cystic spaces seen in the lesion with slit-lamp biomicroscopy help to differentiate nevus from papilloma, lymphoma, and amelanotic melanoma, which generally do not have cysts. Lymphangioma, on the other hand, can have cystlike spaces and resemble a diffuse amelanotic nevus (1,2,12).
Another common clinical variant is what the authors call a speckled nevus. It is less well defined and appears as a patchy area of pigmentation in the conjunctiva. It may closely resemble primary acquired melanosis (PAM), to be discussed shortly, except that it generally occurs in younger individuals and sometimes contains subtle clear cysts, a finding not seen with PAM.
In rare cases, a blue nevus can occur in the conjunctiva. It is often congenital and appears clinically as a blue to black, circumscribed or slightly ill-defined lesion deep to the conjunctival epithelium that differs from the more diffuse scleral or episcleral melanocytosis (1,23). Conjunctival blue nevus can have a diffuse growth pattern and resemble primary acquired melanomas. Such a diffuse blue nevus can rarely undergo malignant transformation into melanoma (21).
Although most nevi develop in the interpalpebral region, they can be located in the extralimbal bulbar conjunctiva, semilunar fold, or caruncle. In rare instances, they can apparently be confined to the palpebral conjunctiva (11) or cornea (24). Such locations should raise suspicion that the lesion is an early melanoma.
In some instances, a conjunctival nevus can assume an irregular or diffuse growth pattern. Such an atypical nevus can occupy a large portion of the conjunctiva and lead to diagnostic confusion with PAM, melanoma and, in the case of amelanotic lesions, with lymphoma or lymphangioma (12). A relatively common occurrence with conjunctival nevus is secondary inflammation, which may simulate primary conjunctivitis or episcleritis (34). However, slit-lamp biomicroscopy often discloses the typical cysts that characterize the nevus.
Pathology
The histopathological classification of nevi is discussed in the literature (1,2). Although most pathologists accustomed to evaluating ocular tissues can make the diagnosis without difficulty, there are some cases where the lesion has borderline malignant features and even experienced ocular pathologists may have difficulty classifying the lesion as benign or malignant (29). Histopathologically, a conjunctival nevus is composed of a diffuse infiltration or distinct nests of benign melanocytes near the basal layer of the epithelium. Depending on their relationship to the layers of the conjunctiva, they are most often classified as junctional, compound, or deep (1,3). Depending on their cytology and other features, they may be classified as dysplastic nevus, spindle cell nevus, epithelioid cell nevus, balloon cell nevus, or a combination of these variants (1,13,27).
A blue nevus is uncommon in the conjunctiva. It may be identical to the typical congenital or acquired nevus, except that it is more likely to be deep to the conjunctival epithelium, sometimes partially attached to the sclera. It may be dark brown or black and it is less likely to contain cysts.
A variety of other nevi can be occasionally recognized in the conjunctiva histopathologically. There have been examples
of balloon cell nevus, Spitz nevus, epithelioid cell nevus, dysplastic nevus, and melanocytoma in the conjunctiva (8,13).
of balloon cell nevus, Spitz nevus, epithelioid cell nevus, dysplastic nevus, and melanocytoma in the conjunctiva (8,13).
On occasion, a conjunctival nevus shows features of both a conventional nevus and deeper dendritic cells that characterize a blue nevus. Such a lesion has been called a “combined” nevus. It has recently been stressed that such a nevus may be more common than previously suspected and must be differentiated from a melanoma (16,28).
Currently used immunohistochemical techniques can be used to differentiate melanocytic lesions from nonmelanocytic conditions. However, the popular melanoma-specific antigen (HMB-45) generally shows a positive reaction with both nevus and melanoma and cannot be reliably used to differentiate benign from malignant melanocytic lesions (30).
Management
The best initial management for a small, typical conjunctival nevus is periodic observation with photographs. If growth is documented, local excision of the lesion should be considered. However, relative indications for earlier excision include location in the forniceal or palpebral conjunctiva or cornea, nutrient blood vessels, larger lesion that contains no cysts, positive family history of conjunctival or cutaneous melanoma, distinct onset of the lesion in middle age or later in life, insistence of the patient or parents, and cancerophobia. In addition, any recurrence of a previously excised conjunctival nevus should be removed. Such a recurrence should raise the possibility of malignant transformation. We have sometimes removed a small lesion believed clinically to be a nevus and were surprised to find that it was a melanoma histopathologically.
If a lesion shows suspicious change or growth, it is important that an excisional biopsy be done, using a reported technique, described later in this chapter and illustrated in Chapter 25. As a general rule, incisional biopsy is contraindicated in lesions that can be resected entirely in one procedure. The resection technique that we employ is the same as that used for malignant neoplasms, like squamous cell carcinoma, and other lesions near the limbus. It involves a partial alcohol epitheliectomy, removal of the main tumor by partial lamellar sclerokeratoconjunctivectomy, and double freeze thaw cryotherapy (33).
Selected References
1. Folberg R. Melanocytic lesions of the conjunctiva. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:125-147.
2. Shields CL, Fasiudden A, Mashayekhi A, et al. Conjunctival nevi: clinical features and natural course in 410 consecutive patients. Arch Ophthalmol 2004;122:167-175.
3. Farah S, Baum TD, Conlon MR, et al. Tumors of the cornea and conjunctiva. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology. 2nd ed. Philadelphia: WB Saunders; 2000:1002-1019.
4. Shields CL, Shields JA. Overview of tumors of the conjunctiva and cornea. In: Foster CS, Azar DT, Dohlman CL, eds. Smolin and Thoft’s The Cornea. 4th ed. Philadelphia: Lippincott, Williams & Wilkins; 2005:735-755.
5. Shields JA, Shields CL. Tumors of the conjunctiva. In: Stephenson CM, ed. Ophthalmic Plastic, Reconstructive and Orbital Surgery. Stoneham, MA: Butterworth-Heinemann; 1997:263.
6. Shields CL, Shields JA. Tumors of the conjunctiva and cornea. Surv Ophthalmol 2004;49:3-24.
7. Shields CL, Demirci H, Karatza E, et al. Clinical survey of 1643 melanocytic and nonmelanocytic tumors of the conjunctiva. Ophthalmology 2004;111:1747-1754.
8. Folberg R, Jakobiec FA, Bernardino VB, et al. Benign conjunctival melanocytic lesions. Clinicopathologic features. Ophthalmology 1989;96:436-461.
9. Grossniklaus HE, Green WR, Luckenbach M, et al. Conjunctival lesions in adults. A clinical and histopathologic review. Cornea 1987;6:78-116.
10. McDonnell JM, Carpenter JD, Jacobs P, et al. Conjunctival melanocytic lesions in children. Ophthalmology 1989;96:986-993.
11. Buckman G, Jakobiec FA, Folberg R, et al. Melanocytic nevi of the palpebral conjunctiva. An extremely rare location usually signifying melanoma. Ophthalmology 1988;95:1053-1057.
