Congenital Vascular Lesions
Ravindhra G. Elluru
In 1982, a seminal article authored by Mulliken and Glowacki (1) marked a turning point in the history of classifying and managing congenital vascular lesions, or more properly termed vascular anomalies. These authors developed a classification system in which vascular anomalies were designated as either vascular tumors or vascular malformations, based on their clinical appearance, histopathologic features, and biologic behavior (Fig. 104.1). Hemangiomas were identified as benign tumors that undergo a phase of active growth characterized by endothelial proliferation and hypercellularity, followed by gradual tumor regression that occurs over the first decade of life. In contrast, vascular malformations were described as structural congenital anomalies derived from capillaries, veins, lymphatic vessels, arteries, or a combination of these. Unlike vascular tumors, vascular malformations were shown to have normal levels of endothelial turnover and to grow proportionately with the child. In the chapter to follow, readers will be presented with a description of the most common types of vascular anomalies and available treatment modalities.
VASCULAR TUMORS
Infantile Hemangioma
The most commonly occurring vascular tumor is the infantile hemangioma, affecting 1 in 10 white infants in North America, though less commonly seen in children of African or Asian descent (2). These tumors are more common in females (3:1) and in infants with low birth weight (3). They are typically observed at birth or during the first several weeks of life. Lesions generally present cutaneously in the head and neck (60%), but can involve any anatomic site, including the extremities (15%), visceral organs, and brain (3).
Infantile hemangiomas are clinically characterized as superficial, deep, or combined, depending on their anatomic depth. Superficial lesions are typically soft, red, and raised, whereas deep lesions show a spectrum of appearance and consistency, ranging from soft and supple to raised and firmer warm masses with a bluish hue. Combined lesions have both a red epidermal coloration and a subcutaneous mass that is either blue or flesh colored.
Although most tumors present singularly, up to 20% of affected infants have multiple cutaneous lesions. When a patient has six or more cutaneous hemangiomas, there is an increased risk of having visceral hemangiomas, which in turn can give rise to serious or life-threatening conditions such as hepatomegaly, gastrointestinal bleeding, profound hypothyroidism, anemia, or congestive heart failure (4, 5).
Hemangiomas of infancy generally follow a predetermined clinical course of active growth (proliferation) and later tumor regression (involution); however, there is wide variation in the rate, duration, and degree of growth and spontaneous tumor regression. Proliferation begins during the first few weeks of life and generally continues for 4 to 10 months, though deep lesions may proliferate until 2 years of age. The proliferative phase is followed by a period of quiescence during which the growth rate of the lesion stabilizes. Involution occurs at 12 to 18 months and can last up to 5 to 6 years. During this time, the color of the lesion fades, becoming grayish or dull purple (Fig. 104.2). Clinical studies show that maximum involution occurs in 50% of children by age 5 and in 90% by age 9 (6).
The cosmetic outcome after involution varies considerably and is generally unpredictable. In many patients, involution results in the restoration of normal skin. In others (20% to 40%), residual changes of the skin such as laxity, discoloration, telangiectasia, fibrofatty masses, or scarring are seen in the affected area. Given this unpredictability, for patients who are not at risk, clinical monitoring, parental education, and ongoing support are preferable to early intervention.
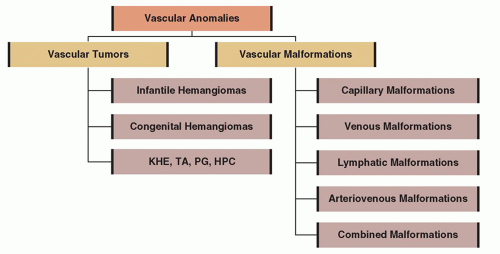 Figure 104.1 A schematic representation of the 1996 ISSVA classification of vascular anomalies. KHE, kaposiform hemangioendothelioma; TA, tufted angioma; PG, pyogenic granuloma; HPC, hemangiopericytoma. |
In the growth phase, infantile hemangiomas are composed of proliferating endothelial cells and large numbers of pericytes, mast cells, and fibroblasts (7). As lesions regress, endothelial cell apoptosis increases and the vascular network is slowly replaced by fibrofatty tissue. Over the past two decades, many studies have investigated possible molecular factors that control this tumor life cycle, and considerable progress has been achieved in understanding the etiology of these lesions. To date, however, no single theory can explain key characteristics of hemangiomas, such as the predilection for females, usual occurrence after birth, spontaneous involution, and abnormal tissue architecture.
