The nose is a prominent feature of the human face. Congenital malformations of the nose, whether functional or anatomic, affect the physiologic and psychologic wellness of children who have these anomalies. Congenital nasal abnormalities may be overt or subtle and can occasionally cause life-threatening emergencies at birth. A discussion of nasal embryology and development provides the basis for the discussion of some of the important congenital abnormalities seen in clinical practice. The final portion of the article is devoted to several of the more common syndromes in which nasal abnormalities are encountered.
Nasal embryology
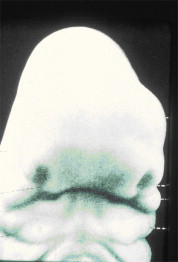
External nose formation begins when the embryonic stomodeum appears during the fourth and fifth weeks of gestation, delineating the center of the face. The stomodeum is surrounded by the maxillary, mandibular, and frontal prominences . On the lateral aspects of the frontal prominence, neural crest cells proliferate and form the nasal placodes. The nasal placodes invaginate to form the olfactory pit, which further invaginates to form the nasal processes ( Fig. 1 ).
Forming on the outer edge of the pits are the lateral nasal processes. Those on the inner side are the medial nasal processes . The lateral rounded angles of the medial prominences are the globular processes. The globular processes continue ( Figs. 2–4 ) posteriorly as plates termed the nasal laminae . The nasal laminae fuse with the nasofrontal process in an anterior to posterior direction, creating the nasal septum and initially partitioning the nasal cavity into left and right divisions . The nasal septum continues to grow posteriorly and begins fusion with the palatine processes during the ninth week of gestation. Chondrification and ossification begin around the twelfth week, but ossification does not fully complete until puberty .
The globular processes of the medial prominences then fuse with the maxillary processes, forming the philtrum and the columella. The maxillary processes also give rise to the lower portion of the lateral walls of the nasal cavity and the posterior borders of the nares. The nares are initially filled with epithelium, which eventually breaks down by the 24th week, leading to the permanent openings ( Fig. 5 ) .
Ectoderm of the nasal sac contacts ectoderm of the roof of the mouth, forming the oronasal septum. Attenuation of this septum leads to creation of the oronasal membrane separating the nasal cavity from the pharynx. The oronasal membrane then undergoes degeneration, forming the choanae. Beginning at 6.5 weeks, lateral nasal wall development occurs. The inferior concha appears above the palatine processes. As the nasal cavity heightens, ectodermal folds appear in the ethmoid region and give rise to superior, middle, and inferior conchae ( Fig. 6 ) .
Nasal cleft deformities
Nasal cleft deformities include nasal clefting, cleft lip, and cleft palate. Cleft lip and palate are addressed elsewhere in this issue. This section discusses nasal cleft defects, associated esthetic and airflow complications, and the repair of these malformations.
Nasal defects associated with cleft lip and palate
Nasal deformities are commonly seen in children who have cleft lip. In general, the worse the cleft lip, the worse the nasal deformity . According to facial development theories, cleft palate begins to occur at 35 days’ gestation, leading to nasal septal deviation. The nasal defects can be unilateral or bilateral. In unilateral cleft, the premaxilla and maxilla tethers the septum, causing it to deviate. As embryogenesis continues, maxillary growth is also hindered by the tethered septum, leading to maxillary hypoplasia in the caudal-cranial and anterior-posterior directions .
When a cleft lip is unilateral, the medial nasal crus is medially and inferiorly rotated. Due to the maxillary bone hypoplasia, the nasal ala is retrodisplaced and the nostril is flat and flared. The nasal tip may appear uneven, wide, or boxy. The bases of the nares are widened, and the caudal septum and nasal spine are deviated to the nonaffected part of the nose. When a bilateral cleft defect is present, all the previously mentioned defects are present, along with a shortened columella and a relative prognathism due the bilaterally hypoplastic maxilla . In some patients, the floor of the nasal cavity is absent .
Controversy surrounds the most appropriate timing of correction of cleft lip and nose deformities. At times, it may be beneficial to delay correction until facial growth is complete and nasal structures have fully matured. When the deformity is causing inadequate airflow and respiratory distress, however, the defect should be repaired earlier . Because neonates are preferential nose breathers, early repair is often indicated .