12. Rosenfeld SI, Smith ME. Benign cystic nevus of the conjunctiva. Ophthalmology 1983;90:1459-1461.
13. Jakobiec FA, Zuckerman BD, Berlin AJ, et al. Unusual melanocytic nevi of the conjunctiva. Am J Ophthalmol 1985;100:100-103.
14. Liesegang TJ. Pigmented conjunctival and scleral lesions. Mayo Clin Proc 1994;69:151-161.
15. Rodriguez-Sains RS. Pigmented conjunctival neoplasms. Orbit 2002;21:231-238.
16. Kabukcuoglu S, McNutt NS. Conjunctival melanocytic nevi of childhood. J Cutan Pathol 1999;26:248-252.
17. Farber M, Schutzer P, Mihm MC Jr. Pigmented lesions of the conjunctiva. J Am Acad Dermatol 1998;38:971-978.
18. Gerner N, Norregaard JC, Jensen OA, et al. Conjunctival naevi in Denmark 1960-1980. A 21-year follow-up study. Acta Ophthalmol Scand 1996;74:334-337.
19. Jakobiec FA, Folberg R, Iwamoto T. Clinicopathologic characteristics of premalignant and malignant melanocytic lesions of the conjunctiva. Ophthalmology 1989;96:147-166.
20. Friedman RJ, Rodriguez-Sains R, Jakobiec F. Ophthalmologic oncology: conjunctival malignant melanoma in association with sporadic dysplastic nevus syndrome. J Dermatol Surg Oncol 1987;13:31-34.
21. Demirci H, Shields CL, Shields JA, et al. Malignant melanoma arising from unusual conjunctival blue nevus. Arch Ophthalmol 2000;118:1581-1584.
22. Carney JA. Carney complex: the complex of myxomas, spotty pigmentation, endocrine overactivity, and schwannomas. Semin Dermatol 1995;14:90-98.
23. Blicker JA, Rootman J, White VA. Cellular blue nevus of the conjunctiva. Ophthalmology 1992;99:1714-1717.
24. Shields JA, Shields CL, Eagle RC Jr, et al. Compound nevus of the cornea simulating a foreign body. Am J Ophthalmol 2000;130:235-236.
25. Eller AW, Bernardino VB. Blue nevi of the conjunctiva. Ophthalmology 1983;90:1469-1471.
26. Pfaffenbach DD, Green WR, Maumenee AE. Balloon cell nevus of the conjunctiva. Ophthalmology 1972;87:192-195.
27. Seregard S. Pigmented spindle cell naevus of reed presenting in the conjunctiva. Acta Ophthalmol Scand 2000;78:104-106.
28. Crawford JB, Howes EL Jr, Char DH. Combined nevi of the conjunctiva. Arch Ophthalmol 1999;117:1121-1127.
29. Margo CE, Roper DL, Hidayat AA. Borderline melanocytic tumor of the conjunctiva: diagnostic and therapeutic considerations. J Pediatr Ophthalmol Strabismus 1991;28:268-270.
30. Glasgow BJ, McCall LC, Foos RY. HMB-45 antibody reactivity in pigmented lesions of the conjunctiva. Am J Ophthalmol 1990;109:696-700.
31. McDonnell JM, Mayr AJ, Martin WJ. DNA of human papillomavirus type 16 in dysplastic and malignant lesions of the conjunctiva and cornea. N Engl J Med 1989;320:1442-1446.
32. Kantelip B, Boccard R, Nores JM, et al. A case of conjunctival Spitz nevus: review of literature and comparison with cutaneous locations. Ann Ophthalmol 1989;21:176-179.
33. Shields JA, Shields CL, De Potter P. Surgical management of circumscribed conjunctival melanomas. Ophthal Plast Reconstr Surg 1998;14:208-215.