Proliferating hemangiomas have been shown to have increased expression of type IV collagenase, vascular endothelial growth factor (VEGF), and basic fibroblast growth factor (bFGF) (8). In involuting hemangiomas, the high expression level of bFGF is maintained, whereas the level of expression of VEGF significantly decreases. Gene expression analysis comparing proliferating versus involuting hemangiomas demonstrates that insulin-like growth factor 2 (IGF-2) is highly expressed during proliferation but is significantly decreased during involution (9).
There is sound evidence that hemangiomas of infancy are related to placental endothelial cells. Four markers of hemangioma cells that are coexpressed in placental vessels have been identified: GLUT1 (a glucose transporter enzyme), merosin, Lewis Y antigen, and Fcγ-RIIb (10). GLUT1 is strongly expressed in infantile hemangiomas, placentas, and the blood-brain barrier; however, it is not expressed in normal surrounding vascular endothelium or in vascular malformations nor is it generally expressed in congenital hemangiomas (see discussion below). Because the positive expression of GLUT1 persists throughout all phases of the hemangioma life cycle, this histochemical marker is particularly useful in distinguishing hemangiomas of infancy from other vascular tumors and from vascular malformations.
Congenital Hemangiomas
Congenital hemangiomas are an uncommon variant of infantile hemangiomas. They differ from infantile hemangiomas in clinical behavior, appearance, and histopathology and are occasionally diagnosed in utero. Unlike infantile hemangiomas, congenital hemangiomas present at birth as fully grown lesions and do not undergo additional postnatal growth. Congenital hemangiomas fall into distinct subgroups: rapidly involuting congenital hemangiomas (RICHs) and noninvoluting congenital hemangiomas (NICHs) (11). RICHs typically involute by 12 to 14 months of age, leaving a residual patch of thin skin with prominent veins and little, if any, subcutaneous fat. NICHs do not undergo involution. Both tumor types have a predilection for the head or limbs. Both tumor types generally present as solitary violaceous lesions at birth and rarely coexist in a patient with a typical infantile hemangioma. Both are high-flow lesions that can be misdiagnosed as arteriovenous malformations (AVMs). In contrast to infantile hemangiomas, congenital hemangiomas are GLUT1 negative and comprise less than 3% of all hemangiomas seen in infancy (12).
Problematic Head and Neck Hemangiomas
Hemangiomas can occur anywhere in the head and neck region. Hemangiomas can occur singularly on the neck, cheek, nose, ears, forehead, or scalp, or multifocally at several of these sites. The head and neck can also be the site of segmental hemangiomas that occupy an entire developmental subunit (Fig. 104.3).
 Figure 104.2 Infantile hemangiomas undergo a process of natural regression. The following series of photographs depict a young girl at (A) 2 months, (B) 6 months, (C) 18 months, and (D) 36 months of age. As the child grows older, the hemangioma changes from a bright red color to a grayish red color, and finally to the natural skin color. The mass of the lesion also decreases, leaving little evidence of the hemangioma over time. |
 Figure 104.3 A series of photographs of children with hemangiomas are presented demonstrating variations in morphology. A: Example of a child with an isolated focal hemangioma. B: Example of a child with multiple cutaneous hemangiomas. C: Example of a child with a facial segmental hemangioma occupying the periorbital, temporal, cheek, and chin areas of the face. Segmental hemangiomas are prone to ulceration as can be seen in this child around the left nasolabial crease. |
Phaces
Hemangiomas that present in developmental segments are referred to as “segmental” lesions. These lesions are less common than focal lesions and have a higher risk of being life- or function-threatening and of having associated structural anomalies. Large cervicofacial segmental hemangiomas, particularly those on the forehead, temple, upper cheek, and around the periorbital area can be accompanied by a constellation of anomalies referred to as PHACES association (13). This association is far more common in females. Accompanying anomalies include posterior fossa brain malformations (e.g., Dandy-Walker malformation), hemangiomas, arterial abnormalities, cardiac and aortic arch defects (e.g., aneurysms and congenital valvular aortic stenosis), eye abnormalities (e.g., congenital cataract, microphthalmia, and abnormal retinal vessels), and sternal clefts or supraumbilical raphes. More than 50% of patients are affected by neurologic sequelae, including seizures, stroke, developmental delay, and migraines (14).