Nasal cleft deformities
Nasal cleft deformities include nasal clefting, cleft lip, and cleft palate. Cleft lip and palate are addressed elsewhere in this issue. This section discusses nasal cleft defects, associated esthetic and airflow complications, and the repair of these malformations.
Nasal defects associated with cleft lip and palate
Nasal deformities are commonly seen in children who have cleft lip. In general, the worse the cleft lip, the worse the nasal deformity . According to facial development theories, cleft palate begins to occur at 35 days’ gestation, leading to nasal septal deviation. The nasal defects can be unilateral or bilateral. In unilateral cleft, the premaxilla and maxilla tethers the septum, causing it to deviate. As embryogenesis continues, maxillary growth is also hindered by the tethered septum, leading to maxillary hypoplasia in the caudal-cranial and anterior-posterior directions .
When a cleft lip is unilateral, the medial nasal crus is medially and inferiorly rotated. Due to the maxillary bone hypoplasia, the nasal ala is retrodisplaced and the nostril is flat and flared. The nasal tip may appear uneven, wide, or boxy. The bases of the nares are widened, and the caudal septum and nasal spine are deviated to the nonaffected part of the nose. When a bilateral cleft defect is present, all the previously mentioned defects are present, along with a shortened columella and a relative prognathism due the bilaterally hypoplastic maxilla . In some patients, the floor of the nasal cavity is absent .
Controversy surrounds the most appropriate timing of correction of cleft lip and nose deformities. At times, it may be beneficial to delay correction until facial growth is complete and nasal structures have fully matured. When the deformity is causing inadequate airflow and respiratory distress, however, the defect should be repaired earlier . Because neonates are preferential nose breathers, early repair is often indicated .
Piriform aperture stenosis
Piriform aperture stenosis (PAS) is rare and subtle. Thus, it often overlooked as a cause of respiratory distress in neonates. PAS results from bony overgrowth of the nasal process of the maxilla, narrowing the anterior bony opening of the nose. This narrowing can cause increased nasal resistance and cyclic cyanotic periods . The disorder usually presents in the initial few months of life. It may occur alone or in association with holoprosencephaly. A solitary maxillary central incisor may serve as a clue that additional significant abnormalities of the midface, orbits, and brain are present ( Fig. 7 ) .

PAS is often found incidentally on intranasal examination. Axial CT is helpful in differentiating PAS from choanal atresia, demonstrating anterior bony nasal stenosis ( Fig. 8 ) . The differential diagnosis of anterior nasal obstruction includes nasal mucosa edema, obstruction of the nasal passage by a nasolacrimal duct cyst, or hypoplasia of the nasal alae .
Respiratory distress from PAS can be managed using an oral airway or a McGovern nipple, supplemented by humidified oxygen and nasal decongestants. Mild stenosis improves with growth and may never require surgery. When a neurologic deficit is suspected, MRI can help to rule out associated structural brain defects . The neonate may be discharged from the hospital when an artificial airway is no longer needed and oral intake is adequate . Respiratory status should be carefully monitored.
Surgery is indicated for persistent respiratory distress with cyanosis or apnea, or with poor feeding . Repair is performed using a sublabial approach to the premaxilla. The narrowed nasal aperture is enlarged by submucosal drill-out of the nasal process of the maxilla. Care must be taken to preserve the nasolacrimal ducts and forming teeth . Nasal stenting is usually employed for 1 to 6 weeks to prevent recurrent stenosis . Extended postoperative follow-up is necessary to look for restenosis.
Nasal dermoid cysts
Midline congenital lesions of the nose are rare, affecting 1:20,000 to 1:40,000 newborns . Nasal dermoid cysts are the most common of these congenital midline nasal defects and may present as noncompressible masses over the nasal dorsum with an associated midline pit. These cysts often present at birth or in early childhood. Masses and pits may appear anywhere from the glabella to the nasal columella. Sixty percent are located on the lower nasal dorsum. Thirty percent are intranasal and 10% are combined. Usually, nasal dermoids terminate in a single subcutaneous tract with hair at the opening. They may secrete sebaceous material or pus, if inflamed. They may cause recurrent septal abscesses or osteomyelitis or broaden the nasal root. With intracranial extension, infected nasal dermoids may lead to meningitis or brain abscess ( Figs. 9 and 10 ) .