34. Zamir E, Mechoulam H, Micera A, et al. Inflamed juvenile conjunctival naevus: clinicopathological characterisation. Br J Ophthalmol 2002;86:28-30.
Conjunctival Melanocytic Nevus: Pigmented Type
Most conjunctival nevi are pigmented and located near the limbus in the interpalpebral region. Characteristic clear cysts in the lesion strongly support the diagnosis of compound nevus. Conjunctival nevus can be completely pigmented, partly pigmented, or nonpigmented.
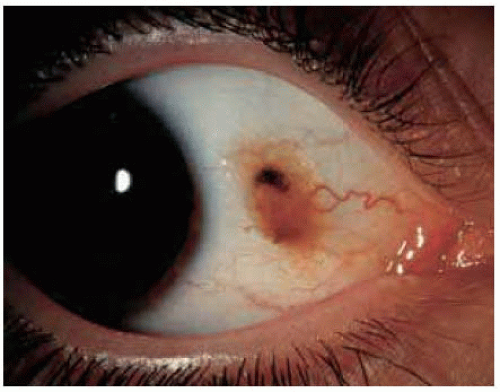 Figure 19.1. Typical conjunctival nevus in a 43-year-old man. |
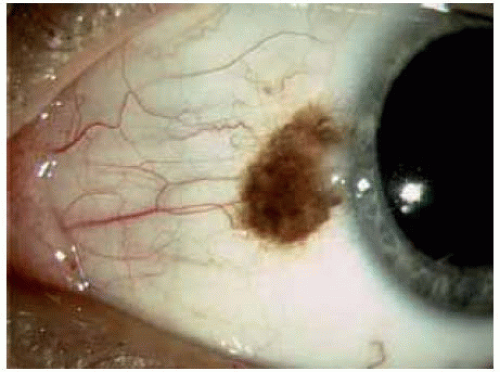 Figure 19.2. Characteristic conjunctival nevus showing subtle clear cystic spaces. |
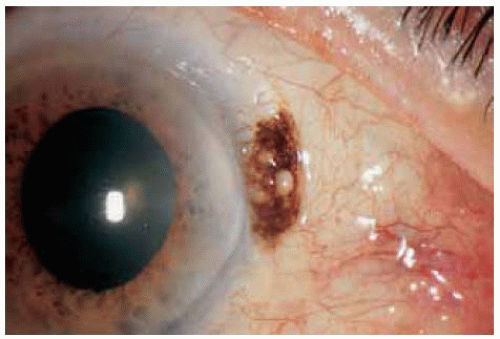 Figure 19.3. Characteristic conjunctival nevus with more distinct clear cystic spaces. |
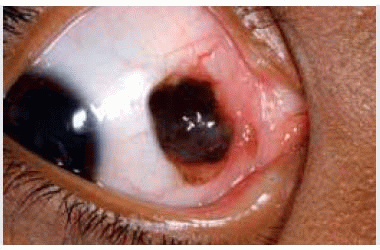
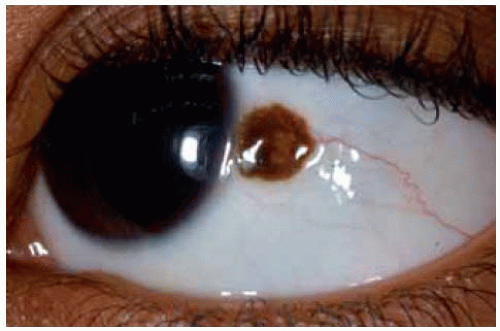 Figure 19.4. Deeply pigmented conjunctival nevus in African American child. Note the associated dilated conjunctival blood vessel. |
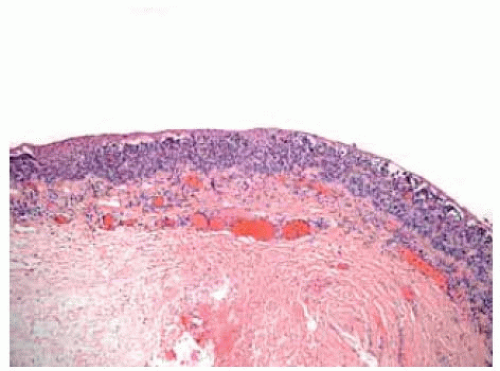 Figure 19.5. Histopathology of functional conjunctival nevus showing diffuse atypical melanocytes in the deeper layers of the conjunctival epithelium. In this case, there are no large cysts. (Hematoxylin-eosin 10.) |
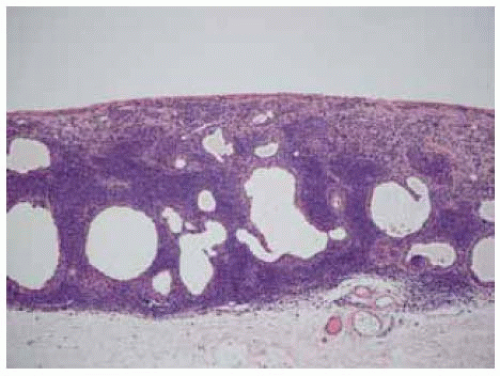 Figure 19.6. Histopathology of compound conjunctival nevus showing numerous cysts within the lesion, lined by conjunctival epithelium. (Hematoxylin-eosin 20.) |
Conjunctival Melanocytic Nevus: Nonpigmented Type
Some conjunctival melanocytic nevi have no apparent pigment on clinical examination. Typical cysts within the lesion on slit-lamp examination, however, should suggest the diagnosis of nevus. All of the lesions shown here had typical cysts, but cysts are not appreciated in every case. Such an amelanotic nevus can become inflamed periodically and be confused with conjunctivitis or episcleritis.
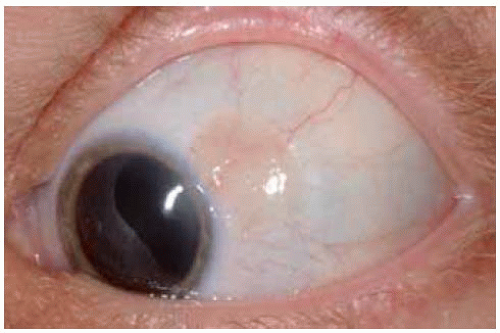 Figure 19.7. Light pink conjunctival nevus in a 13-year-old boy. |
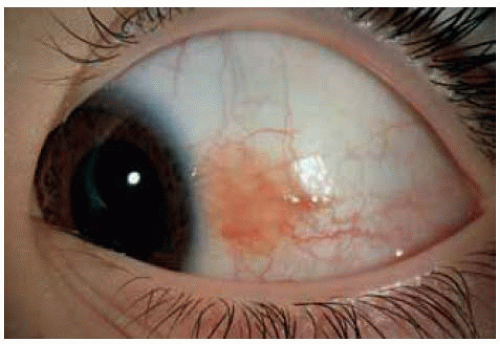 Figure 19.8. Nonpigmented conjunctival nevus near limbus in a 50-year-old man. |
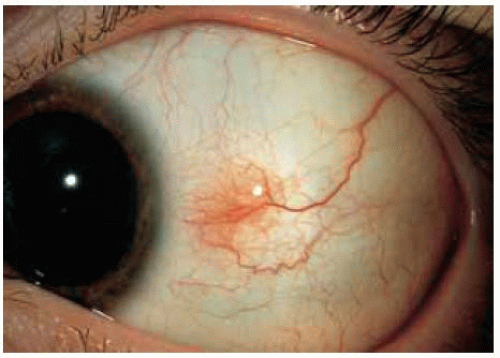 Figure 19.9. Subtle conjunctival nevus with slightly prominent feeder vessel in a 20-year-old man. |
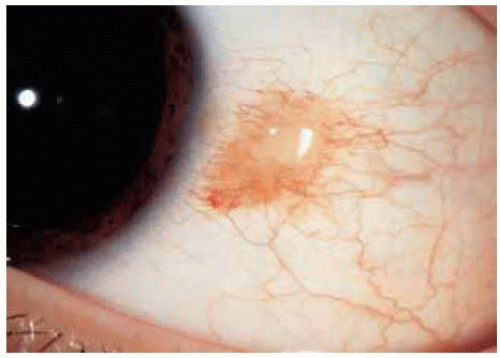 Figure 19.10. Amelanotic conjunctival nevus with minimal peripheral pigmentation in a 13-year-old girl. |
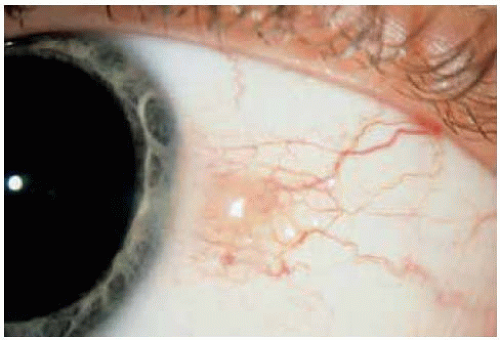 Figure 19.11. Light pink conjunctival nevus in a 9-year-old boy. |
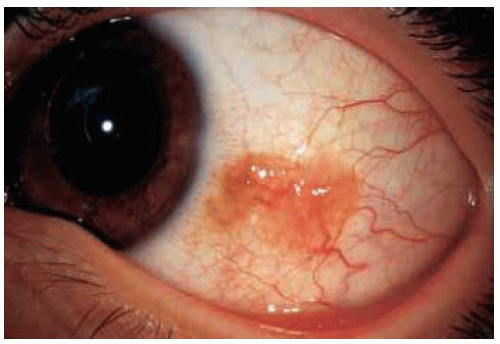 Figure 19.12. Larger, more irregular, salmon-colored conjunctival nevus in a 14-year-old boy. |
Conjunctival Melanocytic Nevus: Partially Pigmented Type
In some instances, a conjunctival nevus is only partly pigmented. The presence of even minimal pigmentation should strongly suggest that the lesion is a melanocytic nevus.