Segmental hemangiomas are plaque-like in contour, typically undergo an extended proliferative period of 18 months, and unlike most hemangiomas of infancy, they do not completely regress. Furthermore, segmental hemangiomas are at a higher risk of ulceration and residual scarring (13). When there is an index of suspicion for PHACES association, referral should be made for an ophthalmologic and neurologic examination, screening echocardiogram, and possibly a magnetic resonance imaging (MRI) or magnetic resonance angiography (MRA) of the head, neck, and chest. Patients in whom imaging reveals
a central nervous system abnormality should be closely monitored. The frequency of repeated imaging depends on symptom presentation and disease progression.
a central nervous system abnormality should be closely monitored. The frequency of repeated imaging depends on symptom presentation and disease progression.
Hemangiomas in a Beard Distribution
Sixty-five percent of patients with hemangiomas that occur in a beard distribution (i.e., the chin, jawline, and preauricular areas) have associated airway involvement (15), and most airway hemangiomas are localized in the supraglottic or subglottic region. Patients must be closely followed and treatment should be initiated when airway involvement is suspected. Localized lesions are managed with laser ablation, intralesional steroids, surgical resection, or medical therapy (see below). Tracheotomy placement is used only in refractory cases or in cases in which the airway hemangioma is extensive. Hemangiomas that occur in the beard distribution often involve the parotid glands. Parotid gland hemangiomas typically occupy the entire gland and adjacent parapharyngeal space. They grow rapidly, causing extrinsic compression of the upper pharyngeal airway. These lesions frequently have a prolonged proliferative phase (12 to 16 months) and may require systemic therapy if the airway is compromised (16). Children with extensive hemangioma of the parotid region and pharyngeal area often have chronic recurrent otitis media, likely secondary to extrinsic compression of the eustachian tube.
Periocular Hemangiomas
Periocular hemangiomas can involve the upper lid, lower lid, and/or the retrobulbar space (Fig. 104.4). Pressure from the hemangioma on the globe may lead to astigmatism and amblyopia. Early ophthalmologic evaluation and treatment is indicated for all cases of periocular hemangiomas to avoid deprivation amblyopia, which can occur with as little as 1 week of deprivation during key developmental periods. Treatment options for vision-obstructing periocular hemangiomas include either medical therapy or surgical excision. Children older than age 1 who have gone untreated have rates of deprivation amblyopia as high as 75%.
 Figure 104.4 An axial cut through the orbit of a child with a right pre- and postseptal orbital hemangioma. |
Nose, Lip, and Ear Hemangiomas
Hemangiomas involving the nose occur in close to 16% of facial hemangiomas (17). Proliferation of lesions on the nasal tip often distort the anatomy of the nose, causing misalignment of the nasal cartilages and mild to severe nasal volume increase. Management approaches must consider the depth, location, rate of involution, and functional and cosmetic disturbance caused by the lesion. A multimodal approach combining serial observation, intralesional steroid injection, systemic steroid therapy, pulsed-dye laser (PDL) treatment, and surgical intervention is generally used (18). In view of possible complications such as severe cutaneous infiltration, the consequences on nasal growth, and the psychological impact of nasal distortion, surgical excision before school age is currently recommended. Various surgical techniques have been reported (19).
Lesions of the pinna of the ear can deform normal anatomic structures and result in ulceration with focal destruction of the auricle. Lesions obstructing the auditory canal can cause temporary conductive hearing loss. Lip lesions frequently involute slowly, sometimes leaving residual skin changes. Additionally, lip ulcerations can result in feeding difficulties, secondary infection, and significant scarring.
Subglottic Hemangiomas
Hemangiomas can occur anywhere within the tracheobronchial tree; however, they are most commonly seen in the subglottis (Fig. 104.5). As mentioned above, there is a close association of hemangiomas in a beard distribution with airway hemangiomas. However, airway hemangiomas can occur without associated cutaneous hemangiomas. In fact, only 50% of patients with airway hemangiomas have cutaneous hemangiomas (20). Presentation usually occurs within the first 6 months of life, and the earlier the presentation, the greater the likelihood that patients will require surgical intervention. Symptoms typically include progressive stridor and retractions. The diagnosis is made on rigid bronchoscopy, and though radiologic evaluation (MRI with contrast enhancement) is indicated, it rarely demonstrates extension of the lesion beyond the confines of the subglottis. Lesions are typically asymmetric and usually covered by a normal smooth mucosa.