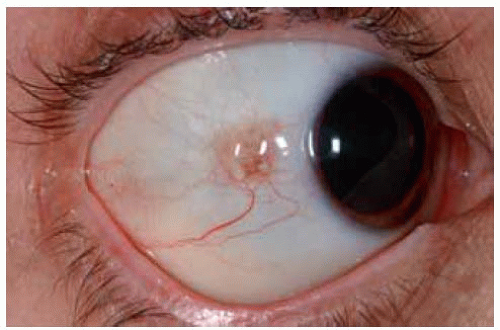 Figure 19.13. Slightly pigmented conjunctival nevus on temporal bulbar conjunctiva. Note the dilated blood vessel. |
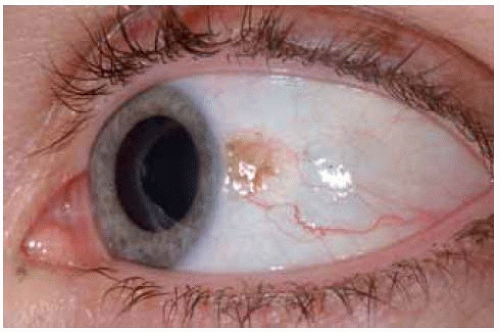 Figure 19.14. Slightly pigm ented conjunctival nevus at lim bus with mildly dilated vessels. |
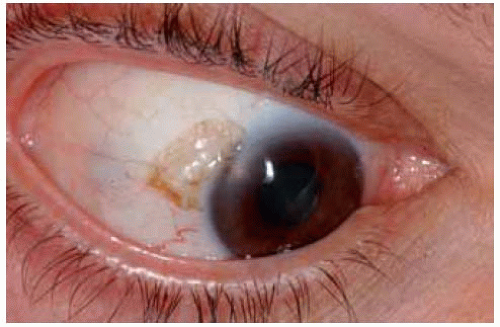 Figure 19.15. Partially pigmented cystic conjunctival nevus with corneal stroma opacity. |
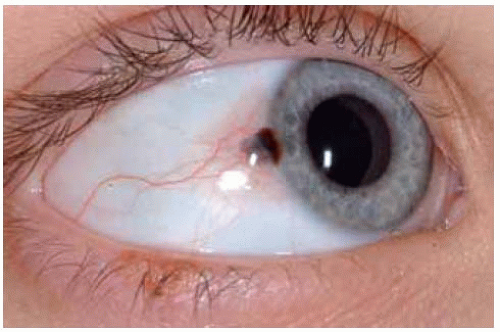 Figure 19.16. Mostly nonpigmented conjunctival nevus with well-defined central focus of pigmentation. |
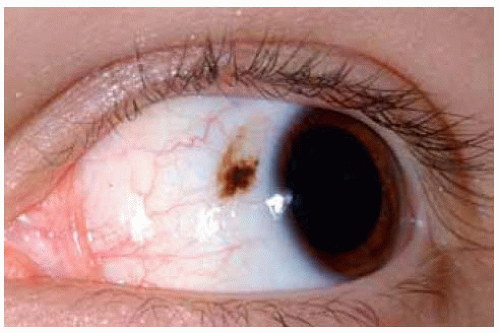 Figure 19.17. Conjunctival nevus with pigmented inferior portion and nonpigmented superior portion. |
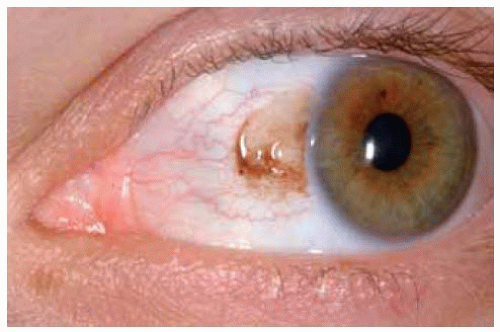 Figure 19.18. Gelatinous nonpigmented conjunctival nevus with irregular rim of pigmentation. |
Conjunctival Melanocytic Nevus: Clinical Variations
Conjunctival nevi can vary in size, color, and location. Occasionally, a conjunctival nevus may be apparently confined to the cornea. There are some atypical clinical and histopathologic variations of conjunctival nevus. Selected examples include the speckled nevus that might resemble primary acquired melanosis, epithelioid cell nevus, corneal nevus.
Shields JA, Shields CL, Eagle RC Jr, et al. Compound nevus of the cornea simulating a foreign body. Am J Ophthalmol 2000;130:235-236.
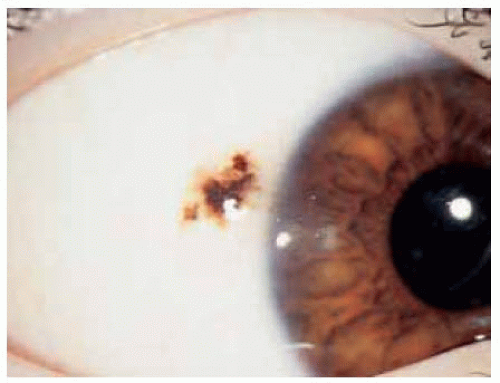 Figure 19.19. Speckled nevus in a 7-year-old boy. |
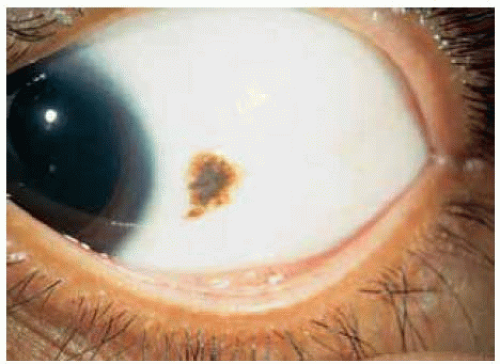 Figure 19.20. Speckled nevus in a 33-year-old woman. |
 Figure 19.21. Example of epithelioid cell nevus. Deeply pigmented nevus in inferior fornix of a 12-year-old girl. |
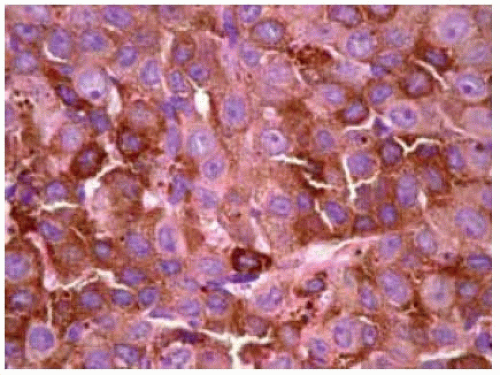 Figure 19.22. Pathology of the lesion shown in Figure 19.21 showing large, round, pigmented cells with abundant cytoplasm uniform nuclei, prominent uniform nucleoli, and lack of mitotic activity. (Hematoxylin-eosin 250.) |
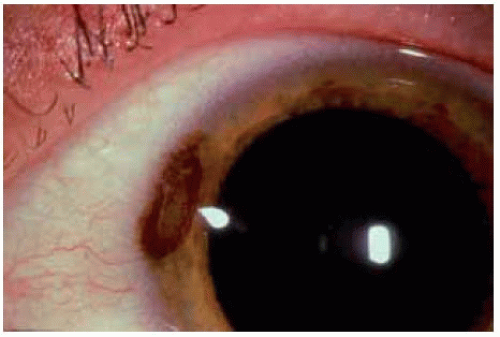 Figure 19.23. Nevus of peripheral cornea in a 22-year-old man, resembling a rusty corneal foreign body. |
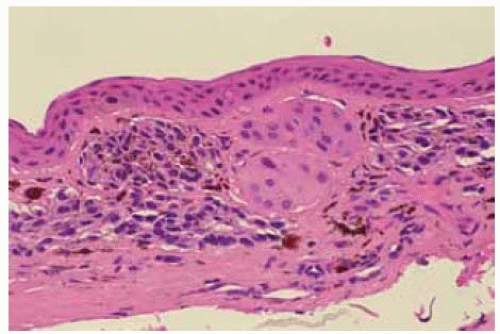 Figure 19.24. Histopathology of lesion shown in Figure 19.23 showing clusters of deep nevus cells within the peripheral corneal stroma. (Hematoxylin-eosin 50.) |
Conjunctival Melanocytic Nevus: Extralimbal Location
Nevi can often be located in the extralimbal bulbar conjunctiva, semilunar fold (plica semilunaris), and the caruncle. Caruncular lesions are discussed and illustrated later.
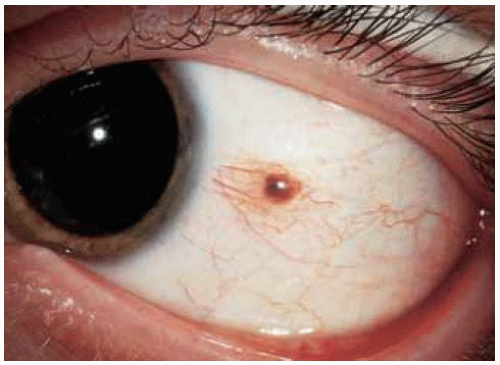 Figure 19.25. Small, slightly elevated lesion in temporal bulbar conjunctiva in a 20-year-old man. |
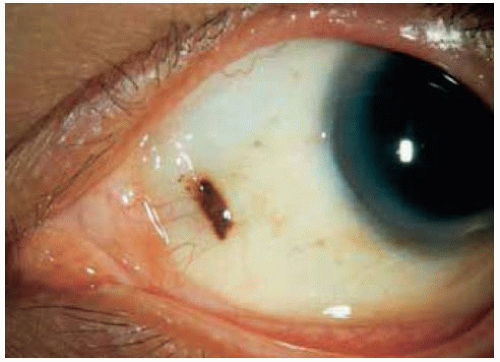 Figure 19.26. Nevus in nasal bulbar conjunctiva just central to the semilunar fold in a 43-year-old man. Note the dusting of pigment around the main lesion. |
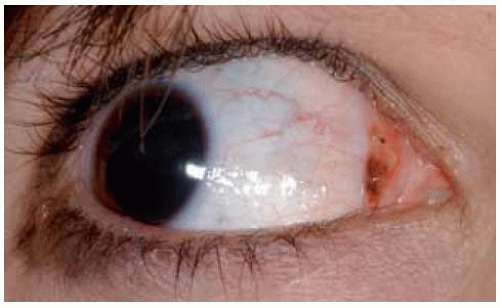 Figure 19.27. Lightly pigmented nevus of semilunar fold in young woman. |
 Figure 19.28. More heavily pigmented conjunctival nevus in semilunar fold of left eye. |
 Figure 19.29. Nevus in inferonasal conjunctival fornix in a middle-aged woman. |
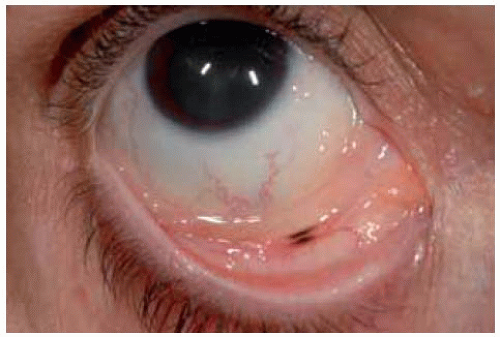 Figure 19.30. Nevus in conjunctival fornix in a 30-year-old woman. |
Conjunctival Melanocytic Nevus: Lesions With Prominent Cysts
In some instances, the cysts within a conjunctival nevus can be very prominent and suggest the diagnosis of a primary cystic lesion or a lymphangioma.
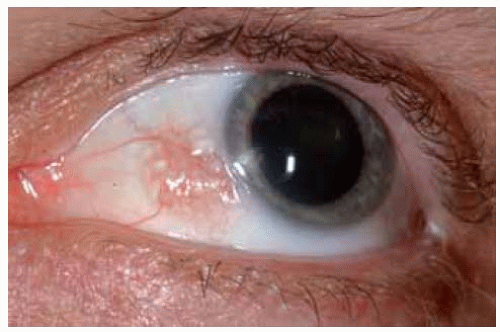 Figure 19.31. Amelanotic cystic conjunctival nevus near limbus. |
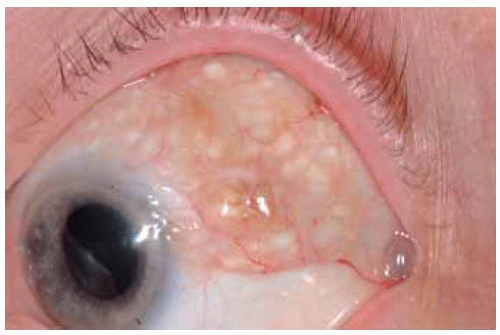 Figure 19.32. Minimally pigmented extensive superior conjunctival nevus with cysts. |
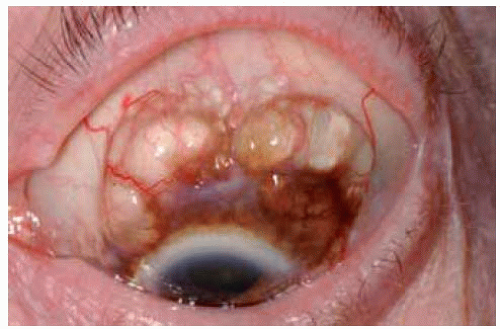 Figure 19.33. Pigmented conjunctiva with giant cysts in an elderly man. The lesion had been present and unchanged since childhood. |
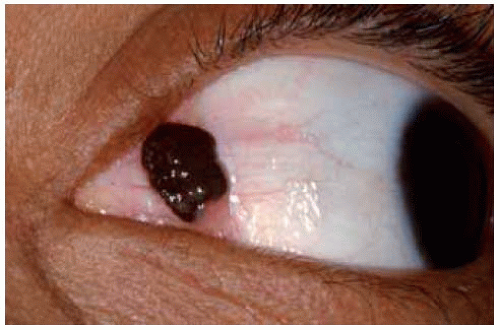 Figure 19.34. Dark black, heavily pigmented cystic nevus of conjunctival semilunar fold in an African American patient. The cysts were obscured by the dense pigment but were evident on slit-lamp biomicroscopy. |