Open surgical excision is an option in large focal hemangiomas of the subglottis and is accomplished through a vertical tracheotomy extending through the cricoid ring. Typically, a thyroid alar graft is needed to augment the concomitant narrow subglottis (20). Although many other treatment modalities (systemic steroids, intralesional steroids, prolonged intubation, CO2 [carbon dioxide] and KTP [potassium-titanyl-phosphate] laser ablation, and microdebrider resection) have been used, these modalities carry a significant risk of inducing an acquired or congenital subglottic stenosis (20). Medical management as discussed below is also an option in selected cases.
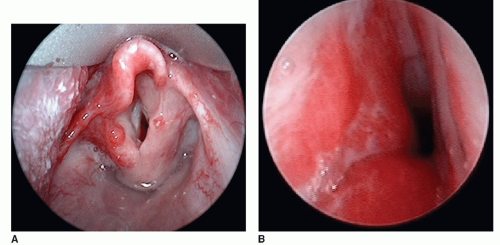 Figure 104.5 Endoscopic photographs of (A) a child with flat supraglottic hemangiomas occupying the left epiglottis and aryepiglottic fold and (B) a child with a large left subglottic hemangioma that severely narrows the subglottic lumen. |
KASABACH-MERRITT PHENOMENON
Kasabach-Merritt phenomenon is a rare, life-threatening condition associated with two specific subtypes of vascular tumors, tufted angioma or kaposiform hemangioendothelioma. Kasabach-Merritt phenomenon is included in this section only to highlight the fact that it is not associated with infantile hemangiomas, as sometimes construed. In Kasabach-Merritt phenomenon, the tumor traps and destroys platelets. In addition to platelet trapping, there are also other associated coagulopathies. As the tumor grows, it causes more platelet trapping. No single treatment approach is effective and unfortunately, responses to various treatments are inconsistent. Initially, corticosteroids are given at varying doses. If this approach is not effective, chemotherapy with vincristine is started. If this regimen is not effective, other drugs such as interferon, Cytoxan, and Amicar are used. If the tumor does not respond to drug therapy, embolization, surgical removal, or both may be necessary. Blood products such as platelets and packed red blood cells are administered only if absolutely necessary. The lesion may take many years to decrease in size. Improvement in platelet counts initially occurs with a decrease in the size of the lesion.
DIAGNOSTIC EVALUATION OF INFANTILE HEMANGIOMAS
The diagnosis of infantile hemangiomas is generally established on the basis of clinical presentation, history, and physical examination. In patients with complex lesions that require surgical intervention, additional investigations can be helpful in determining the extent of involvement. Ultrasound (US) with color flow Doppler can be extremely useful in differentiating hemangiomas from vascular malformations that may have a similar appearance. On US, an infantile hemangioma appears hypoechoic, well defined, and heterogeneous in texture, with small cystic and sinusoidal spaces. In most proliferating hemangiomas, a characteristic fast-flow pattern is visualized by Doppler US. Typically, a quick upstroke and gradual down slope is seen (Fig. 104.6).
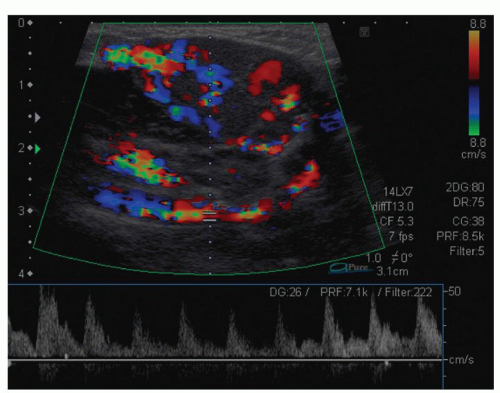 Figure 104.6 Color ultrasound Doppler image of an infantile hemangioma. Infantile hemangiomas are composed of small blood vessels conducting blood at high flow rates (top panel). Doppler demonstrates that the blood flow in these small blood vessels is pulsatile, characterized by a rapid upstroke and a gradual down stroke in flow rates (bottom panel). |
TABLE 104.1 MRI CHARACTERISTICS OF VASCULAR ANOMALIES | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|