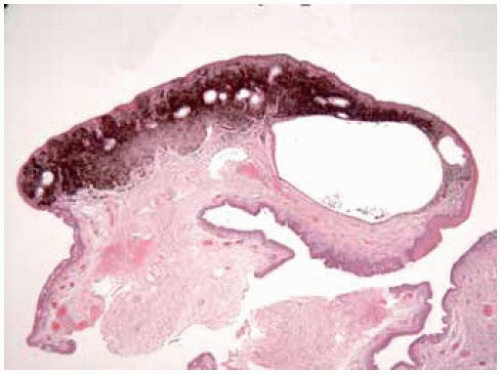 Figure 19.35. Low-magnification photomicrograph of lesion shown in Figure 19.34 depicting superficial pigment and deep cyst. Goblet cells lining the cyst are barely visible. (Hematoxylin-eosin 25.) |
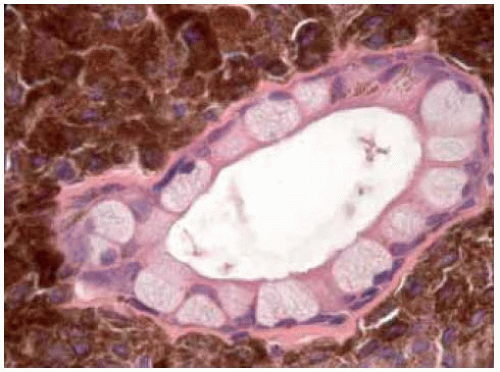 Figure 19.36. Higher power view showing one of the cystic structures with very evident goblet cells. (Hematoxylin-eosin 150.) |
Conjunctival Melanocytic Nevus: Blue Nevus Variant
A blue nevus may be similar to a typical acquired nevus except that it is located deeper in the stroma and episcleral tissues and it generally lacks cysts. Examples are illustrated.
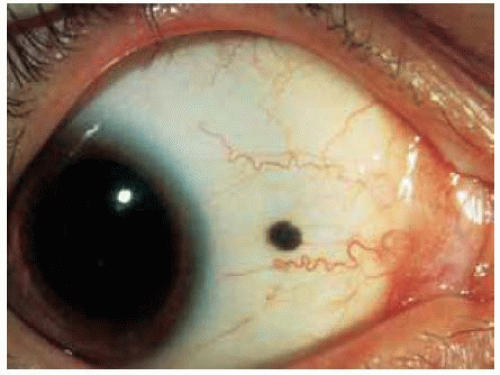 Figure 19.37. Dark episcleral blue nevus in a 45-year-old woman. |
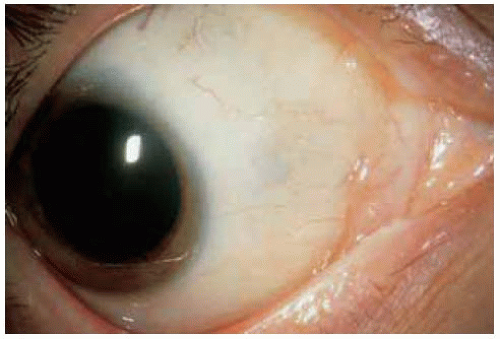 Figure 19.38. Appearance of area shown in Figure 19.37, one year after excision of lesion with no tumor recurrence. |
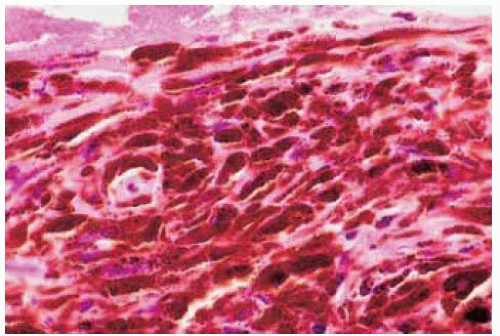 Figure 19.39. Histopathology of same lesion, showing the closely compact deeply pigmented melanocytes. (Hematoxylin-eosin 100.) |
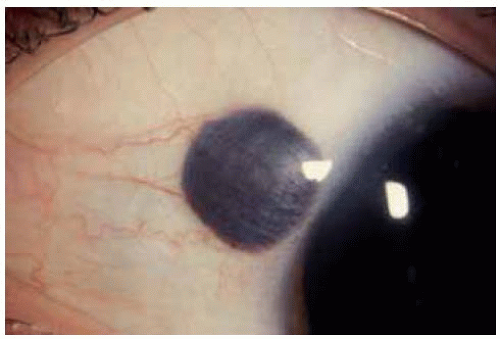 Figure 19.40. Large, ovoid blue nevus superotemporal to limbus. |
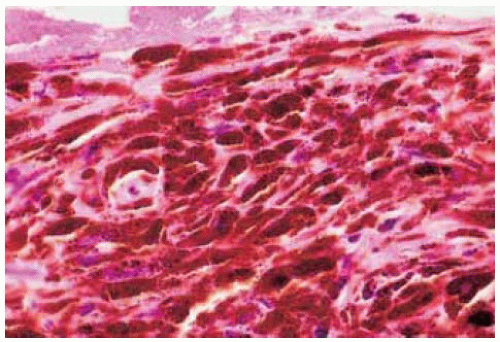 Figure 19.41. Cellular blue nevus located near limbus superiorly in a 38-year-old man. This lesion was more brown than gray, but had histopathologic features of a deep blue nevus. |
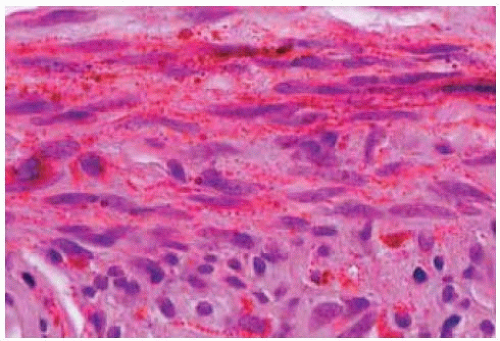 Figure 19.42. Histopathology of lesion shown in Figure 19.41, showing densely packed tumor cells in the stroma. (Hematoxylin-eosin 200.) |
Conjunctival Melanocytic Nevus: Diffuse Atypical Type
Conjunctival nevus can assume a number of atypical clinical variations. The amelanotic diffuse variant can be confused clinically with lymphangioma, lymphoma, and other amelanotic lesions.
Rosenfeld SI, Smith ME. Benign cystic nevus of the conjunctiva. Ophthalmology 1983;90:1459-1461.
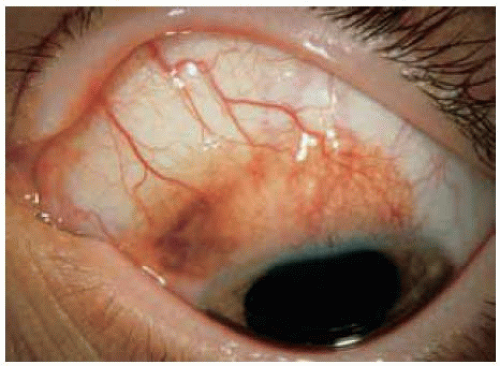 Figure 19.43. Lightly pigmented diffuse nevus near superior limbus in a 13-year-old boy. |
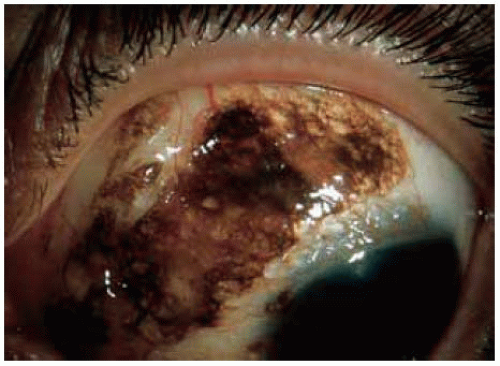 Figure 19.44. Deeply pigmented diffuse nevus superonasally in a 43-year-old man. Note the numerous large cysts that are evident in the lesion. |
 Figure 19.45. Amelanotic diffuse nevus in superior conjunctiva of a 42-year-old man. The thickened lesion actually overhangs the cornea for about 1 to 2 mm, an exceptional finding for a conjunctival nevus. |
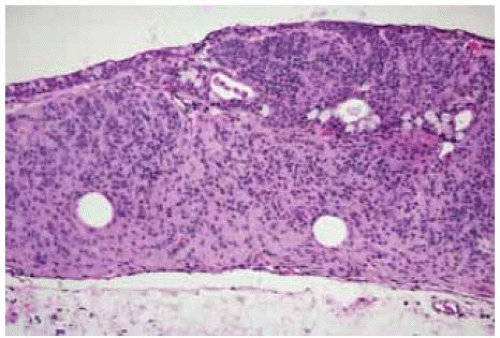 Figure 19.46. Histopathology of lesion shown in Figure 19.45 showing densely packed amelanotic nevus cells, mostly in the stroma, with cystic spaces. (Hematoxylin-eosin 15.) |
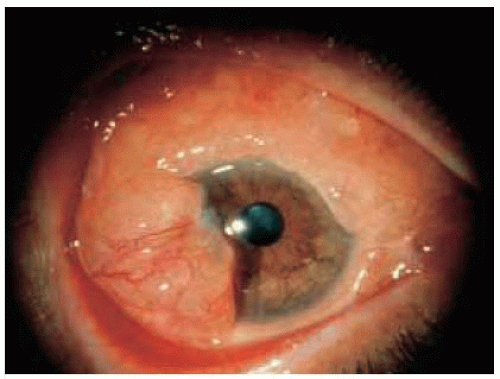 Figure 19.47. Massive amelanotic, cystic nevus in a 51-year-old man. The lesion was similar clinically to a lymphangioma or lymphoma. (Courtesy of Morton Smith, MD.) |
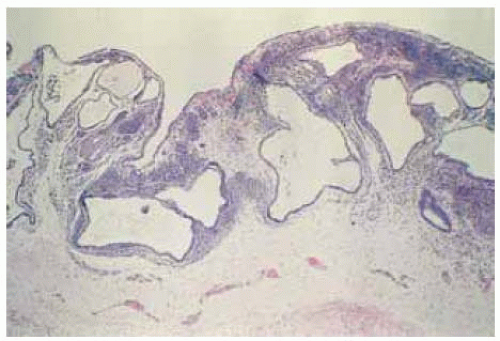 Figure 19.48. Histopathology of lesion in Figure 19.47, showing nevus cells and large, epithelial-lined cystic spaces. (Hematoxylin-eosin 50.) (Courtesy of Morton Smith, MD.) |
Conjunctival Melanocytic Nevus in Non-Caucasians
 Figure 19.49. Facial view of an 8-year-old African American boy with obvious conjunctival nevus temporally in left eye. |
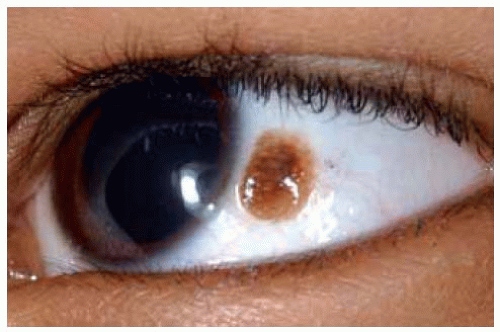 Figure 19.50. Close up view of lesion shown in Figure 19.49 depicting the conjunctival nevus and a trace of racial melanosis at limbus. |
 Figure 19.51. Facial view of 83-year-old African American woman with conjunctival nevus located near semilunar fold in the left eye, as well as bilateral racial melanosis. |
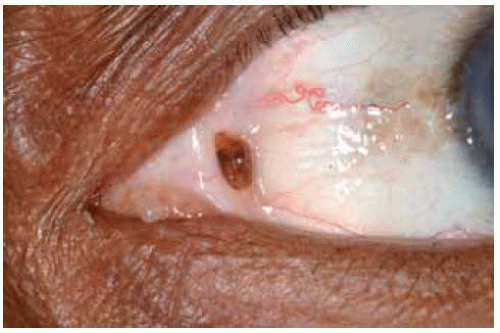 Figure 19.52. Close up view of lesion shown in Figure 19.51. Note the circumscribed nevus at semilunar fold and unrelated racial melanosis near the limbus. |
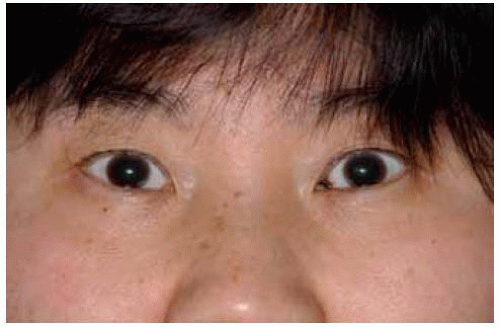 Figure 19.53. Facial view of middle-aged Asian woman with pigmentation in left semilunar fold. |
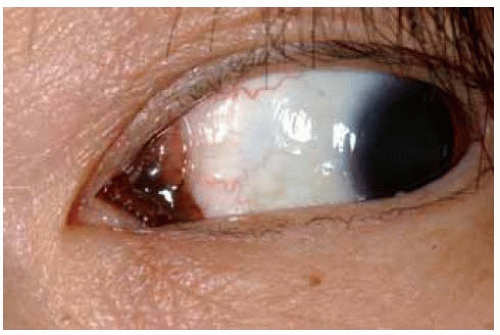 Figure 19.54. Close up view of patient in Figure 19.53 showing involvement of entire semilunar fold. |
Ocular Melanocytosis: Scleral and Episcleral Pigment
General Considerations
Congenital episcleral melanocytosis can occur as a solitary lesion but, in a clinical setting, it is more often seen as a component of ocular melanocytosis or oculodermal melanocytosis (nevus of Ota) (1,2,3,4,5,6,7,8). Oculodermal melanocytosis is discussed under the subject of pigmented lesions of the eyelids. Because of the association of the condition with uveal melanoma, it is also discussed in the Atlas of Intraocular Tumors. It is mentioned here because, although not strictly in the conjunctiva, it is included in the differential diagnosis of conjunctival nevus and primary acquired melanosis (PAM) of the conjunctiva.
Clinical Features
Clinically, the lesions appear as irregular geographic patches of scleral and episcleral pigmentation that can range from distinct brown to gray in color (1,2,3,4,5,6,7). The pigment can be randomly distributed or it can follow a sector distribution, sometimes corresponding to similar sector pigmentation of the uveal tract. Although we have not observed it in our tumor clinic, reports from other facilities have shown that this condition has a 10% incidence of elevated intraocular pressure or true glaucoma, which can occasionally be congenital or late congenital (6,7). Hyperpigmentation of the nasal and buccal mucosa are often associated with oculodermal melanocytosis.
Diagnostic Approaches
The diagnosis can usually be made readily with external ocular examination and slit-lamp biomicroscopy. To help differentiate it from a conjunctival lesion, one can move the conjunctiva with a cotton-tipped applicator. The overlying conjunctiva can be moved over the lesion without distorting it, confirming that it is located deep to the conjunctiva. Fundus examination should be done to exclude uveal melanoma.
Pathology
The scleral and episcleral lesion consists of deeply pigmented dendritic melanocytes with benign cytologic features. In most cases of ocular melanocytosis, the pigmentation involves the sclera and the underlying uveal tract.
Management
No management is necessary for the scleral and episcleral pigmentation of ocular melanocytosis. As mentioned, the patient should be followed for the development of uveal melanoma or secondary glaucoma.
Selected References
1. Zimmerman LE. Melanocytes, melanocytic nevi and melanocytomas. The Jonas S. Friedenwald Memorial Lecture. Invest Ophthalmol 1965;4:11-41.
2. Shields JA, Shields CL. Introduction to melanocytic tumors of the uvea. Congenital ocular melanocytosis. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:46-50.
3. Singh AD, De Potter P, Fijal BA, et al. Lifetime prevalence of uveal melanoma in Caucasian patients with ocular (dermal) melanocytosis. Ophthalmology 1998;105:195-198.
4. Kiratli H, Bilgig S, Satilmis M. Ocular melanocytosis associated with intracranial melanoma. Br J Ophthalmol 1996;80:1025.
5. Kiratli H, Irkec M. Melanocytic glaucoma in a child associated with ocular melanocytosis. J Pediatr Ophthalmol Strabismus 1997;34:380-381.
6. Teekhasaenee C, Ritch R, Rutnin U, et al. Ocular findings in oculodermal melanocytosis. Arch Ophthalmol 1990;108:1114-1120.
7. Teekhasaenee C, Ritch R, Rutnin U, et al. Glaucoma in oculodermal melanocytosis. Ophthalmology 1990;97:562-570.
8. Donoso LA, Shields JA, Nagy RM. Epibulbar lesions simulating extraocular extension of uveal melanomas. Ann Ophthalmol 1982;14:1120-1123.
Scleral Involvement With Congenital Ocular Melanocytosis
The scleral pigmentation of congenital ocular melanocytosis has typical features and location. It must be differentiated from other diffuse epibulbar pigmentary conditions like primary acquired melanosis and complexion-related pigmentation. Unlike these other conditions, it is attached to the sclera and does not move with manipulation of the conjunctiva.
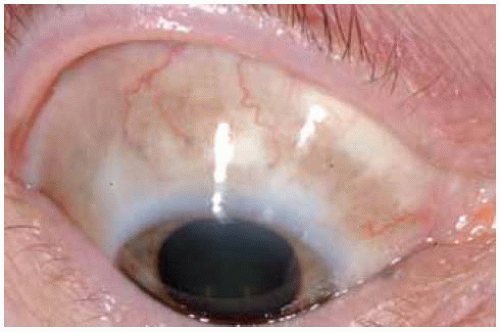 Figure 19.55. Scleral melanocytosis showing diffuse patchy brown pigment in superior aspect of the right eye. |
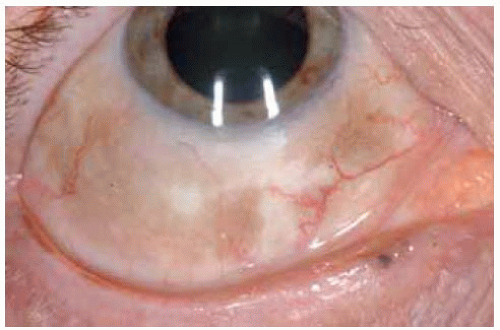 Figure 19.56. Same patient shown in Figure 19.55 demonstrating pigment in the inferior aspect of the right eye. |
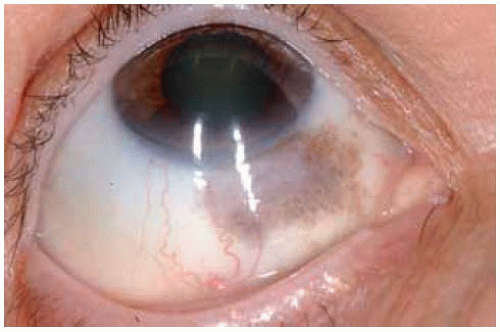 Figure 19.57. Sector scleral melanocytosis inferonasally in the right eye. Note the corresponding sector iris melanocytosis. |
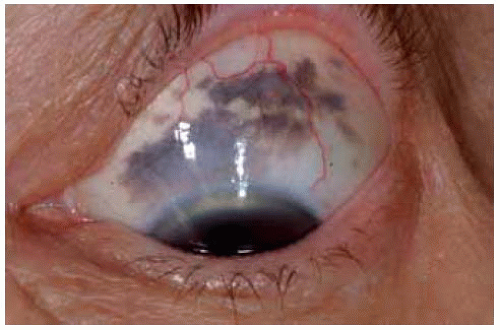 Figure 19.58. Superior melanocytosis in a 60-year-old woman. It was followed for more than 20 years without change. |
 Figure 19.59. Face view of young child with blue-gray discoloration of sclera.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|